

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The metabolic syndrome (MetS) is a complex of metabolic risk factors that may result in chronic diseases [1]. Presence of MetS is back to many years ago, but the new form of that have started with description by Reaven in 1980 [2]. Definition of MetS by The National Cholesterol Education Panel-Adult Treatment Panel III (NCEP-ATP III) includes the presence of obesity, dyslipidemia, the elevation of arterial blood pressure (BP) and glucose intolerance [3].MetS can lead to diabetes mellitus, cardiovascular disease (CVD), stroke and even cancers [456]. Based on studies, the prevalence of MetS varies worldwide and within Iran [78], so some regions of Iran have a slightly high prevalence (more than 25%) [910]. The cause of MetS has not revealed clearly; however, genetic, metabolic and environmental factors can play an important role in etiology of MetS [1112].
Complementary therapies have existed for many years in different parts of the world; but, the standard herbal medicine has been started in the recent decade and considered as a new challenge to preventing and treatment of diseases such as MetS, CVD, and diabetes mellitus [13]. Today, several communities give more attention to plants as a care option for diseases because of their lower side effects. Nigella sativa (N. sativa) or black seed (belongs to the family of Ranunculaceae) has been used for health promotion and diseases management for many years especially in Asian countries [14] due to its therapeutic characteristics [15]. The curing properties of N. sativa are originated from several components including proteins, amino acids, carbohydrates, fibers, oils (especially polyunsaturated fatty acids), volatile oil (including thymoquinone), mineral, alkaloids, flavonoids, and etc. [16].
Effects of a different form of N. sativa on clinical parameters were assessed in many studies. Blood glucose is one of the most important metabolic parameters in MetS. The effects of N. sativa on blood glucose have been controversial in chronic diseases because these effects were significant in some studies, but not in the other studies [1718]. The effect of N. sativa on BP has been also evaluated in a lot of studies, but the effect varied among studies. In one study, N. sativa reduced BP in patients with MetS [19] but this effect was not significant in menopausal women with MetS [20]. Anthropometric indices are also important parameters in predicting the risk of chronic diseases. The effects of N. sativa on anthropometric parameters were not equivalent among studies because it could reduce weight, waist circumference (WC), and BMI in obese men [21], but no in MetS patients [22].
Since most previous studies used N. sativa as a pharmacological supplement, this study will evaluate the effects of N. sativa, as a form of traditional bread, on blood glucose, BP and anthropometric indices in patients with MetS.
MATERIALS AND METHODS
Total of 54 MetS patients (male and female) with age group of 20–65 years old participated in a cross-over, double-blind, randomized clinical trial in Chalus, north region of Iran. Our project has been approved by medical Ethics Committee of Isfahan University of Medical Sciences. This clinical trial has been registered in Iranian Registry of Clinical Trials with registration number IRCT2015041821815N1. Subjects were collected according to the data from several laboratories and general recalling. Definition of NCEP-ATP III was the diagnosis criteria of MetS for subjects.
Inclusion criteria
Study design
In the beginning, subjects were selected based on inclusion criteria of this study. So, 54 subjects with MetS participated in the study and enrolled to Faculty of Medical Science, Azad University of Chalus. Aims of the survey were informed to all of the patients and consent forms were received from all study participants. Information of subjects such as age, sex, physical activity level, telephone, address, and other characteristics such as the suffering of diseases, use of drug and family medical history were recorded in a questionnaire. For analyzing unusual dietary intake, we evaluated 3 days of dietary food records (a weekend and 2-weekdays) in subjects. Subjects who used herbal therapy or consumed energy less than 1,200 kcal or more than 4,000 kcal, were excluded from the study.
Also, a nutritionally-balanced sample diet was served to each subject according to nutritional requirement till subjects follow a standard test diet. Daily energy requirements for subjects were calculated by the formula suggested by the Institute of Medicine, Food and Nutrition Board [23]. Furthermore, subjects were informed not to change their diet and physical activity level during the study procedure.
Study participants were divided into 2 groups by regular randomization (group A, n = 27 and group B, n = 27). Based on cross-over study, 1 group (for example A) was assigned as intervention group and the other (B) as a control group in phase 1. Subjects in both groups were placed in a washout period and then, in phase 2, group assignment was switched to the other group. In phase 1, group A received daily 100 g of bread with N. sativa and group B received the same bread without N. sativa for 2 months. Giving of pieces of bread to patients was down weekly. After 2 months, the washout period was placed for 2 weeks. Then, phase 2 begun with replacing of groups as group B could consume daily bread with N. sativa and group A could consume bread without that for 2 months. Also, it was carefully watched that patients consumed bread regularly and did not miss it.
For establishing double-blind status in the study, a third person was employed and informed about study groups and type of bread. So, the third personnel gave bread to patients without informing of researchers and subjects. Although, 2 types of bread have almost the same shape.
Bread preparation
The N. sativa (black seed) were bought from the traditional herbal shop. Then, seeds were sorted, grinded and the powder of black seed was delivered to a local bakery. Two types of 100 g massive bread have been considered for this study: a bread which includes 3 g powder of black seed and 3 g wheat bran (for the intervention group) and the other includes only 3 g wheat bran and without black seed (for the control group). These bread were produced by high quality materials and under hygiene situation with the supervision of researcher. After the baking was completed, bread was gradually cooled and put in the package. Nutrient composition of 2 types of bread was analyzed in food laboratory in the School of Nutrition & Food Science, Isfahan University of Medical Sciences and was summarized in Table 1. According to this table, there was much difference in the fat content of 2 types of bread due to high polyunsaturated fatty acids contents in the black seed.
Assessment of biochemical variables
Before beginning of phase 1, patients were referred to a laboratory test for evaluating blood parameters. Then, measurement of blood parameters were repeated in the end of phase 1, beginning and end of phase 2.
Measuring body weight
For measuring of body weight, a weighing scale with accuracy 0.1 kg was used. Measurement was done on subjects without a shoe and having less wear [23].
Measuring of BMI
Calculating of BMI was done by the equation: weight (kg) divided to the square of height (m2) [23].
Measuring of WC
Measuring of WC was done by using a non-stretchable tape ruler. The value of WC was obtained by measuring the distance around the smallest area below the rib cage and above the umbilicus [23].
Measuring of blood glucose
For analyzing this parameter, the subjects were referred to the laboratory after 10–12 hours of fasting. Samples of patients were taken from venous blood. Blood samples were centrifuged for 5–7 minutes with 3,000 g at 37°C within 20–30 minutes of collection. FBG was measured in a colorimetric manner by using commercial kits (Pars Azmoon Co., Tehran, Iran).
Measuring of BP
Patients were requested to have a rest for 10 minutes before measuring BP. BP was measured by a clinic nurse and using standard sphygmomanometer. BP was measured in the left arm of patients twice and the mean value of 2 measurements was reported as actual BP [24].
Statistical analysis
The statistical analysis was performed by SPSS (version 22; IBM Corp., Armonk, NY, USA). The statistical analysis evaluated the comparison of effect of 2 types of bread (treatment effect), the grouping of subjects (sequence effect) and before and after of intervention (time effect) on related parameters in this crossover study. The general linear model was a statistical manner for evaluating these effects. A p value of < 0·05 was considered significant.
RESULTS
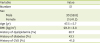
Of 54 MetS patients in this study, 3 participants dropped out (2 male and 1 female) during the study because changing of medical prescription and therapy process (< 6% drop out). Therefore 51 patients completed the study procedure (Figure 1). Biographic and clinical characteristics of patients were summarized in Table 2. Numbers of male and female patients were 30 and 21, respectively. Mean age of all subjects was 47.5 ± 5.7 years old. Mean BMI of all subjects was 29.9 ± 3.8 kg/m2. Besides, family history of diseases in patients was presented in this table.

Table 2
Biographic and clinical characteristics of participants
| Variable | Value | |
|---|---|---|
| Number | 51 | |
| Sex | ||
| Male | 30 (58.8) | |
| Female | 21 (41.2) | |
| Age (yr) | 47.5 ± 5.7 | |
| BMI (kg/m2) | 29.9 ± 3.8 | |
| History of dyslipidemia (%) | 62.7 | |
| History of diabetes (%) | 43.1 | |
| History of CVD (%) | 41.2 | |
Values are expressed as number (%) or mean ± standard deviation.
BMI, body mass index; CVD, cardiovascular disease.
![]()
Effects of treatment (2 types bread), sequence (grouping of subjects), and time (before and after of intervention) of the study were evaluated after dividing the patients into 2 groups (as crossover study). Mean and standard deviation of biochemical parameters were stated based on the types of the treatment (A or B), the grouping of patients (AB or BA) and time of parameter measurement (Pre or Post of intervention) (Table 3).
Table 3
Descriptive statistics of clinical indices in treatments, sequence and times effect of study by general linear model

Clinical indices are expressed as mean ± standard deviation. Participants in group A received a bread with N. sativa and in group B received a bread without N. sativa. AB presents the group who consumed firstly bread with N. sativa and after bread without it and BA presents the group who consumed firstly bread without N. sativa and after bread with it.
BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, fasting blood glucose; PRE, the beginning of phase; POST, the end of phase.
![]()
Based on results, treatment, sequence and time effects have influenced blood parameters in MetS patients but these effects were not significant in many of them. Furthermore, the mean of changes was different in related indices based on the type of effect. Use of bread with N. sativa has not significant treatment effect (as the most important effect) on FBG, systolic blood pressure (SBP), diastolic blood pressure (DBP), body weight, WC, and BMI (p > 0.05). Sequence effect was significant on FBG, weight, WC, and BMI (p < 0.05); but was not on BP (p > 0.05). Time effect was only significant on DBP (p < 0.05) and was not significant on other parameters (p > 0.05) (Table 4).
Table 4
Effects of treatment, sequence, and time of study on clinical indices by general linear model

BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, fasting blood glucose.
*p value of < 0.05 was considered as significant.
![]()
DISCUSSION
The purpose of this study was to evaluate the effects of bread with N. sativa on blood glucose, BP, and anthropometry indices in MetS patients in the framework of a crossover study. As it is said above, these effects were not significant on most of the clinical parameters. On the other hands, consumption of bread with N. sativa (in comparison of bread without that) does not have a significant effect on these parameters (treatment effect). Also, there was no significant effect between the mean of changes of parameters in the beginning and end of study (time effect) except to DBP. But, in regards to the grouping of patients (to be included in intervention and control group first or last), this effect of study was significant for some of parameters (FBG, weight, WC, and BMI) and was not on BP (sequence effect). In regards to evaluating of effects of N. sativa on related parameters, these results were in accordance with results from other studies but in some part, were contradict to others.
Supplementation of N. sativa could not reduce FBG significantly with a dose of 2 g daily in the study of on hyperlipidemic patients [17]. In another study on obese men also did not report any significant change in FBG with consumption of N. sativa supplementation with dose 1.5 g daily [21]. In contrast, in a study with type II diabetic patients has shown a significant change in FBG with consumption of N. sativa with dose 5 mL daily [25]. Study on patients with MetS showed also a significant change in FBG with consumption of N. sativa with dose 5 mL daily [26].
Several mechanisms are recommended for the hypoglycemic effect of N. sativa including: presence of thymoquinone with antioxidant activity [27], reducing glucose absorption from the intestine [28].
In spite of above-mentioned results and mechanisms, in this study, bread with N. sativa did not have a significant effect on blood glucose.
Of course, previous studies evaluated the effects of N. sativa in the form of pharmacological supplementation; but in this study, we used the food form of N. sativa. Thus, it is possible that food intervention has different effects in comparison to pharmacological intervention.
A few reasons could be taken into consideration for no effect of bread with N. sativa on blood glucose: 1) effect of cooking quality and characteristic of N. sativa, 2) not consumption of bread totally by patients, 3) irregular consumption of bread by patients, and 4) different characteristic of patients to other studies [29].
Positive sequence effect that has been acquired in this study on some of parameters (FBG, body weight, WC, and BMI), means that patients who was assigned intervention group in phase 1) and after transferred to control group in phase 2) showed significant change for these indices in comparison to patients who was assigned inversely. This is probably related to spent time in this study. Although, treatment and time effects of this crossover study did not show, overall, any significant change in blood glucose by bread with N. sativa.
This study has not revealed a significant change in BP. This result is similar to a study that reported N. sativa supplementation with a dose of 500 mg daily could not lower BP significantly in MetS patients [30] and similar to a result of a study that reported this supplementation with a dose of 5 mL daily did not reduce BP in patients with MetS [26]. In contrast, in a study on healthy, subjects with N. sativa supplementation with 5 mL daily reduced BP significantly [31]. Also, in a study on patients with mild hypertension 400 mg daily supplementation of N. sativa had a significant effect on BP [32].
Several mechanisms are proposed for hypotensive effect of N. sativa including: inhibition of angiotensin converting enzyme by flavonoids [33] or mediating some signaling molecules that lead to lowering BP [34].
This study was performed with MetS patients. In most studies, N. sativa supplementation did not show a significant change in this clinical parameter. It is considered that the hypotensive effect of N. sativa is mainly influenced by clinical conditions of patients at baseline of the study. Also, in this study, a type of N. sativa which was incorporated to food (bread), was different to other studies which used the pharmacological form and the effect of this seed might vary as food.
In regard to anthropometry indices (body weight, WC, and BMI), this study did not show any significant change (as treatment effect of study) by N. sativa supplementation. This result is similar to other studies which evaluated the effects of N. sativa with different doses on anthropometric indices in MetS patients [182022]. Only a study with obese men showed that N. sativa reduced these parameters [21]. It is possible that the effects of black seed on anthropometric parameters are related to a type of disease that patients bear.
CONCLUSION
Taken together, this study demonstrated significant sequence effects of bread with N. sativa on some of the clinical indices (FBG, body weight, WC, and BMI), and time effect on DBP. However, treatment effects (as the most important effect) of N. sativa on blood glucose, BP and anthropometric indices were not significant in MetS patients. This study is one of the most updated trials in related to food form of N. sativa supplementation. Based on the results of this study it is proposed that further studies can be performed with other functional food and the mechanisms of therapeutic effects of herbal foods should be investigated.
 XML Download
XML Download