

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The infrarenal abdominal aorta is the most common location for aneurysmal dilatation (1). The standard definition for an infrarenal abdominal aortic aneurysm (AAA) is a transverse aortic diameter > 3 cm. Other studies have used a different definition of 1.5 to 2.0 times the normal adjacent aortic diameter (2).
Due to a high risk of aneurysmal rupture, repair is considered for AAA > 5.5 cm in diameter (3). Traditionally, open surgical repair has been considered as standard treatment for AAA. However, endovascular aneurysmal repair (EVAR) with stent-graft has now rapidly expanded as primary treatment for AAA since its first report by Parodi et al. (4) almost 30 years ago. A previous retrospective observational study for patients who underwent AAA repair concluded that a decline in AAA rupture and short-term AAA-related mortality was partly related to the introduction and expansion of EVAR (5).
In this review, we will thoroughly discuss EVAR as a treatment for AAA, including pre-procedural considerations for successful EVAR, technique of EVAR, and EVAR-related complications. In addition, the pathophysiology of AAA will be also presented to deepen the understanding of EVAR.
Risk Factors and Pathophysiology of AAA
Old age is the most potent risk factor for AAA. Increasing risk has also been noted with longer smoking history, male sex, high blood pressure level, concomitant peripheral artery disease, carotid disease, and family history of AAA (678). Although various risk factors have been documented, the steps of the pathological process that contribute to the development of AAA are poorly understood. Several pathologic processes have been identified as responsible for the development of AAA. Traditionally, atherosclerosis has been considered as major underlying pathology for the development of AAA. However, current studies suggest multifactorial pathophysiology, including genetic, environmental, hemodynamic, and immunologic factors (9). On a histological level, inflammation, vascular smooth muscle cell apoptosis, extracellular matrix degradation, and oxidative stress are related to AAA development and progression (11011). Moreover, autoimmunity may also play a role in the development and progression of AAA (12).
Aneurysmal dilatation of the aorta can develop in both the thoracic and abdominal aortas. AAA, particularly developed along the infra-renal abdominal aorta, is much more common than thoracic aortic aneurysm (TAA), at least nine times higher in incidence (19). Structural difference of vascular wall between thoracic and abdominal aortas could be the reason for higher incidence of AAA than TAA (13141516).
Decision to Treat AAA
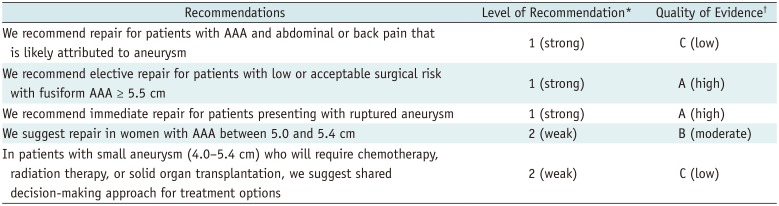
The decision to treat AAA is based on patient's clinical presentation and aneurysm status. According to the society for vascular surgery practice guidelines, anatomical treatment such as open surgical repair or EVAR is indicated with strong recommendation level in case of ruptured AAA, symptomatic unruptured AAA, and large AAA > 5.5 cm in diameter (Table 1) (7). If the aneurysm size is small and the patient has no symptoms relevant to AAA, early anatomical treatment have failed to show significant long-term survival benefit (17181920212223).
Anatomical Considerations for EVAR
Anatomical suitability is the key factor for successful EVAR. When performed in patients with suitable anatomy, EVAR has proven to be effective in preventing aneurysm-related death. Aortic neck, aneurysm morphology, and iliac artery anatomy should be considered for successful EVAR.
Aortic Neck Anatomy
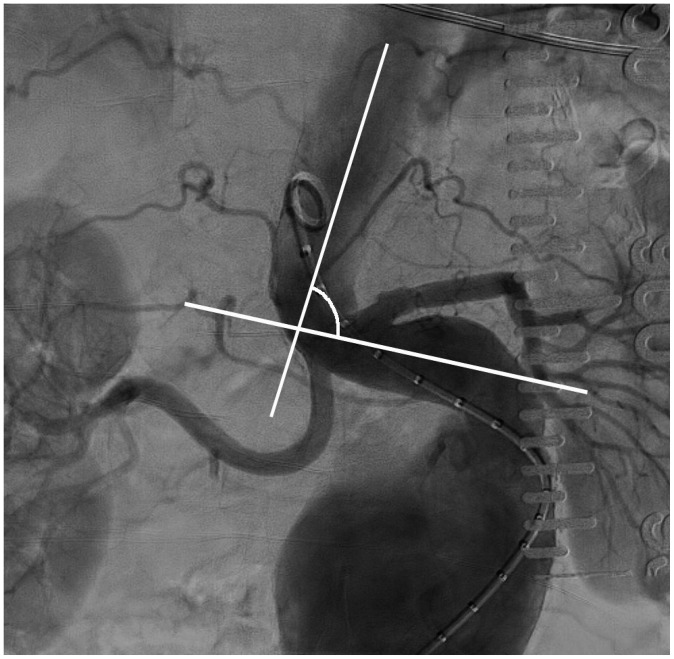
Aortic neck anatomy greatly affects device delivery, deployment, aneurysm exclusion, and long-term durability of the stent-graft because the aortic neck is the proximal fixation site for the stent-graft and the most important factor in determining successful EVAR (24). The length, angle, presence of calcification or thrombus, and the diameter and shape of aortic neck should be carefully considered. The aortic neck length is defined as the distance from the lowest renal artery to the top of the aneurysm. Aortic angle is defined as the angle between the flow axis of the supra- and infrarenal aortas (aneurysmal neck) (Fig. 1).
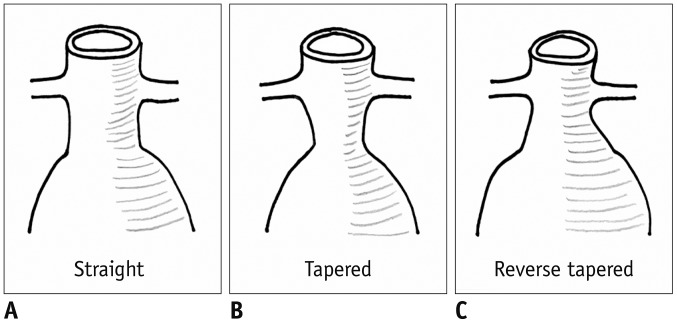
Generally, longer aortic neck > 1.5 cm, wider aortic angle > 150°, and healthy aortic neck without calcification or thrombus are considered as the favorable anatomy for successful EVAR. In contrast, shorter aneurysmal neck < 1.0 cm, narrower aortic angle < 120°, diseased aortic neck with calcification or thrombus > 50% of neck circumference are considered as unfavorable or hostile anatomy and classically not indicated for EVAR (25). The shape of the aneurysmal neck also has a great importance for successful outcome. The shape of the aneurysmal neck is determined by the difference of the diameter between the proximal and distal aneurysmal neck. Accordingly, the shape may be straight, tapered, or reverse tapered (Fig. 2). Usually, reverse tapered neck which shows greater distal aortic neck diameter than proximal one showed a complicated outcome and required more meticulous imaging surveillance after EVAR (252627).
Aneurysm Morphology
Aneurysm anatomy refers to aneurysmal angle, presence of intraluminal mural thrombus, and branching vessels from the aneurysm. Aneurysmal angle is the most acute angle in the line through the central lumen between the lowest renal artery and aortic bifurcation (24). Generally, as aneurysmal tortuosity increased, the aneurysmal angle is decreased. A small aneurysmal angle makes stent-graft delivery and deployment difficult.
Intraluminal mural thrombus of AAA is a known factor responsible for not only AAA progression and rupture, but also an increased risk for cardiovascular events. This might be related to leukocytes, proinflammatory cytokines, and proteolytic enzymes contained in the thrombus burden, which can be released into the circulation (2829). Intraluminal mural thrombus is usually soft and sometimes can be broken during EVAR and can induce distal embolism.
Branching vessels from the aneurysm, including inferior mesenteric artery, lumbar arteries, and median sacral artery, are considered as a major collateral pathway responsible for type II endoleak after EVAR. The number of patent lumbar arteries, patent inferior mesenteric artery, and cross-sectional area of the aorta around the ostium of the inferior mesenteric artery are suggested as predictors for type II endoleak after EVAR (303132). However, there are controversies for prophylactic embolization of branching vessels to prevent type II endoleak.
The diameter of the distal aorta should also be considered during pre-EVAR planning. Previous guidelines recommended that the distal aorta diameter should be larger than 20 mm for placement of a bifurcated stent-graft (33). A narrow distal aorta has been known as a key risk factor for late endograft limb occlusion and subsequent acute limb ischemia after EVAR (34).
Iliac Artery and Common Femoral Artery Anatomy
Anatomy of iliac and common femoral arteries is another main concern for stent-graft delivery, distal sealing, and patency of EVAR. The tortuosity and diameter of the iliac artery, presence of atherosclerotic lesion along the iliac artery, and length of the common iliac artery should be considered for adequate EVAR.
The tortuous iliac artery is associated with an increased risk for graft limb occlusion after EVAR (3536). Iliac artery tortuosity could be quantified using the iliac tortuosity index, which is determined by dividing the distance along the central lumen line from the aortic bifurcation to the common femoral artery by the shortest distance. An index > 1.6 could be defined as severe tortuosity, and adjunctive vascular stenting should be considered to enhance stent-graft patency after EVAR (2437).
Smaller iliac artery diameter particularly due to atherosclerotic lesion with calcification, could make the engagement of the delivery system into the abdominal aorta difficult. In case of complete occlusion, EVAR with aorto-uni-iliac stent-graft concomitant femoro-femoral bypass surgery could be considered when passage of device is impossible (38).
Stent-Graft
The types of stent-graft are diverse, based on the level of fixation and location of stent-graft skeleton. A suitable device selection for various AAAs is as important as the anatomy of AAA for successful outcome after EVAR.
Suprarenal Fixator vs. Infrarenal Fixator
Stent-graft can be divided into two groups based on the level of graft fixation to the aortic wall. Suprarenal-fixating devices attach the stent-graft to the aortic wall at the suprarenal aorta, with metallic struts or barbs placed in the bare stent portion superiorly extended above the fabric-covered stent-graft. Infrarenal-fixating devices attach the stent-graft at the infrarenal abdominal aorta, with barbs placed on graft fabric (Fig. 3). Generally, devices with suprarenal fixator are more useful and recommended in AAA with unfavorable proximal aortic neck such as shorter and more angulated neck, neck with calcification and mural thrombus, and reverse-tapered configuration (7). Devices with infrarenal fixator can be applied onto the long proximal aortic neck appropriately.
Although suprarenal fixator devices seem to be more efficient in various situations, there is a concern regarding the bare struts or barbs crossing the renal artery or other visceral artery origins which could lead to target organ damage such as renal or visceral infarctions. However, previous studies have shown no significant difference in the risk of post-EVAR complications between supra- and infrarenal-fixating devices, although suprarenal-fixating devices could be associated with a very small incidence of immediate occlusion of renal and visceral arteries (394041).
Endoskeleton vs. Exoskeleton
Endoskeleton stent-graft is a device with metallic stent framework located inside of tubular graft fabric while the exoskeleton stent-graft has a metallic stent framework outside the tubular graft fabric (Fig. 3).
Although there is little difference in aneurysmal exclusion between the two stent-graft designs, stent-graft with the exoskeleton design might be related to an increased arterial stiffness which is one of the independent predictive factors for cardiovascular events including hypertension. The endoskeleton stent-graft design shows a minimal effect on arterial stiffness which may result in a reduced risk of end organ injury after endovascular treatment (4243).
EVAR Technique
Planning
Adequate sizing and planning are pre-requisites for optimal EVAR procedure. Not only anatomy of AAA, but also access site should be considered before the delivery of stent-graft system.
Pre-procedural measurement is important for choosing a precise stent-graft. Stent-graft size is selected by overestimating the diameter of the proximal and distal landing zones by 10–20% to improve early outcome after EVAR (44). The diameter of proximal and distal landing zones should be measured using the minor axis from outer to outer (from adventitia to adventitia) margin, even with the presence of mural thrombus within the arterial lumen. Stent-graft oversizing > 30% might be related to device migration and late aneurysmal sac expansion (45). Iliac artery diameter should be considered to secure distal fixation and prevent endoleak from inadequate distal sealing. Iliac tortuosity and aortic bifurcation diameter should also be considered to prevent stent-graft occlusion after implantation due to unexpected stent-graft kinking.
Arterial Access
Although lower-profile systems have currently become available, a larger arterial access, usually > 12-Fr sheath size, is still required for EVAR compared with other endovascular procedures. Therefore, an adequate arterial access might be regarded as a touchstone for EVAR.
Generally, ultrasound (US)-guided common femoral artery cannulation is recommended for precise puncture and can reduce access site complication (46). US makes direct visualization of the common femoral artery and femoral artery bifurcation possible. Furthermore, compressibility at designated access level can be assessed with an US probe. Confirmation of adequate puncture site (around 12 o'clock direction) at the anterior arterial wall without arterial calcification can also be possible with US (Fig. 4).
Percutaneous Endovascular Aneurysmal Repair
With increasing experience and advances in lower profile delivery systems, percutaneous endovascular aneurysmal repair (PEVAR) became a popular procedure, replacing the surgical cut-down procedure. PEVAR can be performed under conscious sedation or local anesthesia with only stab incision around the groin area. US evaluation of bilateral common femoral arteries and US-guided arterial access are paramount for successful PEVAR outcome. Puncture over arterial wall calcification should be avoided. For PEVAR, a pair of suture-mediated vascular closure device, Proglide (Abbott Medical, Abbott Park, IL, USA) is usually required for each common femoral artery access site.
The outcome and advantages of PEVAR have been validated by several previous studies. The PEVAR trial has shown that it is noninferior to standard open femoral artery exposure (cut-down) (47). Retrospective review of 4112 patients who underwent PEVAR or conventional EVAR via surgical cut-down showed that PEVAR was associated with a shorter operative time, shorter hospital stay, and fewer wound complications (48). Despite an additional cost related to vascular closure devices, PEVAR may not only be cost-effective due to reduced hospital stay, but also minimizes surgical trauma as well as increases patient's satisfaction because it is less painful and more aesthetic (49). Because PEVAR does not require general anesthesia and can be rapidly performed, it can be successfully performed also for unstable patients with ruptured AAA. Therefore, if there is no contraindication, PEVAR should be primarily considered as a method for EVAR in both stable and unstable patients (50).
Branch Vessel Embolization
Branch arteries from AAA could be embolized before EVAR to prevent retrograde and persistent pressurization of aneurysmal sac after stent-graft placement. These branching arteries include accessory renal, inferior mesenteric, lumbar, and internal iliac arteries (IIA). Moreover, to extend distal fixation on external iliac artery, planned IIA occlusion can be performed unilaterally or bilaterally.
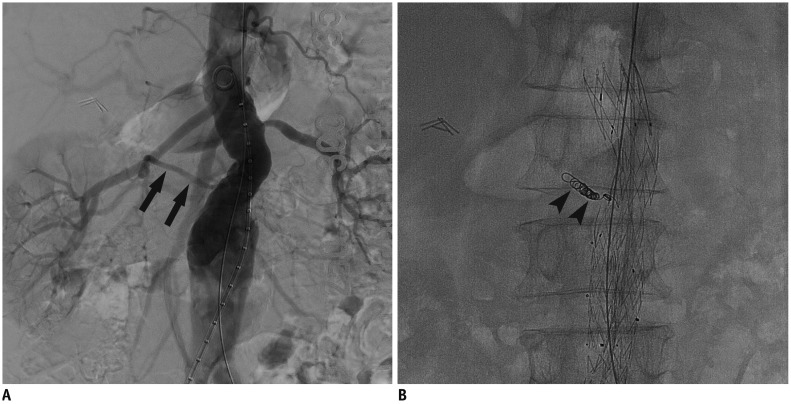
Although the effectiveness of preventive embolization of aortic branches is controversial (51), patients with inferior mesenteric artery diameter > 3.0 mm or lumbar artery diameter > 2.0 mm can be the candidates for undergoing preventive embolization (Fig. 5) (52).
IIA occlusion has a substantial risk of significant ischemic complication in approximately 25% of patients. The incidence of ischemic complication after bilateral IIA occlusion is significantly higher (53). To reduce complication rate, several procedures can be used. First, a staged embolization can be performed weeks before EVAR to provide time for collateral development to lower the risk of pelvic ischemia, particularly for patients considering bilateral IIA embolization. Second, IIA preservation technique such as iliac branching graft or other advanced techniques (e.g., sandwich technique) can be used (2453).
EVAR Procedure
Even though procedural steps might be different according to the stent-graft systems and manufacturers, EVAR procedure can be summarized as follows: 1) common femoral artery access, 2) full digital subtraction aortogram for confirming the length of aneurysm with a calibrated catheter, 3) ancillary procedure such as branch vessel embolization, if indicated, 4) sheath insertion via delivery system over stiff guidewire, 5) confirming an orifice of bilateral renal arteries after insertion of main body delivery system into proximal neck, 6) main body stentgraft deployment, 7) gate cannulation from contralateral common femoral artery access site for contralateral limb stent-graft, 8) contralateral limb stent-graft deployment after confirming length of stent-graft, 9) ipsilateral limb extension after confirming IIA orifice, 10) ballooning with compliant balloon to expand and attach the stent-graft to the native vessel wall at both proximal and distal ends as well as at the point of graft overlap, 11) completion aortogram to find any large post-EVAR endoleak and to confirm the patency of all graft components.
The delivery system and sheath for main body graft is usually larger than those for contralateral limb stent-graft. Therefore, healthier and larger iliofemoral arteries should be selected for main body insertion. Because the guidewire for sheath and delivery system insertion is extremely stiff except for the distal part, the guidewire should not be inserted too much and the location of the guidewire should be carefully monitored during procedure.
Precise confirmation of the renal artery orifice is a very important step to preserve renal perfusion. It is helpful to set an adequate angle to confirm renal artery orifice with changing C-arm angle to align top markers of graft onto a virtual line (Fig. 6). Although the delivery system is technically improving, relocation of the stent-graft after opening the delivery system is difficult. Therefore, a placement of the main-body graft should be performed carefully, particularly in patients with the angulated proximal neck.
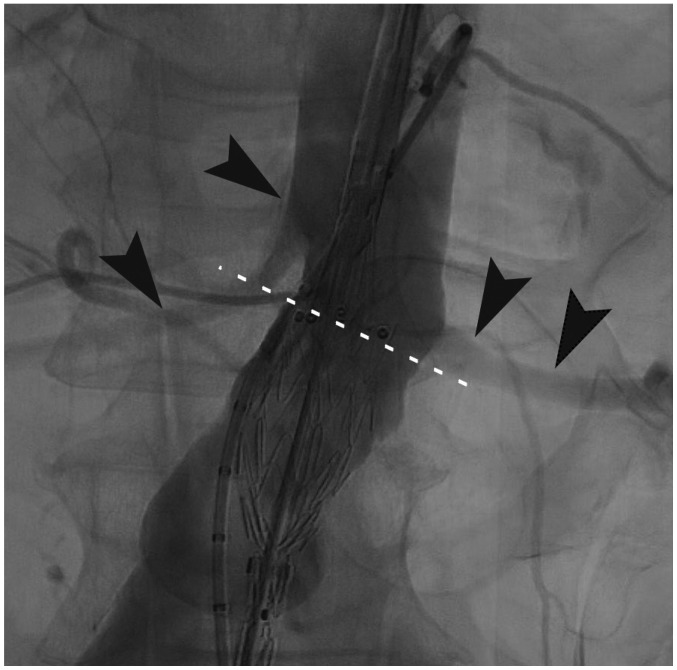
Gate cannulation for contralateral limb stent-graft is also technically demanding and a time-consuming step, particularly in patients with large AAA or very tortuous iliac artery. If gate cannulation fails, snare technique can be used through a contralateral access site (Fig. 7).
Advanced EVAR Technique
Advanced EVAR technique refers to a technique used for AAAs which are considered anatomically unsuitable for conventional EVAR. Chimney technique and periscope technique can be performed to overcome challenging proximal landing zone. Customized stent-graft, fenestrated graft, and branched stent-graft can be also used for inadequate landing zone (54). However, a lack of long term data and complexity of procedure are obstacles for deciding and performing such advanced techniques.
EVAR Complications
Complications may occur during or after EVAR for AAA. Access vessel injury, improper stent-graft placement related complications, and post-implantation syndrome might occur during or immediately after EVAR. During follow-up, stent-graft migration, endoleak, limb occlusion of stent-graft, and stent-graft infection might be observed (55).
Access Vessel Injury
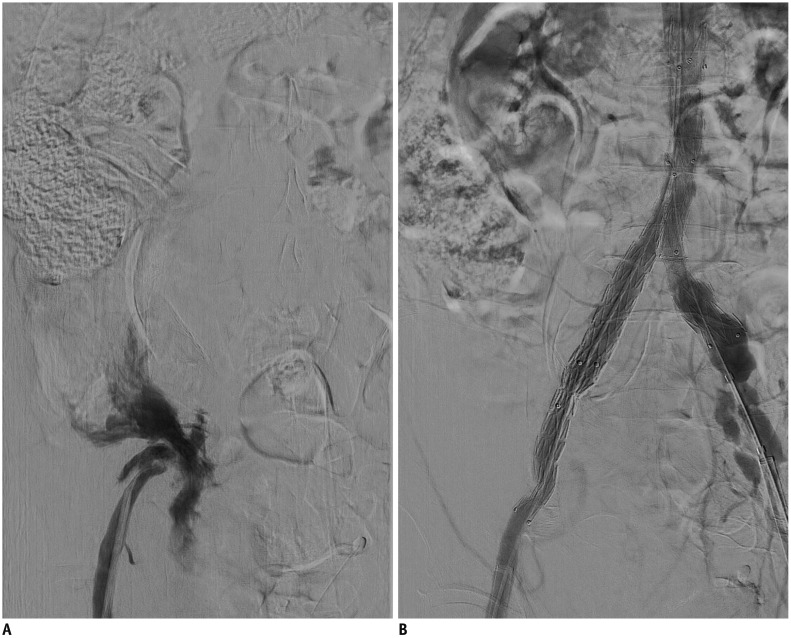
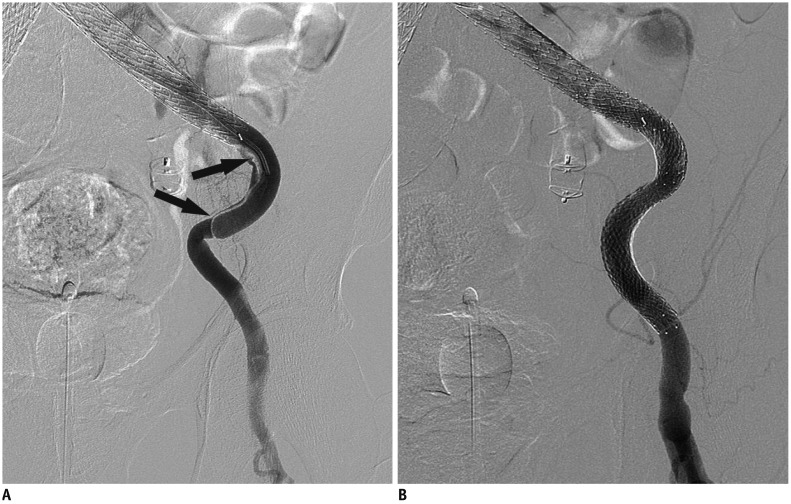
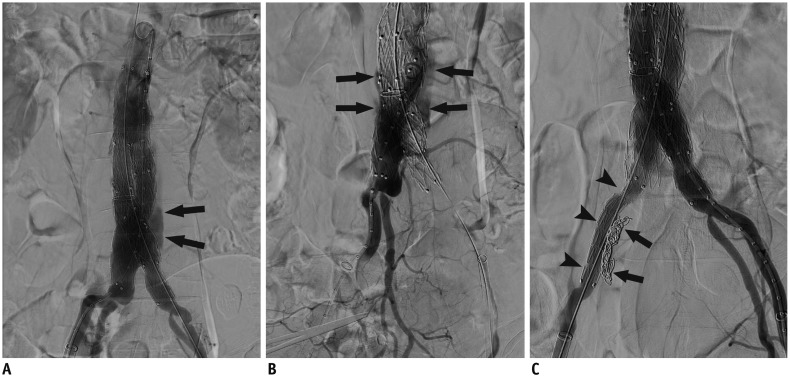
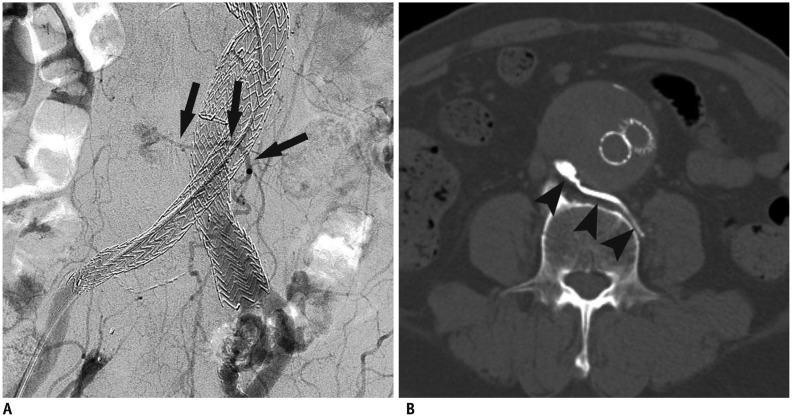
Access vessel injury, including iliac and common femoral artery injury can occur during EVAR. Iliac artery rupture or dissection can also occur during vascular access or EVAR procedure by a delivery system or large angio-sheath. Vascular calcification, diminished diameter, and severe tortuosity of the iliac arteries are reported to be associated with an increased incidence of access vessel injury (56). Iliac artery rupture during EVAR is related to high mortality rate and increased length of hospital stay (Fig. 8) and iliac artery dissection might cause early limb occlusion (Fig. 9). Therefore, prompt stent-graft deployment should be considered for iliac artery rupture and an additional vascular stenting is required for iliac artery dissection.
Improper Stent-Graft Placement
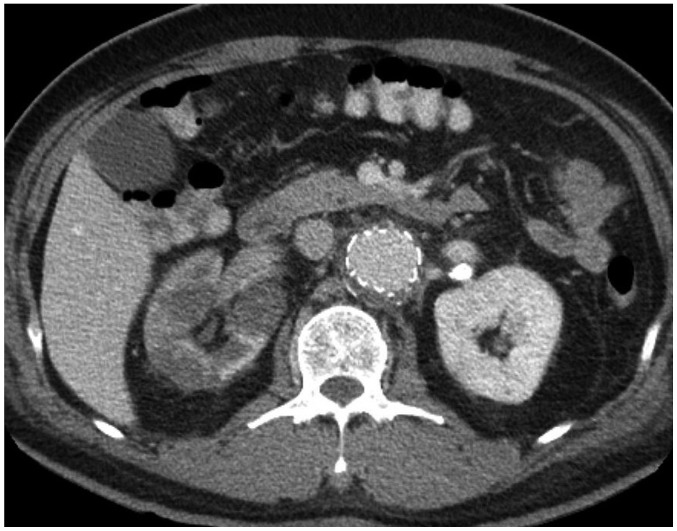
Accurate placement of stent-graft at the proximal aortic neck is important for successful outcome after EVAR as well as for preservation of perfusion through the side branches. Improper stent-graft placement is more frequent in hostile proximal neck anatomy, particularly in the angulated neck. If stent-graft is placed too high in the proximal aortic neck, renal arteries can be occluded and may cause ischemic complications in the kidney (Fig. 10). Conversely, if stent-graft is placed too low in the proximal neck, particularly in patients with reverse-tapered neck, a caudal migration of the stent-graft can occur during or immediately after EVAR, resulting in massive type Ia endoleak. To prevent improper stent-graft placement, an adequate angulation of C-arm and meticulous evaluation about the location of proximal neck are mandatory.
Post-Implantation Syndrome
Post-implantation syndrome is an inflammatory response following EVAR. Post-implantation syndrome can be diagnosed when fever (> 38℃) lasts more than 1 day with leukocytosis (white blood cell count > 12000 µL) and negative blood culture (57). Symptoms of post-implantation syndrome are flu-like in nature and manifest clinically as systemic inflammatory response, characterized by fever, leukocytosis, and elevated C-reactive protein, tumor necrosis factor-alpha, and interleukin-6 levels. The incidence of post-implantation syndrome ranges from 13% to 60% (58).
The proposed pathophysiologic factors are various: injury of the endothelium during EVAR, bacterial translocation due to transient sigmoid colonic ischemia, contrast-induced neutrophilic degranulation, endovascular instrumentation of the mural thrombus, development of new thrombus within aneurysmal sac after stent-graft placement, and a specific type of graft fabric, particularly in stent-graft made with woven polyester (5960).
The clinical course of post-implantation syndrome is usually benign and treatment consists of only surveillance and aspirin to reduce inflammation. However, aggressive anti-inflammatory drugs including steroids, could be required when patients show extensive inflammatory symptoms. Antibiotics are not usually required for most cases (5758).
Stent-Graft Migration
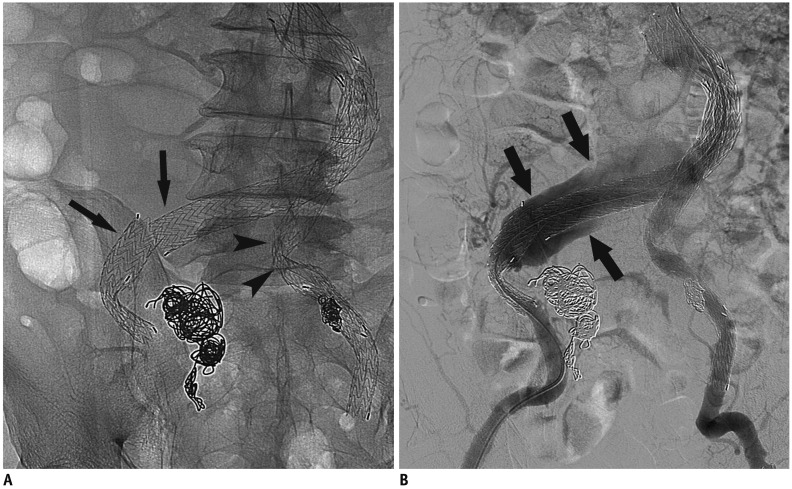
Displacement of stent-graft > 5–10 mm from its original fixation site can be defined as stent-graft migration (58). Proximal stent-graft migration is an insidious and late complication, which may result in type Ia endoleak, re-expansion of AAA, and eventually fatal aneurysmal rupture. Proximal stent-graft migration and late-onset type 1a endoleak can occur any time even after successful EVAR, requiring life-long surveillance (Fig. 11). Large AAA with short and angulated necks which were treated especially with older version of stent-graft shows higher risk for proximal stent-graft migration (61). Most proximal stent-graft migrations can be managed by endovascular methods such as proximal extension with aortic cuffs or large balloon-expandable stents to augment the stent-graft to the aortic wall. Recently, endoanchors can be used to secure stent-graft on the aortic wall to prevent stent-graft migration in case of AAA with short neck (< 10 mm). This procedure can be also prophylactically performed.
Endoleak
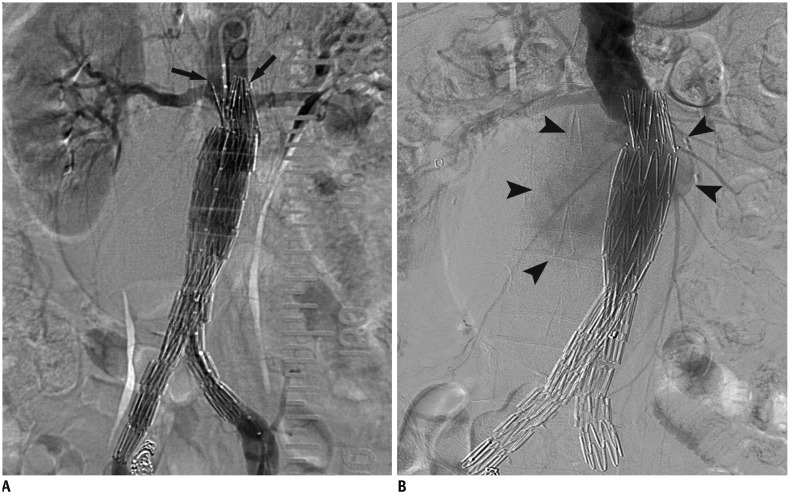
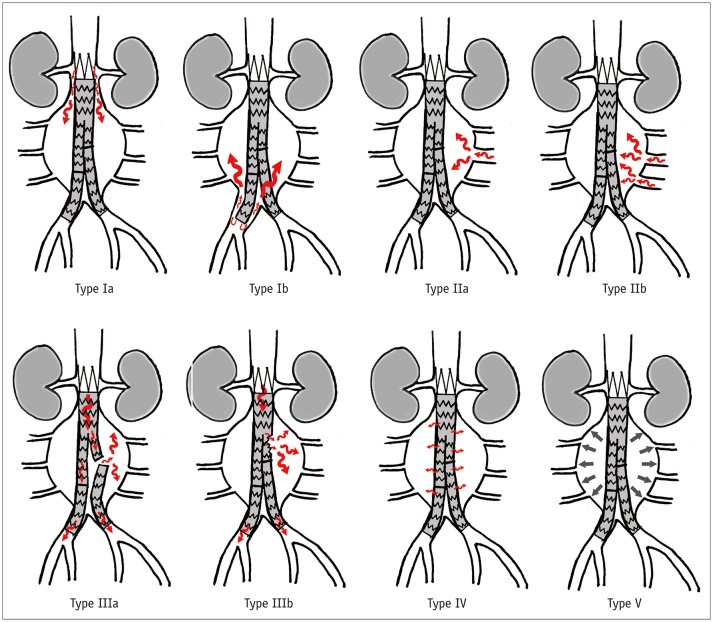
Endoleaks are the most common complications following EVAR. Endoleaks are defined as continuous blood flow and/or pressurization of aneurysmal sac, resulting in failure of treatment, continuous AAA growth, and rupture of the aneurysmal sac. Endoleaks can be classified into five different types in terms of routes of continuous perfusion to the aneurysmal sac. Type I endoleak occurs due to incompetent seal at the proximal (type Ia) and distal attachment (type Ib). Type II endoleak is persistent retrograde blood flow to the aneurysmal sac through a patent single (type IIa) or multiple (type IIb) aortic side branches such as the inferior mesenteric artery or lumbar arteries. Type III endoleak can be defined as structural failure of stent-graft, such as separation of modular components (type IIIa) or graft fabric tear (Type IIIb). Type IV endoleak is defined as transient blood flow to the aneurysmal sac through graft fabric porosity. Type V endoleak means continuous and gradual aneurysmal sac expansion without an evidence of contrast leak, a phenomenon known as endotension, on surveillance imaging (Fig. 12). Type II endoleak is the most common type of endoleak, with a reported incidence ranging from 14% to 25.3%. Type I and III endoleaks occur at 0.6–13% and 0.9–2.1%, respectively. Type IV and V endoleaks are rare (62).
Endoleaks are the most common cause for secondary intervention after EVAR. The initial management of type Ia endoleak is an additional stent-graft attachment to native aortic wall with a large compliant balloon. Other treatment with large balloon-expandable metallic stent or aortic cuffs can be applied to reinforce and extend the proximal sealing zone. Endoanchor can also be applied to secure proximal attachment of the stent-graft to the aortic wall. Conversion to open repair is not recommended unless rupture of significant uncorrectable improper stent-graft placement occurs (7). For persistent type Ia endoleak, other endovascular techniques such as embolization with liquid embolic agent (N-butyl cyanoacrylate or ethylene vinyl alcohol copolymer) or coils, chimney technique for renal artery, and branching stent-graft, or surgical conversion could be considered. Type Ib endoleak can be managed by repeated stent-graft attachment to the arterial wall with a compliant balloon. Stent-graft extension to the external iliac artery can also be performed to treat type Ib endoleak. Embolization for IIA might be required in case of stent-graft extension to the external iliac artery (Fig. 13).
Management of type II endoleak is indicated when persistence of endoleak is accompanied with continuous aneurysmal sac expansion. Embolization for the parent aortic side branches which serve as route for continuous perfusion and pressurization as well as for nidus within aneurysmal sac, should be performed (Fig. 14).
With introduction of new generation of stent-grafts, the incidence of type III endoleak is significantly reduced (63). Although the incidence of type III endoleak is lower than that of type I or II endoleaks, type III endoleak is considered dangerous because it is associated with an increased risk of aortic rupture (Figs. 15, 16). Type III endoleak can be managed with endovascular techniques such as placing additional stent-graft over the disconnection or ballooning at overlap zones to secure modular connection (764).
Type IV endoleaks are usually self-limiting and treatment is not required. For type V endoleak, endovascular re-lining with additional stent-graft or surgical conversion should be considered if continuous aneurysmal sac growth presents (58).
Acute Limb Occlusion
Acute limb occlusion has been reported in 0.4–11.9% of patients who underwent EVAR for the treatment of AAA (758626566). Although new generation of stent-grafts may lower the incidence, acute limb occlusion still remains one of the major adverse events causing secondary intervention, extended hospitalization, and mortality after EVAR (67). Causes for limb occlusion include extreme oversizing of the limb stent-graft, kinking of stent-graft within the iliac tortuosity, hemodynamically significant out-flow impairment from unsolved steno-occlusive lesion or dissection in external iliac artery, and injury at the arterial access site (766).
Acute limb occlusion after EVAR can be managed by endovascular methods or surgery. Endovascular methods include stent-graft limb extension, reinforcing stent placement over stent-graft limb kinking, additional angioplasty or stenting for outflow obstruction, and revascularization of occluded limb with bare stent or re-lining with stent-graft (Fig. 17). Moreover, catheter-directed thrombolysis or thrombectomy can sometimes be performed despite a risk of distal embolization of the outflow tract. Surgical options include femoro-femoral bypass, axillo-femoral bypass, and open embolectomy (5866).
Stent-Graft Infection
Stent-graft infection has been reported in 0.3–3.6% of EVAR-treated patients (62). The mortality rate of stent-graft infection is high and ranges from 25% to 50% (58). The cause of stent-graft infection is different based on the time of presentation. Intra-procedural contamination could be related to early onset of infection. Remote site infection and colonization on stent-graft might be a cause for delayed stent-graft infection.
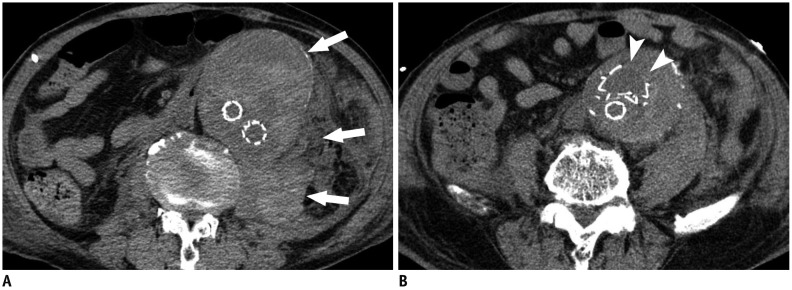
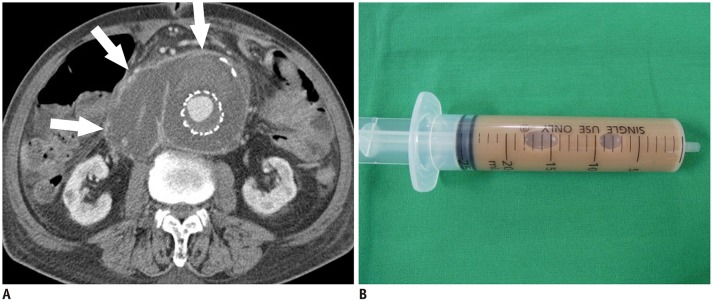
Diagnosis can be made by combination of clinical, radiological, and laboratory findings. Fever, leukocytosis, pus-natured fluid collection, or soft tissue infiltration around the stent-graft, presence of aorto-enteric fistula or erosion, and infected false aneurysm are diagnostic clues for stent-graft infection (Figs. 18, 19) (5868).
Aggressive surgical management is usually indicated for stent-graft infection, including stent-graft removal, debridement of infected tissue, and arterial flow reconstruction for preservation of distal flow. Based on clinical situation, conservative intravenous antibiotics can be administered. The duration for antibiotic treatment can be several weeks, months, or years. Sometimes life-long antibiotic suppressive treatment might be required (68697071).
Issues Related to Radiation and Contrast Materials
As endovascular technique and devices are getting improved and indications for EVAR even in complex AAA are expanding, several concerns regarding the length of procedure, radiation hazard, and iodinated contrast agent-induced complications are also increasing. Furthermore, improved survival after EVAR also increased requirement for radiation-based imaging surveillance such as CT angiography for timely detection of EVAR-related complications and for monitoring residual aneurysmal sac (72).
Recent technical advancement enables image fusion and three-dimensional patient-specific roadmap (Fig. 20). Image fusion for which a pre-procedural CT angiographic image can be overlaid onto an intra-procedural live fluoroscopic image, can facilitate three-dimensional navigation even in patients with complex AAA anatomy. This technique can reduce radiation dose, the amount of contrast agent, and procedure time (7374).
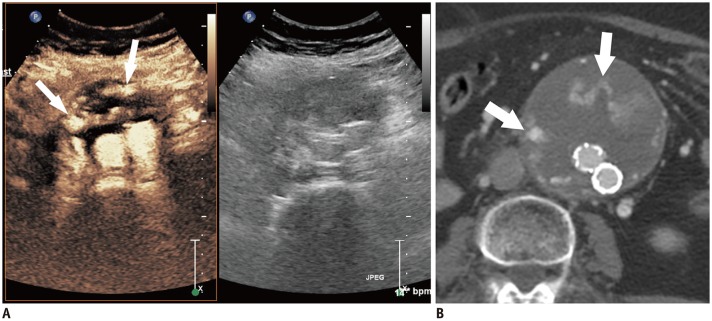
New generation ultrasound contrast agent (USCA) composed of gas microbubbles encapsulated by phospholipid shell (Sonovue®, Bracco, Milan, Italy), showed an improved diagnostic capability for EVAR-related complications. Therefore, contrast-enhanced ultrasound (CEUS)-based EVAR follow-up protocol is considered a safe and effective method, showing similar or better diagnostic capability in the identification and follow-up of endoleaks after EVAR (Fig. 21). As a result, CEUS allows a reduction of the number of CT angiography in surveillance and can reduce radiation hazard and complication related to iodinated contrast agent (7576). In most recently updated guidelines from European Federation of Societies for Ultrasound in Medicine and Biology, CEUS using this new USCA is recommended not only for the detection and characterization of endoleak but also for the follow-up of AAA endoleak with the strongest level of recommendation (77).
Results after EVAR
Several randomized controlled trials which compared EVAR with open repair have failed to reveal superiority of EVAR in terms of long-term advantage over open repair, although EVAR showed a significantly lower early mortality rate and shorter stay for intensive care unit (Table 2) (787980). Considering previous studies performed EVAR using an early version of stent-graft which was not as good as recently used one, long-term results after EVAR might be improved as stent-graft is upgraded.
CONCLUSION
Minimally invasive EVAR for AAA has now become a mainstream treatment for AAA. With advancement of device and endovascular technique, indications of EVAR are becoming wider and clinical outcome is getting better even in complex AAA and various clinical scenarios.
Understanding the significance of the anatomical feature of AAA, adequate planning for individual AAA, and performing essential ancillary procedures are all important. Knowledge on the characteristics of different types of stent-grafts is crucial to select the most appropriate device to complete exclusion of AAA from the aortic circulation.
Operators who are willing to perform EVAR as a treatment for AAA, should be aware of overall procedural steps of EVAR and possible adverse events after EVAR. Extensive knowledge regarding an adequate management for various complications after EVAR could improve the procedural outcome and makes EVAR a safer procedure.







 XML Download
XML Download