

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Endovascular embolization using liquid embolic agents such as N-butyl cyanoacrylate (NBCA; Histoacryl, B Braun, Tuttlingen, Germany) or Onyx (Medtronic, Irvine, CA, USA) is a widely accepted treatment option for spinal and cranial vascular diseases (123). The penetration or delivery of a sufficient amount of liquid embolic agent into the target shunt or nidus is key to successful embolization in abnormal neurovascular shunt diseases (1234). For this purpose, a microcatheter wedge technique for NBCA delivery and proximal plug formation or dual-lumen balloon catheter for Onyx delivery have been used (567). In the majority of cases, these techniques allow controlled delivery of a sufficient amount of the embolic agent into the target shunt or nidus and prevent unintentional reflux or premature occlusion of the major draining veins (5789). However, small and tortuous feeding arteries may preclude navigation of a microcatheter close enough to the target lesion or wedging of the microcatheter tip, which are essential for safe and effective embolization with a liquid agent. The coil-protected technique may be useful in cases of cranial and spinal vascular diseases where navigation or wedging of a microcatheter close to the target lesions is difficult.
Therefore, this study aimed to evaluate the safety and effectiveness of the coil-protected liquid embolization technique for the treatment of various neurovascular shunt diseases.
Go to : 
MATERIALS AND METHODS
Data for patients who underwent coil-protected liquid embolization for cranial and spinal shunts or malformations were retrieved from a prospectively maintained neurointerventional database of a tertiary referral academic hospital. The coil-protected technique was applied as a rescue method in all cases wherein a microcatheter could not to be navigated distal enough to wedge the target feeding artery because of severe tortuosity of the target feeding artery. For these cases, the coil-protected technique was expected to promote penetration or delivery of a sufficient amount of liquid embolic agent into the target shunt or nidus by blocking unintentional reflux during injection of liquid embolic agent and retrieval of the microcatheter used for embolization. The procedural technique is illustrated in Figure 1.
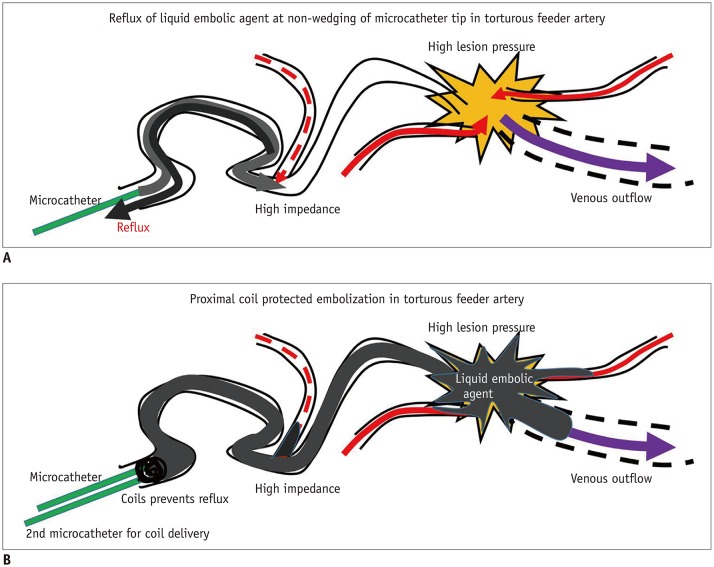 | Fig. 1Illustration of coil-protected technique.
A. During liquid embolization with non-wedging microcatheter tip due to arterial tortuosity, penetration of liquid embolic agent is impossible and early reflux occurs. B. Coil-protected technique makes it possible to deliver liquid embolic agent to target shunt without reflux proximal to coil mass.
|
Patient demographic data, lesion characteristics, and procedural and clinical outcomes of the coil-protected technique were retrospectively analyzed by reviewing the electronic medical records, procedural digital subtraction angiography data, and the prospectively maintained neurointerventional database, in which procedural details and complications had been recorded. Clinical outcomes were evaluated on the basis of clinical and radiologic examinations at the most recent outpatient visit or readmission. If the most recent outpatient visit or readmission was more than three months before the time of data collection, patients' outcomes were determined by telephone interviews performed by a trained clinical research nurse. The Institutional Review Board approved this study and waived the requirement for informed patient consent because of the retrospective study design.
Of the 153 patients who underwent endovascular treatment for neurovascular arteriovenous fistula (AVF) or arteriovenous malformation (AVM) between December 2014 and December 2018, 22 (14.3%) were treated with the coil-protected liquid embolization technique. Baseline patient characteristics are summarized in Table 1. The patient population consisted of 12 men and 10 women (mean age, median 52 years; range, 3–70 years). The patients had eight spinal AVFs, seven cerebral AVFs, six cerebral AVMs, and one mandibular AVM. One patient who was suspected to have Maffuci's syndrome had multiple cranial AVFs (Fig. 2) and hemangiomas in the liver. The coil-protected technique was applied to facilitate delivery of a sufficient amount of the liquid embolic agent into the target shunt or target point (suspected rupture point or intranidal aneurysm) of the AVM nidus or was used to prevent unintentional reflux of the embolic agent to a functional arterial branching point of the feeding artery.
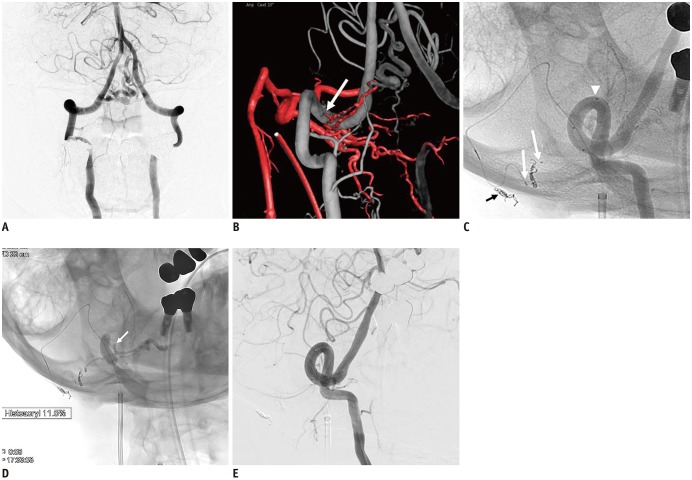 | Fig. 2Findings for 69-year-old man presenting with nausea and vomiting that had aggravated over 3 months.
A. Right vertebral angiogram shows dural arteriovenous fistula with engorged perimedullary draining vein at craniocervical junction. B. Fusion image obtained with dual 3-dimensional volume reconstruction shows relationship of two feeders, one from right vertebral artery (white color) and other from occipital artery (red color). Note that two feeders are connected near right vertebral artery (arrow). C. Non-subtracted angiogram obtained just before embolization. Arrows indicate tips of two microcatheters in feeding branch of right occipital artery, proximal microcatheter for coiling and distal microcatheter for injection of NBCA. Note coils placed between two catheter tips. Arrowhead indicates proximal marker of balloon catheter for protection of NBCA reflux into right vertebral artery during embolization. Short arrow indicates coil mass occluding another branch of right occipital artery, which is occluded to facilitate navigation of microcatheter into target feeding artery. D. Spot image obtained after injection of 11.5% NBCA. Arrow indicates reflux of NBCA into feeder arising from right vertebral artery, which is protected by inflated balloon. Use of inflated balloon during injection of NBCA prevents NBCA from refluxing into vertebral artery through its feeder, which joins with feeder of right occipital artery. E. Right vertebral angiogram shows complete occlusion of fistula. NBCA = N-butyl cyanoacrylate
|
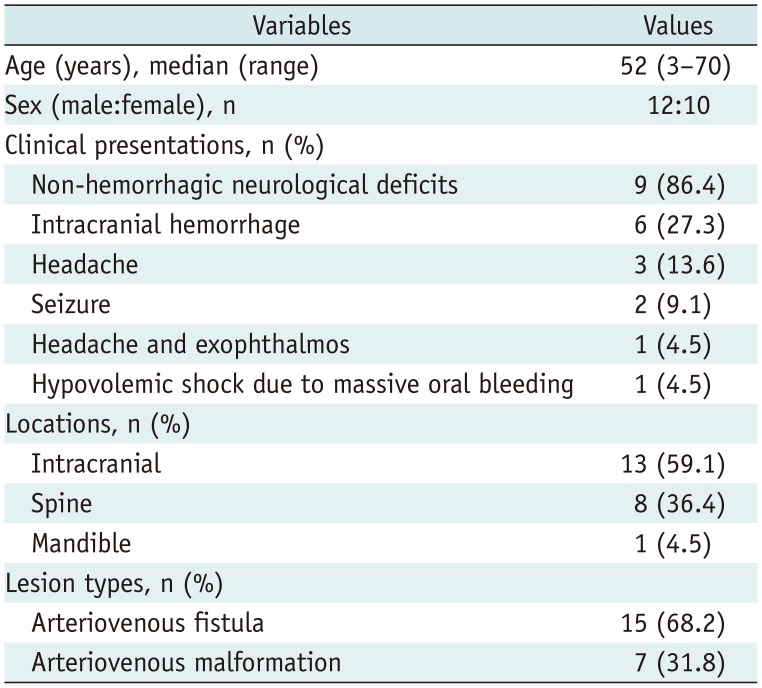
Table 1
Baseline Clinical and Angiographic Characteristics
![]()
Endovascular Procedure
All planned Onyx embolizations for AVM cases were performed under general anesthesia, while planned NBCA embolizations for AVF were performed under either general or local anesthesia at the operator's discretion. A 6-Fr shuttle sheath or 6-Fr Envoy guiding catheter (Cerenovus, Fremont, CA, USA) was placed in the relevant parent artery. If needed, a double-guide catheter system (6-Fr Envoy or 5-Fr Sofia catheter [Microvention, Tustin, CL, USA] within a 6-Fr shuttle sheath [Cook, Bloomington, CL, USA]) was used. In addition, bi-femoral access was preferred in cases where multiple feeders arose from different parent arteries. Generally, the coil-protected technique was not used unless a microcatheter wedge or dual-lumen balloon catheter advancement to a target arterial point failed. When using the coil-protected technique, the first microcatheter (Marathon, Covidien, Plymouth, MN, USA) was navigated as far as possible to the most distal point of the feeding artery, after which the second microcatheter (Prowler-10, Codman, Fremont, CA, USA or Excelsior-10, Stryker, Fremont, CA, USA) was navigated just proximal to the first microcatheter by using a compatible microwire. Using the second microcatheter, the feeding artery was occluded by placement of detachable coils at a point proximal to the first microcatheter tip (Fig. 2). Blockage of arterial inflow was confirmed through a guide catheter angiogram. The absence of reflux proximal to the feeding artery segment where the coil mass was placed was also confirmed with an angiogram through the first microcatheter (Fig. 3). The final coil was left in place without being detached to ensure the stability of the coil mass at the point of rapid retrieval of the microcatheter used for liquid embolization. Embolization was performed using a low-concentration NBCA-lipiodol mixture (NBCA, 10–20%), Onyx-18, or both depending on the geography of the feeders and the target lesions (Fig. 4). After embolization, the first microcatheter was retrieved. Finally, the final coil was detached and the second microcatheter was retrieved. The procedure was considered technically successful if the target lesion was sufficiently filled with liquid embolic agent without unintentional reflux. Angiographic results were evaluated independently by an interventional neuroradiologist who did not treat the patients and classified into complete, near-complete, and partial occlusion. Complete occlusion was defined as no visualization of the shunted cortical vein or AVM nidus in the delayed venous phase on the completion angiogram. Near-complete occlusion was defined as delayed visualization of the shunted vein or AVM nidus in the venous phase, with marked stasis of contrast agent (longer than 2 seconds). Partial occlusion was defined as visualization of the shunted vein or AVM nidus in the arterial phase on the completion angiogram, with contrast material stasis shorter than 2 seconds (7).
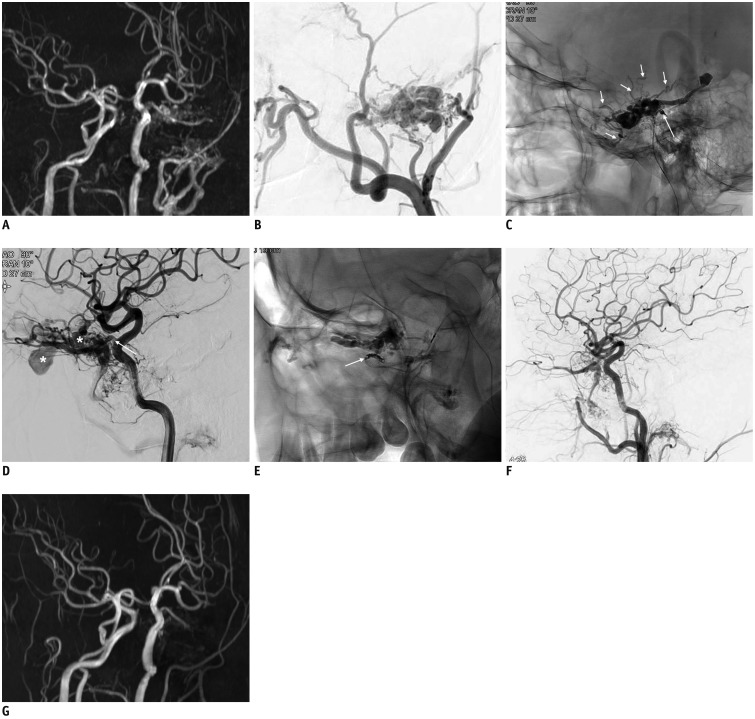 | Fig. 3Findings for 30-year-old man presenting with exophthalmos and tinnitus.
A. MR angiogram shows multiple fistulas in left orbital and left temporal regions. B. Left external angiogram in working projection shows intraosseous fistula fed by multiple feeders in left temporal bone. C. Non-subtracted spot image obtained just after injection of 12% NBCA by proximal coil-protected technique. Note refluxes to other feeders (short arrows) from fistula, which mimics phenomenon during Onyx (Medtronic) embolization. Long arrow indicates coil mass and final coil is not detached. D. Left internal carotid angiogram in working projection. Enlarged left ophthalmic artery is main feeding artery into shunt, which forms multiple venous pouches (asterisks) and then drains through superior ophthalmic vein and pterygoid plexus. E. Spot image obtained just after proximal coil-protected NBCA embolization. Coil delivery catheter is located at lacrimal branch of left ophthalmic artery (arrow). Final coil is not yet detached. F. Left common carotid angiogram shows complete occlusion of left temporal bone fistula and near-complete occlusion of left orbit fistula. G. 12-month follow-up MR angiogram shows no recurrence of fistulas in left orbit and left temporal bone. MR = magnetic resonance
|
 | Fig. 4Findings for 8-year-old boy presenting with intracerebral hemorrhage from de novo arteriovenous malformation.
A. Frontal angiogram shows arteriovenous malformation with intranidal aneurysm (arrow), which is rupture point. B. Non-subtracted image of angiogram obtained just after embolization. Note segment of feeding artery where coil mass is placed (arrowheads). Straight and curved arrows indicate microcatheter for coiling and microcatheter for Onyx injection, respectively. C. 26-month follow-up delayed arterial phase angiogram shows complete occlusion of arteriovenous malformation.
|
Statistical Analysis
Since this study only included the results of the coilprotected technique for liquid embolization without any comparisons with other techniques, only descriptive statistics are presented. All data are presented as the mean and range for continuous variables and as a number and percentage for categorical variables.
Go to :
RESULTS
Detailed information regarding liquid embolic agents and treatment outcomes are presented in Table 2. A total of 36 feeding arteries in 22 patients were embolized using the coil-protected technique. Sixteen patients were treated with NBCA alone, three with Onyx alone, and three with both. Of the 36 feeding arteries, 28 (77.8%) were embolized with NBCA, and 8 (22.2%) were embolized with Onyx. Delivery of the liquid embolic agents into a target shunt of a dural AVF (dAVF) or a weak point of an AVM nidus was successful in all 36 feeders without any unintentional reflux. Immediately post-embolization, angiographies demonstrated complete occlusion in 16 patients (72.7%), near-complete occlusion in three patients (13.6%), and partial occlusion in three patients (13.6%). The three partial occlusions were all in patients with AVM. There were no treatment-related complications. Of the six patients with near-complete or partial occlusion, five received additional treatments. Two patients received stereotactic radiosurgery for cerebral AVM, two underwent surgical removal of cerebral AVM, and one underwent additional liquid embolization for a mandibular AVM by direct puncture through the mental foramen. One patient who had Maffuci's syndrome and near-complete occlusion did not receive additional treatment because the patient's presenting symptoms (headache and exophthalmos) completely resolved and follow-up magnetic resonance angiography showed an improvement in vascular occlusion. Finally, all patients showed complete (n = 19) or near-complete occlusion (n = 3) of the target AVF or AVM nidus on follow-up angiographies. Clinically, presenting neurological symptoms improved completely in 15 patients (68.2%) and partially in seven patients (31.8%).
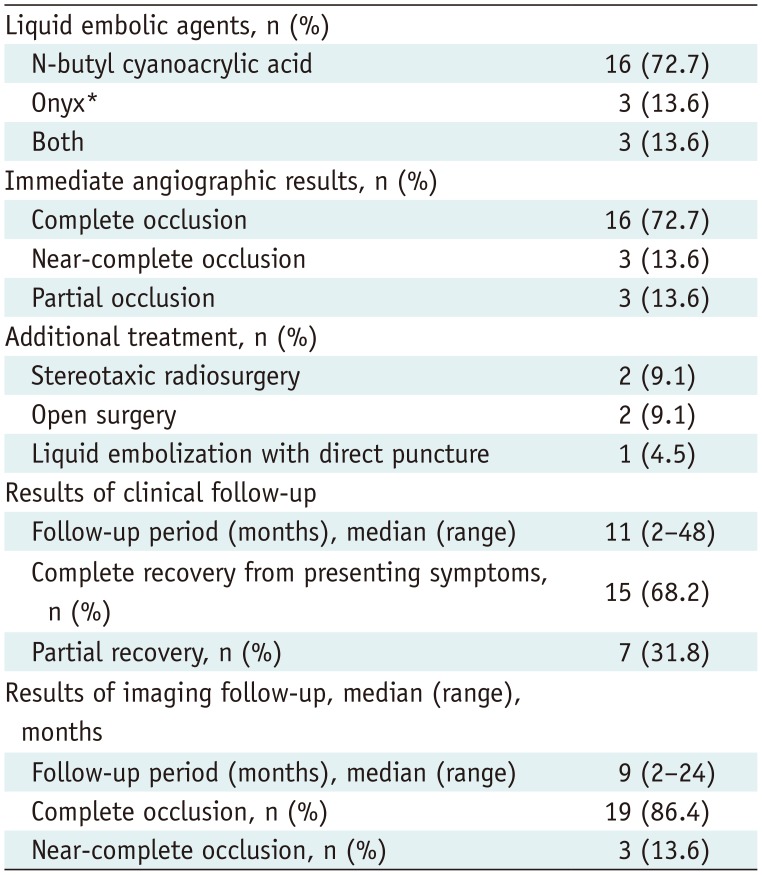
Table 2
Liquid Embolic Agents and Immediate and Follow-Up Outcomes
![]()
Go to :
DISCUSSION
Using the coil-protected technique, a sufficient amount of liquid embolic agent could be successfully delivered into the lesion of a dAVF or the weak point (suspected rupture point or intra-nidal aneurysm) of an AVM in all attempted cases. There was no treatment-related morbidity or mortality. Therefore, we believe that this technique can provide satisfactory immediate and follow-up angiographic and clinical outcomes.
Endovascular embolization is a front-line treatment for neurovascular shunts or malformations. It can be conducted via transvenous, transarterial, or both routes. Transvenous embolization is the treatment of choice and is effective for cavernous sinus dAVFs (10). However, transvenous embolization may show limited effectiveness in treating AVFs at other locations and cannot be used for AVMs, necessitating transarterial embolization. There are potentially serious risks related to liquid embolization for the treatment of neurovascular shunt diseases. Insufficient penetration of the liquid embolic agent into the target shunt leads to incomplete embolization and results in the blockage of an access route to the target site (12). Unintentional reflux may occlude functional arterial branches that supply normal nervous tissues. Furthermore, premature occlusion of the main draining veins could potentially cause a disturbance in venous drainage. This problem is particularly prominent in AVMs with a high flow shunt and can result in serious complications such as hemorrhage or venous infarct (1112).
The microcatheter wedge technique has been used for controlled delivery of a sufficient amount of embolic agent to the target lesion while avoiding serious complications (56). However, in a substantial proportion of cases, it is quite challenging to wedge a microcatheter because of the tortuosity of the feeding artery. Additionally, this carries a risk of arterial dissection or vasospasm, which would result in a loss of the access route. When Onyx is used as an embolic agent, the proximal Onyx plug formation technique with a detachable microcatheter, also known as the “plug and push technique,” is implemented. Although it can be effective in most cases, the “plug and push technique” is difficult to perform in cases with small and tortuous or highly resistant feeder vessels, such as in transosseous arteries. Another alternative technique using a dual-lumen balloon catheter for Onyx embolization has recently been reported (7). However, in small or very tortuous arteries, this method still causes difficulties in navigating the dual-lumen balloon catheter to the target arterial point and carries the risk of arterial injuries such as dissection or rupture. Furthermore, this dual-lumen balloon catheter cannot be employed with NBCA embolization because the NBCA-lipiodol mixture causes the balloon to rupture shortly after contact.
In this study, we demonstrated that the coil-protected technique can be used for safe and effective embolization to treat various spinal and cranial neurovascular shunt diseases in which the feeding arteries may be too tortuous to wedge a microcatheter tip. A similar technique had previously been reported in two small cases series for NBCA embolization of spinal dAVFs (1314). Previous investigators termed the technique “two microcatheter or induced wedge technique.” In the present study, we extended the application of this technique to cranial dAVFs and cranial AVMs in addition to spinal dAVFs. Our results demonstrated that placement of the coils just proximal to the microcatheter tip used for embolization allows artificial wedging of the microcatheter for NBCA embolization. This approach also functioned as a firm plug for forward advancement of Onyx (Fig. 3). Consequently, the coil-protection technique resulted in the delivery of a sufficient amount of the liquid embolic agent into the target shunt of dAVFs or the weak point of AVM niduses while avoiding unintentional reflux. In addition, proximal occlusion of the feeder vessel with coils blocked arterial inflow beyond the coils, which made it possible to control the delivery of the embolic agent. Subsequently, this technique was useful to prevent premature occlusion of the main draining vein. Although the coil-protected technique was technically successful in all our cases, immediate post-treatment angiography showed partial occlusion in three AVM cases. For embolization of the AVM, even when the liquid embolic agent reaches the target (such as an intranidal aneurysm) of the nidus, complete occlusion may not be achieved, especially when the AVM has multiple feeding arteries and draining veins. It is well known that the complete occlusion rate after embolization of AVMs is relatively low with the current technique and embolic agents in comparison to that after embolization of dAVF. However, the final treatment goal (occlusion of active bleeding point or pseudoaneurysm) can be achieved in AVMs even when the nidus is partially occluded.
When using the proximal coil-protected technique, a low (10–20%) concentration of NBCA seems to be better than a routine (25–33%) or high concentration of NBCA. The distance and amount of the mixture delivered depend on the interaction between the viscosity and polymerization time. Reflux is more likely to occur at higher viscosities, while a lower polymerization reaction time results in a longer injection time. As the NBCA concentration in the NBCA-lipiodol mixture decreases, the viscosity increases but the polymerization reaction becomes slower (1516). However, in the coil-protected technique, reflux of the NBCA-lipiodol mixture was almost completely blocked even with a low-concentration NBCA-lipiodol mixture. Therefore, the slower polymerization allowed a slower injection, which in turn made it possible to deliver a sufficient amount of the mixture to the target lesion with reduced distal migration into the draining vein (Fig. 2) (161718).
This study has several limitations. First, it was a retrospective study with a relatively small number of cases. Given that the coil-protected technique is a problem-solving technique rather than a front-line method for transarterial embolization, a prospective and comparative study was difficult to implement. Nevertheless, we believe that our results are unlikely to be affected by selection bias because all cases were registered in the prospectively maintained neurointerventional database with descriptions of the procedural details and complications. Therefore, we cautiously suggest that our results may provide more options for embolization methods in the treatment of neurovascular shunt diseases.
In conclusion, the coil-protected technique can be used as a safe and effective method for liquid embolization, especially in patients with various neurovascular shunt malformations who could not be successfully treated with conventional techniques.
Go to :
 XML Download
XML Download