

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Children constitute a significant percentage of the world's population and improving their health is a priority for all communities [1]. Malnutrition affects all groups, but affects infants and children more due to rapid linear growth, as well as the rapid growth of the brain and the immune system in them [2]. Malnutrition or failure to thrive (FTT) is a clinical syndrome in which the infant or child falls out of the main pattern of growth and is constantly under the 3% curve for height and weight or with more than 2 standard deviations below mean height and weight [34]. Nearly 100 million children under the age of five are suffering from protein-energy malnutrition (PEM) or failure to thrive (FTT) worldwide [4]. Malnutrition in childhood causes delay in body growth, short stature and disturbances in the mental development of children, and is associated with frequent infections and resistance to treatment. In addition to the physical growth retardation in children with malnutrition, the prevalence mental disorders, lack of academic achievement and reduced productivity are very common and these children cannot reach their mental and physical abilities later in life [5]. According to the United Nations International Children's Emergency Fund (UNICEF) statistics, 11% of Iranian children suffer from moderate and severe underweight, and 15% suffer from moderate and severe short stature [6]. It should be noted that not only malnutrition is an important health problem, but is also a problem of economic development, and a human issue. Growth assessment is very important in determining the nutritional status of children up to the age of puberty, and slow growth is one of the symptoms of being deprived of proper nutrition [7]. More than one-sixth of the diseases in the world are due to malnutrition, which might reach one-third in some deprived areas [8]. The causes and the factors contributing to malnutrition include insufficient food intake, parents' literacy level, low environmental health in some areas, lack of potable water, frequent and poor pregnancies, and the inadequate nutrition of children and women and poverty. Based on the results of the Anthropometric Nutritional Indicators Survey (ANIS) in 2004, the percentage of children with moderate and severe underweight, short stature, and slimness in Iran was 5.2, 4.7 and 3.7, respectively [9].
Malnutrition is one of the most important causes of death and pathogenicity in children, which is usually caused by poor or inappropriate food intake. Among the factors that lead to inadequate food intake can be diarrhea, anorexia, severe vomiting, parasitic diseases, celiac disease, harelip, cleft palate, pyloric stenosis [10] bad nutritional habits, poor mental-spiritual food intake, severe poverty or nutritional ignorance [11]. The frequency of malnutrition risk factors varies across different geographical regions and various socio-cultural conditions. That’s because the pattern of food intake, cultural beliefs and access to health care is different in various regions. Unfortunately, poverty and malnutrition together create a defective chain and cycle that reinforce each other and worsen the status of society in all dimensions. The persistence of this problem in the community is associated with problems in children, including physical and mental development disorder, decreased IQ, decreased learning power and academic failure, increased incidence of diseases and osteoporosis, and, finally, decreased mental and physical abilities of individuals, and economic development of the country. Therefore, by conducting studies in this field, we will further understand the factors affecting malnutrition, and we can reduce the incidence of malnutrition through intervention programs and take steps to promote the health of children. One of the most important objectives of meta-analyses is providing a precise and valid result, due to an increase in sample size by combining different studies and thus reducing the confidence intervals and solving problems caused by the controversial results of previous studies. Considering various studies conducted on the prevalence and causes of malnutrition in Iran and in order to validate the results of these studies, a meta-analysis seems necessary to provide a precise and credible criterion for planners and researchers in this regard. The aim of this study was to determine the prevalence and causes of malnutrition, according to Gomez classification (weight for age), Waterlow classification (weight for height) and height for age in Iran through meta-analysis.
MATERIALS AND METHODS
The present study reviews studies published on the prevalence of malnutrition and its effective factors in Iran and includes various sections such as problem statement, data collection, statistical analysis and interpretation of results.
Searching for articles
The search process was started to find Persian and English articles published until September 2017 regarding the prevalence of malnutrition in children under the age of six in Iran using national and international databases including SID, Magiran, Irandoc, IranMedex, PubMed, Medline, Scopus, and ISI Web of Science. The keywords used to search articles were: malnutrition, prevalence, causes, Iran, and all possible combinations. The English equivalents of these keywords were used in international databases. Boolean operators (and, or) were used to combine words. After reviewing the titles and summarizing the articles, their relevance for inclusion in the study was determined to be studied in their "full text". In addition, relevant studies that were included in the list of references for each selected article were also examined to be included in the study. A reference list of selected studies and unpublished national surveys were searched manually as further search tools.
Inclusion and exclusion criteria
All cross-sectional studies and review articles that had the search keywords in their title or abstract were considered, irrespective of the time of the studies and the time of their publication. The main criterion for entering various articles in this study was mentioning the prevalence of malnutrition in Iran. The final review was limited to studies that were randomly performed among the age group under 6 years of age without known disease. Studies were excluded from the analysis for any of the following reasons: lack of reference to the prevalence of malnutrition, articles conducted in other age groups other than children under six years of age, lack of access to full text of articles, non-relevance of subject matter and low quality of articles. In addition, studies that were conducted among people with known disorders, studies with inadequate data, review articles, a summary of congresses, studies published in languages other than Persian and English, systematic studies, and meta-analyses and repeated publications were excluded from the analysis. To assess the quality of the studies, the STROBE statement was used and poor quality studies were excluded from the study. If necessary, the authors were contacted for further information.
Data extraction
The following data were extracted for all studies: first author, year of publication, year of study, study location, sample size, mean and age group, gender, overall prevalence of malnutrition indices including underweight, short stature and slimness based on different criteria, the prevalence of underweight, shortness and weight decreased based on the level of indices (Z≤−1SD as mild, −1SD<Z≤−2SD as moderate and −3SD<Z as severe), the prevalence of indices based on effective factors including gender, place of residence, household economic status, parental employment status, parental education and birth interval. Reviewing the articles and extracting data was done independently by two authors, and if the results did not match, the studies were jointly examined to resolve the disagreements. In the next step, the data were entered into the data collection form and then the X application.
Statistical analysis
Considering the fact that the prevalence of malnutrition indices and sample size were extracted in each article, the binomial distribution was used to calculate the variance of each study and the weighted average was used to combine the prevalence rate of various studies. Each random variable was weighted in inverse proportion to its variance. To evaluate the heterogeneity, Q test and I2 index were used. In cases where the results of the studies were heterogeneous, the random effects model was used. In this study, due to the considerable differences in the prevalence rates in different studies (heterogeneity of studies) and the significance of I2 index, the random effects model was used in meta-analysis. The results are presented as funnel plot 1. The effect of the year of publication and sample size as a source of heterogeneity between studies was evaluated through meta-regression. The publication bias was calculated using funnel plots and Egger's test. The data were analyzed using R and Stata Software Version 11.2.
RESULTS
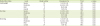
Based on the initial search in national and international databases, 117 articles that included the keywords “prevalence” and “malnutrition” were identified. In addition, as a result of searching the reference list of articles, 45 articles were identified. Overall, 162 articles were identified to be included in the study. In the initial screening stage based on the evaluation of the title and abstract, 109 articles were removed due to failure to meet the inclusion criteria, and 53 articles remained to be considered for the full text. In the next stage and after evaluating the full text of the articles, 26 articles were excluded (7 review articles, 10 low-quality articles and 9 articles with insufficient data). Finally, after a thorough review of the articles, 27 articles from 2002 to 2016 were selected to enter the meta-analysis stage [111213141516171819202122232425262728293031323334353637] (Figure 1). The general specifications and data of these articles are presented in Table 1. Considering all the studies in this meta-analysis, the total sample size was 161,941 with an age range of 0–6 years, of which 50.9% were male and 49.1% were female, 43% were urban population and 57% were rural population.

Table 1
General data of selected studies in meta-analysis of malnutrition prevalence in Iran

| References | Place | Year of publication | Sample size | Age | Prevalence of malnutrition indicators (95% CI) | Criteria | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lightweight | Low height | Slimming | |||||||||
| Level | Sex | Level | Sex | Level | Sex | ||||||
| Nojomi et al. [11] | Karaj | 2003 | 567 | < 5 | - | 15.6:G | - | 19.1:G | - | 4.3:G | Z-score |
| 12.3:B | 21.4:B | 5.6:B | |||||||||
| 13.9:T | 20.3:T | 4.9:T | |||||||||
| Eftekhari and Mozaffari [12] | Lar | 2006 | 2,258 | < 5 | - | 17.1:G | - | 15.6:G | - | 13.7:G | Gomes |
| 12:B | 11.3:B | 15.7:B | |||||||||
| 29.2:T | 26.8:T | 29.4:T | |||||||||
| Kabir and Keshtkar [13] | Golestan | 2006 | 1,473 | < 2 | 0.6:S | 3.6:G | 3.2:S | 7.2:G | 0.5:S | 3.4:G | Z-score |
| 3.5:M | 4.6:B | 7.6:M | 14.3:B | 2.7:M | 3.0:B | ||||||
| 17.3:H | 4.1:T | 20.6:H | 10.8:T | 13.3:H | 16.5:T | ||||||
| Veghari [14] | Gorgan | 2007 | 2,794 | < 5 | 0.7:S | 5.4:G | 4.4:S | 14.3:G | 0.4:S | 2.4:G | Z-score |
| 3.8:M | 3.6:B | 9.1:M | 12.6:B | 1.8:M | 2.1:B | ||||||
| 4.5:T | 13.5:T | 2.2:T | |||||||||
| Sheykh Aleslam et al. [15] | Iran | 2008 | 34,200 | < 5 | 0.6:S | 5.5:G | 1.4:S | 4.4:G | 0.3:S | 3.9:G | Z-score |
| 4.4:M | 5.0:B | 3.9:M | 5.0:B | 2.7:M | 3.5:B | ||||||
| 24.1:H | 5.2:T | 20:H | 4.7:T | 18.5:H | 3.7:T | ||||||
| Hooshyarrad et al. [16] | Iran | 2008 | 2,562 | < 5 | - | 8.0:G | - | 11.8:G | - | 4.8:G | Z-score |
| 7.3:B | 14.2:B | 4.2:B | |||||||||
| 7.6:T | 13.1:T | 4.5:T | |||||||||
| Ansary et al. [17] | Zahedan | 2009 | 1,245 | 2–6 | 1.8:S | 4.3:G | 4.4:S | 8.0:G | 2.6:S | 3.8:G | Z-score |
| 6.9:M | 2.4:B | 11.3:M | 7.3:B | 5.8:M | 4.5:B | ||||||
| 24.7:H | 3.4:T | 24.7:H | 7.6:T | 18.2:H | 4.2:T | ||||||
| Sharifzadeh et al. [18] | South Khorasan | 2010 | 1,807 | < 6 | 1.2:S | 23.7:G | 3.9:S | 21.1:G | 1.6:S | 17.5:G | Z-score |
| 11.7:M | 24.1:B | 12.7:M | 24:B | 5.9:M | 14.7:B | ||||||
| 34.9:H | 18.5:T | 28.4:H | 20.7:T | 24.7:H | 22.8:T | ||||||
| Pilevarzadeh et al. [19] | Jiroft | 2010 | 760 | 2–3 | 1.7:S | 46.2:T | 0.6:S | 37.3:T | 1.0:S | 30.7:T | Gomes |
| 10.5:M | 8.5:M | 1.3:M | |||||||||
| 35:H | 28.1:H | 28.4:H | |||||||||
| Rashidian et al. [20] | Iran | 2010 | 9,298 | < 5 | 0.8:S | 4.2:G | 1.9:S | 6.6:G | 1.4:S | - | Z-score |
| 4.0:B | 7.0:B | ||||||||||
| 4.1:T | 6.8:T | ||||||||||
| Mahyar et al. [21] | Gazvin | 2010 | 804 | < 2 | 0.2:S | 10.1:G | 1.2:S | 10.7:G | - | 7.0:T | Z-score |
| 2.4:M | 13:B | 4.2:M | 14.1:B | ||||||||
| 20.5:H | 11.7:T | 19.4:H | 11.5:T | ||||||||
| Emamiyan et al. [22] | Shahrood | 2011 | 1,359 | < 6 | 0.8:S | 5.7:T | 2.2:S | 10.3:T | 2.0:S | 4.7:T | Z-score |
| 5.7:M | 6.7:M | 4.7:M | |||||||||
| Fesharakinia and Sharifzadeh [23] | Birjand | 2011 | 480 | < 5 | 1.3:S | 5.5:G | 7.7:M | 8.4:G | 0.8:M | 1.3:G | Z-score |
| 5.0:M | 7.0:B | 11.2:B | 0.4:B | ||||||||
| 2.1:H | 6.3:T | 9.8:T | 8.0:T | ||||||||
| Nouri Saeidlou et al. [24] | Salinas | 2012 | 902 | < 5 | - | 2.9:G | - | 7.7:G | - | 1.3:G | Z-score |
| 1.8:B | 6.9:B | 1.6:B | |||||||||
| 2.3:T | 7.3:T | 1.4:T | |||||||||
| Nouri Saeidlou et al. [24] | Ravansar | 2012 | 829 | < 5 | - | 4.5:G | - | 3.8:G | - | 2.8:G | Z-score |
| 3.0:B | 3.0:B | 2.5:B | |||||||||
| 3.8:T | 3.4:T | 2.6:T | |||||||||
| Nouri Saeidlou et al. [24] | Semirom | 2012 | 794 | < 5 | - | 6.8:G | - | 10.5:G | - | 4.1:G | Z-score |
| 4.5:B | 10.9:B | 5.5:B | |||||||||
| 5.7:T | 10.7:T | 4.8:T | |||||||||
| Mohammadinia et al. [25] | Iranshahr | 2012 | 700 | < 5 | 3.4:S | 9.8:T | 2.7:S | 11.1:T | - | - | Z-score |
| 7.8:M | 7.1:M | ||||||||||
| Sheykhi et al. [26] | Zahedan | 2012 | 514 | < 5 | - | 14.9:G | - | 22.9:G | - | 3.8:G | Z-score |
| 19.8:B | 28.2:B | 9.9:B | |||||||||
| 17.3:T | 25.5:T | 6.8:T | |||||||||
| Farajzadeh et al. [27] | Birjand | 2012 | 1,132 | < 6 | 1.2:S | 23.5:G | 0.3:S | 9.7:G | 8.0:S | 36.6:G | Z-score |
| 8.7:M | 19.3:B | 3.3:M | 9.5:B | 17:M | 24.4:B | ||||||
| 32.9:H | 42.8:T | 15.6:H | 29.9:T | 36.1:H | 61:T | ||||||
| Farrokh-Eslamlou et al. [28] | West Azerbaijan | 2012 | 3,341 | < 5 | - | 3.2:G | - | 7.3:G | - | 4.6:G | Z-score |
| 4.1:B | 10:B | 6.7:B | |||||||||
| 4.3:T | 8.7:T | 7.5:T | |||||||||
| Ramezanpour et al. [29] | Maneh Semelghan | 2013 | 596 | < 5 | - | 10.5:T | - | 9.3:T | - | 10.8:T | Goms |
| Naderi Beni et al. [30] | Shadegan | 2013 | 403 | < 5 | 1.5:S | 13.8:G | 4.0:S | 15.7:G | 0.2:S | 8.2:G | Z-score |
| 5.0:M | 20.8:B | 8.7:M | 21.8:B | 2.5:M | 9.7:B | ||||||
| 28:H | 34.5:T | 24.3:H | 37:T | 15.1:H | 17.8:T | ||||||
| Gholami et al. [31] | Nishapur | 2013 | 1,621 | 3–6 | 0.7:S | 15.2:G | - | - | - | - | Z-score |
| 7.3:M | 20.3:B | ||||||||||
| 27.4:H | 35.5:T | ||||||||||
| Payandeh et al. [32] | Khorasan | 2013 | 70,339 | < 5 | 0.7:S | 7.6:G | 3.2:S | 15.4:G | 0.5:S | 5.8:G | Z-score |
| 6.8:M | 7.5:B | 9.3:M | 9.7:B | 4.0:M | 3.1:B | ||||||
| 7.5:T | 12.5:T | 4.4:T | |||||||||
| Zabihi et al. [33] | Babol | 2013 | 782 | < 2 | 0.5:S | 5.4:G | 1.4:S | 4.6:G | 1.8:S | 10.4:G | Z-score |
| 2.3:M | 5.0:B | 1.3:M | 1.0:B | 5.1:M | 3.9:B | ||||||
| 11.9:H | 3.0:T | 5.6:H | 2.8:T | 14.2:H | 7.1:T | ||||||
| Shafieian et al. [34] | Mashhad | 2013 | 617 | 2–5 | 4.3:S | 28.7:T | 3.1:S | 16.1:T | 4.3:S | 27.9:T | Z-score |
| 24.4:M | 13:M | 23.6:M | |||||||||
| Kavosi et al. [35] | Fars | 2014 | 15,408 | < 5 | - | 9.6:T | - | 9.5:T | - | 8.2:T | Z-score |
| Veghari [36] | Gorgan | 2015 | 2,487 | < 5 | 2.3:S | 6.2:G | 7.4:S | 15.3:G | 0.6:S | 2.5:G | Z-score |
| 4.3:M | 7.1:B | 8.3:M | 16:B | 2.1:M | 2.9:B | ||||||
| 6.6:T | 13.7:T | 2.7:T | |||||||||
| Ahmadipour and Mirzaesmaeili [37] | Kerman | 2016 | 360 | 2–5 | - | 9.9:G | - | 5.9:G | - | 16.8:G | Z-score |
| 8.2:B | 7.0:B | 13.3:B | |||||||||
| 9.0:T | 6.4:T | 15:T | |||||||||
![]()
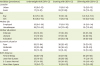
Table 2 shows the final estimate of the prevalence of malnutrition through meta-analysis of the data extracted from studies conducted in Iran.
Table 2
Malnutrition prevalence in terms of the number of studies included in the meta-analysis
![]()
In the studies, the prevalence of moderate and severe stunting and Weight Loss determined according to the percentage of children whose weight or height was 2 standard deviations less than the weight or height of the children of the reference population with similar characteristics of age and sex. . Also, the prevalence of moderate and severe weight loss was determined according to the percentage of children with a weight of 2 SD less than the weight of reference children with similar characteristics in terms of height and sex. Accordingly, malnutrition, stunting, weight loss and weight loss indices in three mild forms (between one to two standard deviations from the mean), moderate (between two to three standard deviations from the mean) and severe (below the three Standard deviation from the mean) was calculated and presented.
Overall, 27 studies were evacuated to calculate the prevalence of underweight; 19 studies reported severe prevalence, 18 studies reported moderate prevalence and 11 studies reported mild prevalence. The final estimate of the underweight prevalence based on the level of the indices was as follows: severe underweight (1%; 95% confidence interval [CI], 1–1) (Figure 2), moderate underweight (6%; 95% CI, 5–7), mild underweight (25%; 95% CI, 21–28). The final estimate of the underweight prevalence, regardless of the level of indices, was 13% (95% CI, 12–15) (Table 2).
 | Figure 2Prevalence severe underweight based on the random effects model. The midpoint of each section of the line estimates the prevalence and the length of the segment, the 95% CI in each study, and the diarrhea sign, indicates the prevalence the country for the all study.ES, effect size; CI, confidence interval.
|
Of the articles included in this study, 18 studies reported severe short stature prevalence (Figure 3), 17 studies reported moderate short stature prevalence and 10 studies reported mild short stature prevalence. Thus, the final estimate of the meta-analysis for severe, moderate, and mild short stature prevalence was (3%; 95% CI, 2–3), (8%; 95% CI, 6–9), and (21%; 95% CI, 17–24). The final estimate of the short stature prevalence, regardless of the level of indices, was 14% (95% CI, 13–16) (Table 2).
 | Figure 3Prevalence severe stunting based on the random effects model. The midpoint of each section of the line estimates the prevalence and the length of the segment, the 95% CI in each study, and the diarrhea sign, indicates the prevalence the country for the all study.ES, effect size; CI, confidence interval.
|
As shown in Table 2, 15 studies reported severe slimness prevalence (1%; 95% CI, 1–1) (Figure 4), 15 studies reported moderate slimness prevalence (5%; 95% CI, 4–5) and 9 studies reported mild slimness prevalence (20%; 95% CI, 17–24). In addition, the final estimate of the prevalence of slimness, regardless of the level of indices, was 11% (95% CI, 9–12).
 | Figure 4Prevalence severe wasting based on the random effects model. The midpoint of each section of the line estimates the prevalence and the length of the segment, the 95% CI in each study, and the diarrhea sign, indicates the prevalence the country for the all study.ES, effect size; CI, confidence interval.
|
In the present study, the prevalence of malnutrition indices was calculated based on gender. As shown in Table 3, the prevalence of underweight was similar in boys and girls (9% vs. 9%). Moreover, the short stature prevalence between the boys and girls were 12% and 11%, respectively. Similar results were observed for slimness (7% for girls and 6% for boys).
Table 3
Factors related to malnutrition in Iran
![]()
The other results of the present study were in regard with the factors affecting malnutrition in Iran. Table 3 shows the results of meta-analysis of the data extracted in this regard. The results of the effect of the place of residence on the prevalence of malnutrition indices were as follows: The prevalence of underweight in the villages was significantly higher than the reported prevalence in the cities (17% versus 10%). Similar results were reported regarding the prevalence of short stature; the prevalence in the village was significantly higher than the city (23% versus 11%). However, there was no significant difference between the prevalence of slimness in the city and the village (12% in the city versus 10% in the village).
The results of this study showed that maternal occupational status was one of the factors influencing the prevalence of malnutrition indices in Iran. As shown in Table 3, the prevalence of all three indices of short stature, underweight and slimness was lower among children whose mothers were employed compared to the children whose mothers were housewives.
In addition, the results of meta-analysis showed that the level of maternal education had an impact on malnutrition indices; the prevalence of short stature, underweight and slimness among children with literate mothers was higher than that of children with illiterate and low-educated mothers (Table 3).
As shown in Table 3, other factors affecting the prevalence of malnutrition indices in Iran are household economic conditions. The results of meta-analysis showed that there is a direct relationship between the economic condition of the family and the prevalence of malnutrition among children. The prevalence of malnutrition indices in children whose families have a good economic situation are lower than those whose families have modest and poor economic status.
According to our study, another factor that affects the prevalence of malnutrition indices in Iran in the birth interval; there is a direct relationship between birth interval and the prevalence of malnutrition indices (Table 3).
Then, the relationship between the prevalence of malnutrition and the year of the study and the number of samples was assessed using the meta-regression model.
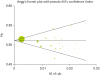
In Figure 5, the relationship between the sample size and the prevalence rate has been assessed. According to the meta-analysis, this figure shows that there is no significant relationship between sample size and prevalence rate (p = 0.006), because it is possible that studies with a larger sample size report higher prevalence rate and vice versa. In the presented figure, the circles represent the weight of the studies, and the larger the circle, the larger the sample size.
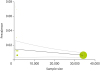
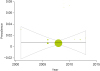
Figure 6 shows the relationship between the prevalence of malnutrition and the year of studies in Iran. As shown in this figure, there is no statistically significant relationship between the prevalence of malnutrition in Iran and the year of studies (p = 0.927). In addition, Figure 7 shows the publication bias using the Begg's funnel plot. The meta-regression analysis did not show significant asymmetry and therefore there was no indication of publication bias (Figure 7). As the regression line slope was negative (p = 0.29), there was no significant relationship between the prevalence of malnutrition and the year of studies in Iran.
DISCUSSION
Children are significantly at risk of malnutrition due to their nutritional needs for growth. Therefore, ensuring their health, growth and development are important priorities in all societies [37]. Since meta-analyses provide an accurate and valid result due to the large sample size obtained from the combination of studies, the present study was conducted to determine the prevalence of malnutrition in Iran. This systematic review article, including 161,941 children under the age of six from 27 published studies, was conducted to assess the overall malnutrition prevalence in this age group and to have a comprehensive review of these studies.
The results of this study showed that the overall prevalence of malnutrition indices in Iran based on the level of indices was as follows: severe, moderate and mild underweight were 6%, 1% and 25%, respectively. Severe, moderate and mild, short stature was 3%, 21%, 8%, respectively. Severe, moderate and mild slimness were 5%, 1%, and 20%, respectively. The final estimate of the prevalence of malnutrition indices, regardless of the level of indices, was as follows: underweight; 13%, short stature; 14%, and slimness; 11%. According to UNICEF, the prevalence of underweight, short stature and underweight in Iranian children under the age of five was 11%, 15%, and 5%, respectively [37]. The present study is consistent with these statistics in terms of underweight and short stature, but shows higher results regarding slimness.
The studies in Haiti, Latin America, regarding underweight, short stature and slimness reported a prevalence of 16.1%, 14.8%, and 15.3%, respectively [38]. These statistics are close to our study results. In this study, the prevalence of mild, moderate and severe underweight was 34.2%, 11.8% and 4.3%, respectively. The prevalence of mild, moderate and severe short stature was 10.4%, 31.3% and 4.4%, respectively. The prevalence of mild, moderate and severe slimness was 11.5%, 25.8%, and 3.8% respectively [38]. In Ecuador (in other Latin American countries), the prevalence of short stature was more than our study (35.9%), whereas the prevalence of underweight (7.4%) and slimness (1.1%) was lower [39]. The majority of studies in Africa reported a high prevalence of malnutrition indices. For example, a meta-analytical study in 32 countries from the north, south, west and sub-Saharan Africa showed that children under the age of five were 25% to 36.4% underweight, 36.6% to 57.7% short, and 6.2% to 18% slim [40]. The prevalence of underweight in Nigeria was 17.1%, 24.8% and 20%, respectively [41]. A meta-analysis in Ethiopia showed that children under the age of five had 33% underweight, 40% short stature, and 19% slimness [42]. Similar results were reported in studies conducted in Kenya, Tanzania and Ghana [434445]. Comparing the results of this study with the studies mentioned in these areas shows that the prevalence of malnutrition in Iranian children below the age of five is lower than that of African children.
The prevalence of malnutrition in Asia was different in various studies. In children under the age of five in Nepal, the prevalence of underweight, short stature and slimness was reported to be 18.6%, 39.9%, and 7%, respectively [46]. In the Philippines, the prevalence of malnutrition indices in this age group was as follows: moderate and severe underweight (18%), moderate and severe short stature (26%) and moderate and severe slimness (26%) [47]. A study in Bangladesh also reported 33% underweight, 39% short stature, and 14% slimness [48]. The prevalence of underweight, short stature and slimness among Indian children was reported to be 55.4%, 60% and 43%, respectively [49]. These data show that the prevalence of malnutrition in children from these regions of Asia is higher than that of Iranian children. A meta-analysis, including 17 studies in Palestine, showed that the prevalence of underweight, short stature and slimness in children under the age of five was 4.7%, 10.9%, and 2.9%, respectively [50]. This study reported a lower prevalence of malnutrition indices compared to our study. Studies in Arabian countries have reported a varied prevalence from 2% in Jordanian children (for underweight and slimness) to 28% in Syria and 29% in Egypt (for short stature) [51]. According to the WHO classification, less than 20% prevalence of malnutrition indices indicates low prevalence, 20%–29% indicates moderate prevalence, 30%–39% indicates high prevalence and over 40% prevalence indicates the very high prevalence [52]. According to these statistics and the results of this study, it can be concluded that the prevalence of malnutrition in Iranian children is low in terms of underweight, short stature and slimness.
The prevalence of malnutrition indices in children is decreasing worldwide. Each year, UNICEF's flagship publication, The State of the World's Children, closely examines a key issue affecting children. This report shows a reduction in the mortality of children under the age of five due to the reduction of the global prevalence of malnutrition over the past 20 years [53]. A study in Bangladesh showed that over the course of two decades, from 1993 to 2012, short stature rate decreased from 53% to 21%, slimness rate decreased from 32% to 22%, and underweight rate decreased from 59% to 29% [54]. In the Peruvian studies, underweight decreased from 10.1% to 8.2% over the course of 15 years and short stature rate decreased by 19.6% [55]. A meta-analysis conducted in Palestine showed that the prevalence of malnutrition indices decreased significantly from 1998 to 2007 [50]. Studies in China have also shown a decline in indices in children under the age of five since the 1990s [56]. There has also been a significant decline in indices in India from 1992 to 2005 [57]. In Ethiopia, a meta-analysis of the studies published from 2001 to 2015 showed that the prevalence of malnutrition indices decreased significantly during these years [42]. A review of studies included in the present meta-analysis based on the year of the study shows that malnutrition in Iranian children under the age of five years has significantly decreased in recent decades. In the past decades, there has been no meta-analysis in Iran in this regard to examine the trend of malnutrition changes. Therefore, the results of several studies in Iran with large sample size were considered. The study of these studies also confirms the current meta-analysis. The prevalence of moderate and severe underweight decreased from 16.6% in the first national survey of the status of children's anthropometric indices in 1995 to 10.9% in the second national survey in 1998, called Anthropometric Nutritional Indicators Survey (ANISE)1, and 5.2% in the ANISE2 survey in 2004. The moderate and severe short stature prevalence also decreased from 19.7% in 1995 to 15.4% in 1998 and 4.7% in 2004. The prevalence of moderate and severe slimness also decreased from 7.1% in 1995 to 4.9% in 1998 and 3.7% in 2004 [585960].
The results of this study showed that the prevalence of malnutrition indices in girls and boys was the same and there was no significant difference in the prevalence of indices based on gender. In national studies conducted in 1995, ANISE1 and ANISE2 also reported similar results [585960]. In the studies conducted in other parts of the world, the differences between these indices between girls and boys are not statistically significant and are consistent with the present study [40414243444546]. UNICEF reports show that the prevalence of underweight between boys and girls is similar in developing countries [61].
Other results of the present study were the high rate of slimness, underweight and short stature in rural areas compared to urban areas. Similar results have been reported in other studies in the other parts of the world [626364]. In the survey of 1995, the prevalence of underweight, short stature and slimness in urban and rural areas was 13.3% vs.17.7%, 12.2% vs. 24.8%, and 7.8% vs. 6%, respectively [58]. In the ANISE1 survey, the prevalence of these indices in urban and rural children was 9.6% vs. 13.7%, 11% vs. 21.8% and 4.8% vs. 5.6%, respectively [59]. In the ANISE2 survey, the prevalence of underweight, short stature and slimness in urban and rural areas was 4.7% vs. 6%, 3.3% vs. 6.8% and 4.1% vs. 3.3%, respectively [60]. These results are consistent with the results of our study, which seems to be due to the lack of adequate nutrition and lack of minerals, vitamins and protein in the rural areas. Lower socioeconomic status and the general conditions of life in rural areas affect the choice of food and nutrition. It is claimed that urban children have a better nutrition than rural children [63]. Furthermore, differences in the level of education in urban and rural areas and the lack of access to appropriate sanitation systems in rural areas also justify somewhat unequal distribution of malnutrition among urban and rural children [44]. A study on the relationship between place of residence and family income also shows that there is a significant relationship between place of residence and wealth, which affects the prevalence of malnutrition [65].
Identifying the factors affecting malnutrition in children can be helpful in identifying appropriate preventive measures. The results of this study showed that the mother's education level and occupational status, household economic conditions and birth interval are the factors influencing the prevalence of malnutrition indices. The review articles and systematic reviews conducted in South Asia and the sub-Saharan Africa have also reported that factors such as low income, food shortage, illiteracy of parents and food insecurity are the factors associated with malnutrition [6667]. Another review article on the determinants of malnutrition in low and middle income countries (LMICs) reported the biological causes such as the infections and social causes such as wealth, education and urbanization as risk factors for malnutrition in children though INDEPTH health and demographic surveillance systems [68]. Poverty is one of the most important risk factors in the prevalence of malnutrition, which has been reported in numerous studies in different countries [676869]. Low-income families are believed to be less aware of their children's nutritional needs, and children living in these families have less access to the food they need to grow properly and are more likely to be affected by inappropriate nutrition and health problems than other children [707172]. Mothers' education can also play an important role in a child’s nutrition and hygiene, and mothers' lack of knowledge about complementary nutrition is another risk factor for malnutrition [73]. Mothers' higher education helps to make more use of healthcare, agreement with modern medical practices, and increase women's autonomy, which in turn affects health decisions and improves the child's nutritional outcomes [747576]. The present study showed that the prevalence of underweight and growth failure at different stages of the interval between the two last pregnancies was significantly different. It has been confirmed that birth interval and mother's education are clearly related with the mortality of children [77]. Socioeconomic factors such as the education of parents, especially the mother, family income, and biological and behavioral variables such as the birth interval, birth weight and maternal health status can indirectly influence the nutritional status of children through affecting the quality of food and health care [7879]. For example, a study of 19 developing countries showed that a short interval between two last pregnancies is a significant risk factor for the growth failure rate among children of these countries [80].
In addition to the mentioned issues and factors, like many developing countries, educational tools have been scarcely used in Iran for solving public health problems and nutritional issues. Undoubtedly, if mothers are well taught about the nutrition concepts, especially children's nutrition, a significant part of the prevalence of malnutrition among children will be reduced.
The present study has the following limitations: First, in various studies included in this meta-analysis, the prevalence of malnutrition was different and the differences were due to different methods of sampling and also the differences in the measured parameter (the prevalence of malnutrition). Second, the low quality of a number of studies was another limitation of this study. Third, in addition, the lack of access to the full text, and in some cases even the abstracts of articles related to this subject were other limitations of this study. Finally, the publication bias is an inevitable problem in the meta-analysis of the published studies.
CONCLUSION
The nutritional status of children under five is an important index that reflects the health status of the community. The results of this study showed that the prevalence of malnutrition in Iranian children has decreased during the last decade. However, considering the importance of nutritional needs for growth in this age group, the prevalence of malnutrition is still relatively high in Iran. Therefore, health authorities should plan to improve the nutritional status of children, pay attention to developing educational intervention strategies to sensitize parents and reinforce the motivation of health workers to continually pursue the children's development and growth.
 XML Download
XML Download