

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Colposcopy is an investigation to evaluate cervix of woman with abnormal cervical cytology or high-risk HPV [12]. During colposcopy, a colposcopist will apply 3%–5% acetic acid solution and/or Lugol's iodine solution to cervix to delineate the transformation zone and to inspect for any areas of abnormal squamous or glandular epithelium. A “colposcopic impression” is generally made by the colposcopist based on the most severe area identified. Biopsy would be carried out for histopathologic examination to confirm the colposcopic impression. Although colposcopic impression plays important role in further management, many studies demonstrated that the accuracy of the process varied upon the experience of the colposcopists [34]. The sensitivity for detecting high-grade lesion and cancer of cervix (CIN2+, cervical intraepithelial neoplasia grade 2 or worse) ranged between 64%–99% and the specificity of only 30%–93% [5].
To minimize the variation, several criteria were created. Among these, Reid Colposcopic Index (RCI) is the most commonly used. The lesion is scored by 4 features: color, margin, vessels, and iodine stain. The RCI had better efficacy than colposcopic impression, with the sensitivity ranged between 74%–97% and specificity between 91%–95% [67]. However, some researchers doubted the role of iodine stain to predict CIN2+ in the RCI because it can stain golden yellow in both low- and high-grade cervical lesions. This may lead to low predictive value of this feature in predicting CIN2+. Base on this suspicion, Boonlikit [8] studied the efficacy of RCI with or without iodine stain to predict high-grade cervical lesion and reported the same results. Another study by Hong et al. [9] modified the RCI by replacing the iodine stain with location of abnormal lesion in transformation zone. The diagnostic values of the modified RCI were comparable to those of the original RCI [9].
In 2005, Strander et al. [10] introduced a new colposcopic scoring system “Swede Colposcopic Index (SCI)”, which added lesion size to the other 4 features of lesion that are used in the RCI. Supplementary Table 1 shows the features and scores assigned in the SCI which consist of acetouptake, margin and surface, vessels, lesion size, and iodine [10]. The original study by Strander et al. [10] reported each of these features had good diagnostic performances. The sensitivity to predict CIN2+ when the score was ≥5 was 100%, that all high-grade lesions were detected, and the specificity was 90% if the score was ≥8 [10]. Another subsequent study compared the RCI and SCI and found the SCI was more flexible to be used in clinical settings than RCI. The SCI had 2 cut-off values: 5 when a high sensitivity was aimed (to detect most lesions) or 8 when a high specificity was required (to diagnose CIN2+) [7].
However, obtaining the score from some features in these 2 indices was not practical in routine practice, such as, to measure lesion size in millimeters (in SCI) or to use iodine stain (in RCI and SCI). So, a use of other features which are easier but still maintain or improve the efficacy than the original indices would be useful. We modified the SCI by replacing iodine stain with the location of lesion. The measurement of lesion in millimeters was also omitted and substituted by area of involvement. The efficacy of this modified Swede Colposcopic Index (MSCI) was studied.
MATERIALS AND METHODS
This retrospective study was approved from the institution Ethics Committee of Faculty of Medicine Vajira Hospital, Navamindradhiraj University (No. COA53/2560) for research involving human subject. Inclusion criteria were women who attended Colposcopy Clinic at Faculty of Medicine Vajira Hospital due to abnormal cervical cytology between January 2013 and July 2017. The women must have satisfactory colposcopy with completely visible transformation zone and cervical abnormalities if any. We excluded women who were pregnant at the time of colposcopy, had no or poor quality of cervicographic images, had no document of colposcopic impression or pathological report.
Data from medical records and cervicographic findings including cervical images during the colposcopy were collected and reviewed. As a routine practice in our colposcopy clinic, images of whole cervix before and after acetic acid application were taken under low-power magnification. Abnormal lesions were then inspected under low- and high-power magnification before photo taking.
We created a MSCI by replacing iodine stain with the location of lesion (outer half of transformation zone, inner and/or outer half of transformation zone, invasion to endocervical canal) on the basis of high-grade lesion usually occur in near new squamocolumnar junction [11]. The measurement of lesion in millimeters was replaced by a number of cervical quadrants involved (1, 2, ≥3) depend on a basis of large lesion tend to be a high-grade lesion [12]. Using MSCI, all images were evaluated and each factor was scored by its degree of abnormality by an author (N.R.) who was blinded to cytologic result, colposcopic impression, and pathologic result. The author who evaluated cervicoghaphy by using this index was a gynecologic oncological fellowship who was well-trained and had experienced in colposcopy. Scoring of each factor was assigned from the lesion which had most severe feature. Table 1 and Fig. 1 show the 5 features used in the MSCI and degree of abnormality (level 1–3) which consist of acetouptake, margin and surface, vessels, lesion size, and location of lesion. For the convenience of practice, the score was assigned as 1, 2, and 3 for the mild, moderate, and severe abnormalities correlated with level respectively. Total summation of assigned score was 15 points.
Table 1
Modified Swede Colposcopic Index

![]()
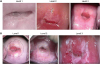 | Fig. 1(A) Lesion size as each level. (B) Location of lesion as each level; black line as an old squamocolumnar junction line. Green line as a new squamocolumnar junction line. Yellow line as divided half of the transformation zone line.
|
Demographic data of the women, results of cervical cytology, colposcopic impression, and pathology of cervix were collected. In a woman with multiple cervical tissues (from biopsy or curettage, or conization), the most severe pathology would be used. Cervical pathology was divided into 2 groups: 1) low-grade lesion including normal, cervicitis, or CIN1; 2) high-grade lesion including CIN2 or more severe lesions.
Sample size was calculated based on a 95% expected sensitivity of the MSCI. By assigning α value of 0.05 and the power of 80%, at least 178 women were required. We added 20% to the calculated sample size for any missing data. Therefore, a total sample size of at least 220 women was to be included.
Statistical analysis was performed using STATA version 13 (StataCorp, College Station, TX, USA). Logistic regression was used to compare the function of each factor to predict high-grade lesion and presented as odds ratios (ORs). The OR of each feature was summed in the first model whereas the assign score of each feature was summed in the second model. The diagnostic performances of both models to detect CIN2+ were compared using the receiver operating characteristic (ROC) curves. The efficacy of the MSCI including sensitivity, specificity, positive predictive value, negative predictive value, and accuracy using the second model at different cut-off point scores was examined. The ability of each and all features to detect CIN2+ was analyzed with Cox & Snell R2.
The reliability of MSCI was assessed by intra-observer and inter-observer, using kappa value to evaluate the reliability of interpretation (low-grade vs. high-grade) and intraclass correlation coefficient (ICC) to evaluate the reliability of scoring value. The intra-observer variation was evaluated in gynecologic oncology fellow (N.R.) who initially scored the 220 by using the MSCI and subsequently assessed again later in a different time. The inter-observer variation was assessed by comparing the performance between the gynecologic oncology fellow (N.R.) and senior gynecologic oncologist (K.P.).
RESULTS
From 409 women who underwent colposcopy during the study period, 189 were excluded, 2 were pregnant, 3 did not have colposcopic impression, and 184 cases had no available or poor quality of cervicographic images. A total 220 cases met all inclusion criteria and were included in the study. The mean age was 40.14±10.14 years (range, 17–77 years). The most common abnormal cytology was low-grade squamous intraepithelial lesion, 88 cases (40%). Malignant cytology was found in 7 women: 6 cases of squamous carcinoma and 1 of adenocarcinoma. The histological diagnoses of cervix with abnormal cytology were high-grade lesion in 114 cases (51.8%), and low-grade lesion in 106 cases (48.2%) (Table 2).
Table 2
Patient characteristics (n=220)
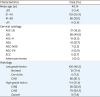
AGC-FN, atypical glandular cells-favor neoplastic; AGC-NOS, atypical glandular cells-not otherwise specified; ASC-H, atypical squamous cells cannot exclude high-grade squamous intraepithelial lesion; ASC-US, atypical squamous cells of undetermined significance; CIN, cervical intraepithelial neoplasia; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion; SCC, squamous cell carcinoma.
![]()
Cervicography of these women was scored by MSCI. The OR of every feature in the MSCI correlated well with the severity level which were significantly predictive of high-grade histology. The OR of location of lesion of level 1 could not be obtained because no high-grade lesion was observed in this particular group (Table 3). The ability of all features to predict high-grade lesion by Cox & Snell R2 was 0.61. The function of each feature to predict high-grade lesions in order of its ability by Cox & Snell R2 were margin and surface (0.55) followed by acetouptake (0.47), vessels (0.38), lesion size (0.19), and location of lesion (0.19).
Table 3
Odds ratio estimates for high-grade lesion and assigned score

CI, confidence intervals; NA, no appropriate, no high-grade lesion was observed in the location of lesion at level 1.
![]()
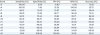
The first and second models had excellent and comparable efficacy with area under curves of 0.94 and 0.95 respectively (p-value=0.28) (Fig. 2). The efficacy of the second model at different cut-off points for high-grade lesion are shown in Table 4. The most appropriate cut-off score for predicting high-grade lesions was 11 points with sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of 82.2%, 96.2%, 96.0%, 85.0%, and 90.0% respectively. At this score, all cases of cancer were detected whereas no normal or cervicitis were observed. Only 4 cases with CIN1 were over-diagnosed.
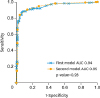 | Fig. 2ROC curve for modified Swede Colposcopic Index and high-grade lesions.AUC, area under the curve; ROC, receiver operating characteristic.
|
Table 4
The efficacy of modified Swede Colposcopic Index at a different cut-off score for high-grade lesion
![]()
The reliability of MSCI assessed by the intra-observer variation revealed the kappa value of MSCI at cut-off point 11 was 0.87 and ICC of MSCI score was 0.87 (95% confidence interval [CI]=0.76–0.94). The inter-observer variation of MSCI comparing between the gynecologic oncological fellowship (N.R.) and senior gynecologic oncologist (K.P.) in 120 cases showed the kappa value 0.7, and ICC 0.8 (95% CI=0.71–0.86).
DISCUSSION
Colposcopy is widely used to evaluate cervix in women with abnormal cervical cytology [1]. The colposcopic impression which is commonly practiced as a standard step in colposcopy has some limitations that it requires training, experience, and continual practice in certain number of women in order to maintain one's skills [13]. The colposcopic index is a method to reduce this limitation of the subjective interpretation of the colposcopists especially the beginners. Among a few colposcopic indices, SCI developed by a Swedish group was the latest one. Although the SCI had good overall efficacy, the features of lesion size and iodine stain remained a problem in evaluation [8].
In the present study, we modified SCI by omitting the iodine stain and replacing it by location of lesion because there is evidence that high-grade lesions usually occur near new squamo-columnar junctions [11]. We also replaced the actual size of lesion in millimeter by the extent of cervical involvement represented as quadrants.
We found that an MSCI score of 11 had good efficacy in determining high-grade cervical lesions with 84.21% sensitivity and 96.2% specificity that no cases of cancer were missed. The sensitivity and specificity of colposcopic impression in predicting CIN2+ was 85% and 69%, respectively [4]. Massad and Collins [14] reported the ability of colposcopic impression in term of sensitivity, specificity, positive predictive value and negative predictive value to predict the same outcome was 89%, 52%, 80%, and 68%, respectively. In the present study, the performance of colposcopic impression to predict CIN2+ in term of a sensitivity, specificity, positive predictive value and negative predictive value was 72.8%, 77.4%, 77.6%, and 72.6%, respectively (data not present). Thus, the function of MSCI to predict CIN2+ was superior to colposcopic impressions.
In previous study of SCI, Strander et al. [10] had proposed two differences cut off value to determine CIN2+ at different purpose. Cut of point at 5 was used for screening which had a 100% sensitivity but only 31% specificity, and cut of point at 8 was for diagnosis which raised the specificity to 90% but sensitivity was dropped to 52% [10]. The current study demonstrated that the MSCI could produce comparable efficacy to diagnose CIN2+ with higher sensitivity by one cut of value at 11 points, which was more simple to apply. Furthermore, this MSCI seemed to have higher clinical value in predicting CIN2+ because the new factors included in MSCI was easier to determine and assign a score, as confirmed by a moderate to good level of agreement in the intra-observer and inter-observer reliability [1516].
When using MSCI, the women may be treated with immediate conization, known as “see and treat” technique, because the specificity and positive predictive value were high and over-diagnosis rate was low. The acceptable overtreatment rate which corresponds to the Cochrane Colposcopy and Cervical Cytopathology Collaborative Group [17] should be less than 10%. The over-diagnostic rate of MSCI was 4%, therefore, MSCI was suitable for the “see and treat” technique and can treat high-grade lesions in a single visit situation.
The strength of the MSCI was it was more practical by using easy-to-assess features into the scoring system. The sample size was relative large with good results in predicting high-grade lesions. The MSCI should help colposcopists especially beginners determine high-risk lesion or cervical cancer. However, the study had some limitations. First, all cervicography was collected retrospectively so there might have been some problems with picture quality and maybe had a different dimension of a picture when compared with the real picture during colposcopy. Second, in this study we included only clearly seen transformation zones; we could not use those cervicography from women without clearly visible transformation zones.
In conclusion, the sensitivity, specificity, positive predictive value, negative predictive value and accuracy of MSCI for predicting CIN2+ were high diagnostic value. All features had significance in predicting high-grade lesions. Our colposcopic index has a simple scoring system, good reproducible and could possibly contribute to the skills of beginner colposcopists.
 XML Download
XML Download