

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Acute myocardial infarction (AMI) is a key component of the burden of cardiovascular disease, and is a very frequent cause of mortality and disability around the world [1]. It is defined by myocardial necrosis resulting from a dynamic process associated with inadequate coronary blood flow [2]. Almost 550,000 first episodes and 200,000 recurrent episodes of AMI occur every year, imposing large socio-economic burdens on healthcare systems [3]. The management of AMI has been improved over the past three decades, but remains a leading cause of death. Strategies are needed to prevent or decrease the progress of the disease [4]. Coronary atherosclerosis plays a pivotal part in the pathogenesis of AMI in many patients [5]. In this regard, many researchers have investigated and suggested that the following play major roles in the occurrence of atherosclerotic cardiovascular disease: diet, physical activity, smoking, or psychosocial stress [678]. This evidence implies that AMI might be largely preventable by adhering to specific diets [9], therefore gaining improved knowledge about the effects of each dietary component can be a critical step toward AMI prevention.
According to the food pyramid presented by the United States Department of Agriculture (USDA), the meat group (including red meat, poultry, fish, eggs, beans, and nuts) is the primary source of protein, and supplies substantial amounts of phosphorous, magnesium, iron, thiamine, niacin, vitamin B6, and vitamin B12 for daily needs [10]. The effect of each source of protein on cardiovascular health is different due to its ingredients [11]. Red and processed meat are sources of saturated fatty acid and cholesterol, which have been shown to be risk factors for atherosclerosis [1213]. On the other hand, fish and nuts provide unsaturated fatty acid and minerals, which have been established as cardio-protective components [1415]. The investigation into the relationships between dietary items and cardiovascular risk factors is not a new interest, with several studies on the subject from the United States [161718], as well as European countries [192021]. However, the available information reporting on these associations among Asian countries is low [2223]. Also, there are many papers examining single-nutrient associations with the risk of atherosclerotic cardiovascular disease, although health recommendations can be more easily provided to patients when they are based on foods. Therefore, the present study was conducted to clarify the associations between the frequency of meat group item intakes on the manifestation of AMI in an adult Iranian population.
MATERIALS AND METHODS
This hospital-based case-control study was conducted in Heshmat Hospital in Guilan, Iran, in 2017. Two hundred coronary care unit patients who had suffered their first AMI, and 200 healthy individual without any history of heart disease or exertional chest pain were included in this study. Case and control groups were matched based on age (plus or minus 5 years), sex, and body mass index (BMI). Inclusion criteria for cases were cases of first myocardial infraction (diagnosed by physician), age > 30, and BMI between 25–30. The subjects were excluded if they were unable to respond to questions, were undergoing a systematic period of treatment by steroids, following a special dietary pattern, malnourished, of suffering from any other chronic disease including chronic liver cirrhosis, thyroid disease, gastrointestinal-related disease, renal failure, chronic inflammatory disease, cancer, pulmonary disease, and chronic infections such as human immunodeficiency viruses and hepatitis. Participants who did not respond to more than 35 food items in the food frequency questionnaire (FFQ), provided incomplete demographic data, or whose total amount of energy consumed lay outside the range of 800–4,200 kcal were also excluded. The same exclusion criteria for AMI cases were applied to the control group. Written informed consent was obtained from all recruited participants. This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by the ethics committee of Guilan University of Medical Sciences (Ethical approval No. IR.GUMS.REC.1396.399).
Questionnaires and interview
After explaining the purpose of the study to each participant and obtaining formal written consent, a structured questionnaire was completed by a researcher through a face-to-face interview. The questionnaire consisted of information on demographic data, anthropometric measurements, physical activity, and the FFQ. Each interview lasted nearly 30 minutes, in which the structured questionnaire was completed.
Assessment of demographic information
At the beginning of the interview, the researcher asked about the demographic and lifestyle characteristics of the subjects, including age, sex, education level (illiterate, elementary, high school, diploma, and university), marital status (single, married, widow, and divorced), occupational status (employed, unemployed, and retired), smoking status, alcohol consumption, opioid drug intake, body weight, and waist circumference measurements.
Assessment of physical activity
The physical activity of the participants was assessed by the short form of the International Physical Activity Questionnaire [24].
The daily physical activity of each subject was calculated based on metabolic equivalent for task, number of days per week, and amount of time in minutes per day.
Assessment of dietary intakes
An FFQ validated for Iranian populations was used to assess usual dietary intakes over the past year [25]. The FFQ was a semi-quantitative questionnaire consisting of a list of 168 food items from 6 food groups. All questionnaires were completed by a trained dietitian. Participants were asked to report their frequency of a given serving of each food item consumption according to intake per day, week, month, and year. All food items were categorized into main food groups based on the food pyramid suggested by the USDA's Food Guide Pyramid [26]. At the end, data of the meat group consumption (including meat [red and processed], fish, poultry, eggs, nuts, and legumes) was extracted.
Anthropometric measurements
Participants' body weight was measured to the nearest 0.1 kg by Seca scale (Seca, Hamburg, Germany), while participants were wearing light clothes and no shoes. The height of subjects was recorded using a tape in a normal position, based on standard protocols by the World Health Organization [27]. BMI was calculated by weight (kg) divided by height (m2).
Statistical analysis
Data was analyzed by SPSS software version 21 (IBM Corp., Armonk, NY, USA). The Kolmogorov-Smirnov test was used to determine the normal distribution of variables. To detect the difference between general characteristics of case and control, Independent t-test and χ2 test were applied for continuous and categorical variables, respectively. The associations between meat group items and AMI were calculated by multivariable logistic regression. These associations were determined in both the crude and adjusted models. The p value < 0.05 was considered to be statistically significant.
RESULTS
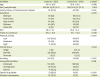
Table 1 demonstrates the characteristics of the participants according to case-control status. A total of 400 participants with a mean age of 53 years old were recruited (200 with AMI and 200 healthy controls). There were no significant differences between the 2 groups in terms of age, sex, BMI (as this was the protocol of the study), waist circumstance, educational, marital and occupational status, while physical activity was significantly higher among patients with AMI than in the control group. In addition, cases reported having higher alcohol consumption, opioid drug intake and smoking habits, in contrast to the control group.
Table 1
Characteristics of patients with acute myocardial infraction and control subjects
Based on the unadjusted results, no significant association was observed between the frequency of consumption of processed and white meat, fish, egg, nuts and beans, and the presence of AMI. However, the results showed a positive association between red meat intake and the risk of AMI. In particular, the frequency of red meat intake in the case group was marginally higher than in the control group (Table 2). The association between the frequency of meat group consumption and the risk of AMI are presented in 3 adjusted models in Table 3. In model 1, age, sex, and BMI were added. No significant association was found in adjusted model 1. After additional adjustment for physical activity, a significant association was observed between both processed and red meat consumption, and the risk of AMI (processed meat consumption: odds ratio [OR], 1.71; 95% confidence interval [CI], 1.31–2.23 and red meat consumption: OR, 2.51; 95% CI, 1.84–5.11). These associations were attenuated, and remained significant in further controlling for more confounders including opioid drug intake, alcohol consumption and smoking habit (processed meat consumption: OR, 2.87; 95% CI, 2.00–3.95 and red meat consumption: OR, 2.81; 95% CI, 2.65–4.12). In addition, an inverse association between nuts intake and AMI risk was seen in the model 3 adjustment (nuts consumption: OR, 0.52; 95% CI, 0.31–0.92).
Table 2
Distribution of frequencies of meat group consumption between AMI patients and controls

Table 3
Results from multiple logistic regression models that were performed to assess the association of meat consumption with the risk of AMI
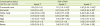
Results are presented as OR and 95% CI and calculated by performing multiple logistic regressions.
AMI = acute myocardial infraction; BMI = body mass index; OR = odds ratio; CI = confidence interval.
*Adjusted for age, sex, and BMI; †Adjusted for age, sex, BMI, and physical activity; ‡Adjusted for age, sex, BMI, physical activity, opioid drug intake, alcohol consumption and smoking habit; §p value < 0.05.
DISCUSSION
This case-control study was carried out to investigate the associations between the frequency of meat group items consumption and the risk of AMI, and demonstrated that red meat consumption might be associated with increased AMI risks. After controlling for potential confounding risk factors, the results indicated a positive association between processed and red meat intake, and risk of AMI. Furthermore, an inverse relationship was observed between frequency of nut intake and the odds of AMI.
This study's finding that processed and red meat intake are related with higher AMI risk is in line with several other studies [28]. Yang et al. [29] showed that high consumption of red meat can increase the risk of total and ischemic stroke. Another study suggested that an increase in consumption of processed meat for each one serving per day is associated with 15% increased risk of cardiovascular mortality [30]. Also, it was demonstrated that the risk of stroke increased by 11% and 13% for each 100 g/day increase in red meat and 50 g/day increase in processed meat consumption [31]. The key link for this association might be related to its high saturated fatty acid and cholesterol content [32]. Also, gut bacteria can metabolize L-carnitine, which is derived from red meat ingestion, and thus produce pro-atherosclerotic compounds [33]. In addition to the aforementioned constituents in red meat, processed meat contains 400% more sodium and 50% more nitrates, which can elevate blood pressure and stimulate peripheral vascular resistance that leads to arterial compliance impairment [2834].
No association between poultry, fish, egg, and beans intakes and the risk of AMI was found. In contrast with our findings, growing evidence has indicated fish intake is associated with lower AMI incidence [353637]. The reason underlying this inconsistency may be related to the species of fish which the participants consumed. One study suggested that fatty fish intake was associated with lower risk of AMI, whereas lean fish was not associated with AMI [38]. Generally, participants of the present study more often consumed Caspian Sea fish, which are categorized as lean fish. The cardio-protective effect of fish intake is proposed as relating to its unsaturated fatty acid content, including eicosapentaenoic acid and docosahexaenoic acid. These polyunsaturated acids can stimulate prostaglandin I3, which acts as a vasodilator and reduces the formation of thromboxane A2 in platelets, which leads to decreased platelet aggregation with no adverse effect on vasodilation [3940]. In addition, fish oil can reduce blood pressure in hypertensive individuals via reducing plasma fibrinogen concentrations [41]. Similar to the present study's results, previous studies did not detect any association between egg consumption and the risk of stroke [424344]. Fish, beans and eggs are very common food items and are used as a main dietary constituent among people in the north of Iran. It seems that there is no direct connection between the incidence of AMI and the usual volume of fish, eggs, and beans consumption.
An inverse association was found between nuts intake and the risks of AMI, after adjusting for potential confounders. A previous study demonstrated that nuts intake of 3 or more times a week reduced the risk of atrial fibrillation by 18%, as well as the risk of heart failure [45]. Another study showed that individuals who consumed nuts more than 4 times per week had a 37% lower risk of coronary heart disease in comparison to non-consumers [46]. Increasing evidence has indicated that nuts consumption may confer cardiovascular protection through bioactive constituents, including unsaturated fatty acids, L-arginine, minerals, vitamin E, folate, phenolics, and phytosterols [47]. It can modify blood lipid levels [48], improve endothelial function [49] and reduce inflammation [50].
There are several limitations that should be considered when interpreting our findings. First, the assessment of dietary intakes by using self-administered FFQ might lead to misclassifications among the study participants. Second, it is possible that there was residual confounding—for example other food group components and stimulant drugs, which could not be detected or/and excluded, and may be confounders in the relationship between the frequency of meat group items intake and the risk of AMI, thus influencing the results. However, multivariable logistic regression was performed to adjust for a number of potential confounders. Third, the present study had a case-control design, so, similar to other observational studies, no causal inference between the frequency of meat group consumption and AMI can be drawn. In this case, it was not possible to clarify whether frequency of meat group items intake modifies the risk of AMI or whether AMI affects food preferences. Finally, due to its small sample size, these findings cannot be generalized to the general population.
CONCLUSION
In conclusion, the study findings suggested a positive association between AMI and processed and red meat consumption. In addition, the present study provides evidence for an inverse association between nuts intake and the risk of AMI. Although these findings imply promising associations which may provide a new approach to manage AMI, due to the nature of observational studies, they cannot be generalized to the wider population and cannot be used to determine causality. Long-term prospective cohort studies are recommended to provide more epidemiological evidence and to present detailed information about the associations between AMI and meat group items intake.
 XML Download
XML Download