

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Globally, an estimated 528,000 new cases of cervical cancer are predicted each passing year, representing 15.7 per 100,000 women in less developed countries and 9.9 per 100,000 women in more developed countries [1]. In Korea, about 3,500 new cases of cervical cancer are recorded every year. The incidence rate of cervical cancer was 9.0 per 100,000 women in 2014, having decreased by 3.9% annually from 1999 to 2014 [2]. Despite these advances, many Korean women have yet to or do not regularly undergo cervical cancer screening (CCS), and these women have been found to be more likely to develop cervical cancer [3].
Organized screening programs for cervical cancer have been shown to contribute to significant reductions of the incidence and mortality rates of cervical cancer [3,4]. Countries with organized screening programs for cervical cancer primarily offer cytology-based Papanicolaou test (Pap test) as a screening modality in target women [4]. In Korea, CCS using Pap test at 2-year intervals has been provided via the National Cancer Screening Program (NCSP) since 1999 to targeted women of ages older than 30 years, extending to those over 20 years of age in 2016. The participation rate for CCS via the NCSP was 40.9% [5], which was low than that in other countries (e.g., 72.3% for the European Union in 2016) [4]. Potentially related therewith, a previous study indicated that non-participants face both psychological burden and practical burden related with the testing procedure [6-8]; that is, CCS involves an invasive pelvic examination to obtain cells from the cervix by a clinician at clinics or hospitals, posing embarrassment and inconvenience.
Human papillomavirus (HPV) testing has been shown to offer better performance in the detection of cervical cancer than cytology testing [9]. However, in conventional HPV testing, women basically undergo the same procedure as that for Pap test, and therefore, the same barriers remain. Recent studies on self-collected sampling that can be performed by the individuals themselves have been actively conducted [10]. That is, as alternative modalities through which to overcome barriers to Pap test, self-collected vaginal sampling (self-sampling) and self-collected urine sampling (urine sampling) for HPV testing have been studied. The performance of self-sampling has been proven to be reliable [11]. Regarding the self-sampling procedure, women insert a sampling kit into the vagina by themselves, and obtain the needed cells using an appropriate technique at a convenient, private location, such as their home or the restroom of a clinic. For this reason, studies suggest that self-sampling may hold the potential to increase compliance rates for CCS by reducing psychological and practical burden thereto [8,10,12]. More recently, urine sampling has been suggested as being potentially more favorable to eliminating reported burdens to CCS considering that urine sampling is as convenient as and less invasive than self-sampling [13-15]. For urine sampling, women urinate in a urine bottle in the bathroom in the same manner as in a basic urine test with which to test for general disease or an sexually transmitted disease.
While self-sampling and urine sampling might be alternative modalities to Pap test through which to increase compliance and adherence to CCS, few studies have been conducted to compare acceptability of these modalities including urine sampling. Therefore, we aimed to explore satisfaction with clinician-collected Pap test, self-sampling, and urine sampling among women. In addition, we explored their preferences for one of these modalities over the others for CCS in subsequent screening rounds.
METERIALS AND METHODS
1. Participants
From July to November 2016, we recruited women aged between 20 and 69 years at the National Cancer Center (NCC) in Goyang city, Republic of Korea. Participants with a history of hysterectomy or cervical cancer or who were in menstruation were excluded. Study participants were recruited in the waiting room of a clinic at the Center for Cancer Prevention and Detection at the NCC, where NCSP invitees undergo cancer screening, including CCS. Before undergoing a Pap test, research staff introduced the purposes and procedures of this study to eligible participants, and written consent was obtained from willing participants. To compare the 3 modalities for CCS, all participants first received a Pap test by a clinician in the clinic, and performed urine sampling by themselves in the usual manner. After collecting both cervix and urine specimens, they performed self-sampling by themselves in the bathroom next to the clinic. Our research staff explained how to use of the self-sampling kit through brochures and verbal instructions: women were to insert the sampling kit into the mid vagina, rotate it 3 times, and then, retract it from the vagina. The self-sampling kit comprises a dry, cone-shaped flocked swab (52980C, FLOQSwabs; Copan Italia, Brescia, Italy). This study was approved by the Institutional Review Board (IRB) of the NCC, Korea (IRB No. NCC2015-0066).
2. Data collection and outcome measures
The study participants who underwent all 3 cervical screening modalities were asked to complete a questionnaire designed to survey their perceived satisfaction with the 3 screening procedures. The completion of the self-reported questionnaires took approximately 5–10 minutes.
The survey questionnaire was developed based on previous studies [7,8,10]. Data were collected for each of the 3 screening modalities. Psychological factors (satisfaction, embarrassment, pain, anxiety, discomfort, and trust) were assessed with individual questions for each modality: for example, “How satisfied were you with the self-sampling?” Responses were to be given on a 4-point Likert scale, ranging from “very satisfied” to “very unsatisfied.” For analysis of satisfaction and trust, we defined “Yes” as a Likert score of 1–2 and “No” as a Likert score of 3–4. For analysis of embarrassment, pain, anxiety, and discomfort, we defined “Yes” as a Likert score of 1–2 and “No” as a Likert score of 3–4. To measure screening stress, participants were asked, “How much stress did you experience during the test?” with answers given on a 10-point Likert scale ranging from “not stressful” to “very stressful.”
Data on preferences for 1 of the 3 modalities for CCS in subsequent screening rounds were collected by a single item, “Among the 3 CCS modalities you experienced, which would you like to undergo in the next screening round?” We also examined demographic data, including age, education level, marital status, supplemental medical insurance, regular medical check-ups, and age at first intercourse.
3. Statistical analysis
The collected data were analyzed using SAS statistical software (version 9.4; SAS Institute, Cary, NC, USA), and all p-values<0.05 were considered statistically significant. For comparison of psychological variables (e.g., satisfaction and embarrassment), we used a logistic and a linear generalized estimating equation to adjust for repeat measures among the 3 CCS modalities. Also, we used descriptive statistics using frequencies and percentages or means and standard deviations.
RESULTS
1. General characteristics of the participants
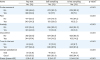
In total, 732 participants were included for analysis. The general characteristics of the participants are presented in Table 1. Of the participants, 50.6% were 20–49 years old, and 49.5% were 50–69 years old. The majority had a university education or more (53.0%), were married (90%), and had supplemental medical insurance for cancer (90.0%). The mean age at first intercourse was 24.2±3.77 years.
Table 1
General characteristics of the participants (n=732)

![]()
2. Satisfaction and psychological distress
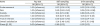
Psychological satisfaction and distress toward CCS are presented in Table 2. All variables were significantly different among the 3 CCS modalities. Overall satisfaction was highest for urine sampling (94.4%), followed by self-sampling (93.4%) and Pap test (87.2%). Psychological distress, including embarrassment, pain, anxiety, and discomfort, was greater for the Pap test than the other sampling modalities. In particular, embarrassment was highest for the Pap test (53.4%), followed by self-sampling (7.7%) and urine sampling (7.1%). Meanwhile, however, the Pap test garnered the highest trust (93.4%). Stress was highest with the Pap test at 5.01±2.81 on average (0–10 points), followed by self-sampling at 2.12±1.97 and urine sampling at 2.04±2.00 (Table 2).
Table 2
Participants' satisfaction and psychological distress according to CCS modality (n=732)
CCS, cervical cancer screening; Pap test, Papanicolaou test; SD, standard deviation.
*p-value was obtained by type III generalized estimating equation.
![]()
In the crude model, psychological distress with self-sampling and urine sampling was significantly lower than that with the Pap test (Table 3). For both self-sampling and urine sampling, stress with undergoing the test was lower than that for the Pap test (−2.89±0.13; −2.97±0.13, respectively). Overall satisfaction was significantly higher for both self-sampling and urine sampling, compared with Pap test (odds ratio [OR]=2.01, 95% confidence interval [CI]=1.48–3.00; OR=2.47, 95% CI=1.75–3.48, respectively).
Table 3
Comparison of psychological variables according to CCS modality (n=732)
This analysis was conducted by a logistic GEE and a linear GEE statistical analysis.
CCS, cervical cancer screening; CI, confidence interval; GEE, generalized estimating equation; OR, odds ratio; Pap test, Papanicolaou test; SE, standard error.
![]()
3. Preferences for CCS modalities in subsequent screening rounds
Fig. 1 depicts the participants' preferences for individual modalities for CCS in subsequent screening rounds. Of the participants, 52.0% (378 participants) expressed desires to receive self-sampling at their next screening. Grouping the participants according to their preferred modality, we found that the levels of stress experienced with each modality in the present study differed significantly. In particular, those who selected self-sampling for future screening showed the highest levels of stress with the Pap test and the lowest levels of stress with self-sampling. With regard to modality preferences according to satisfaction with each screening modality, those who preferred self-sampling reported the greatest satisfaction with self-sampling (96.0%) and relatively lower satisfaction with Pap test (86.7%).

DISCUSSION
In the present study, we evaluated women's satisfaction with and preference for clinician-collected Pap test and HPV testing by self-sampling and urine sampling for CCS. Both urine sampling and self-sampling garnered significantly higher satisfaction than Pap test performing by a clinician at a clinic. Moreover, psychological distress with self-collected sampling (urine sampling and self-sampling) was significantly lower than that with the Pap test. Preferences for self-sampling in future screening rounds were greater than for both Pap test and urine sampling.
Compared to satisfaction with a clinician-collected Pap test, that with self-sampling was significantly higher in the current study. Our findings of significantly higher satisfaction with self-sampling are in line with those of previous studies [8,16,17]. Virtanen et al. [8] reported favorable experiences of ‘ease of sampling taking,’ ‘no pain,’ ‘less embarrassment,’ and ‘less fear or anxiety’ with self-sampling in more than 70% of subjects. Several studies reported that self-sampling for CCS may have the potential to address both psychological barriers (e.g., embarrassment, anxiety, and concern for pain) and practical barriers (e.g., clinic appointment, trust in the test, and available time) associated with the Pap test [6,8,12]. With regard to these barriers, Waller et al. [7] reported that psychological barriers remained the same among all women regardless of whether they underwent CCS or not, while practical barriers only remained prominent among non-attendees for CCS. In Korea, psychological barriers affecting negative attitudes toward CCS have been raised continuously, as have practical barriers, such as time-consuming nature of testing [18,19]. Moreover, reflecting Asian cultural factors, exposure of the genital area in front of a clinician might lead to more negative attitudes and reduce compliance with CCS [20]. Altogether, we suspect that self-sampling might hold substantial advantages to eliminating psychological barriers associated with the Pap smear test. In addition, an enhanced strategy, such as sending a self-sampling kit via mail to an individual's home, might help to lessen practical issues negatively affecting CCS rates [21,22].
Although disadvantages to self-sampling have rarely been reported, obstacles related to inserting the sampling kit into the vagina may still remain, depending on age or personal background [23,24]. Similar to our findings of greater satisfaction with urine sampling, a few studies in recent years have reported that urine sampling may be more likely to be accepted as an alternative to the Pap test than even self-sampling as a non-invasive method for conducting CCS [14,15]. Among our findings, distress in regards to pain, anxiety, discomfort, and stress was lowest with urine sampling. More importantly, a meta-analysis of 14 studies revealed that the detection rate of urine sampling for HPV as a causative factor for cervical cancer was similar to that of cervical sampling, indicating that urine sampling could be a viable alternative to Pap test for CCS [13].
In our study, a greater number of women reported desires to undergo CCS with self-sampling in subsequent screening rounds than with the other 2 CCS modalities. While we did not evaluate the reasons for this preference, this finding might reflect less distress and more satisfaction with self-sampling. A study offering self-sampling among non-attendant women for regular CCS screening reported that intentions to undergo CCS in the future were stronger in the self-sampling group (66%) than the Pap test group (10%) [8]. The main reasons reported were convenience/ease, privacy, and less embarrassment, although the Pap test did garner greater trust in regards to the accuracy of its results than self-sampling [8,10], similar to our findings. That is, the acceptability of self-sampling among women may contribute greatly to improving intentions to undergo future CCS and finally with compliance rates for CCS. Indeed, a cohort study with women who do not attend regular CCS reported that the group receiving a self-sampling kit showed significantly higher CCS compliance by up to 30% than the group receiving recall invitations; moreover, compliance rates were similar regardless of age [16,22]. A systemic review study of 16 randomized trials reported that the compliance rate of study groups receiving a self-sampling kit was significantly higher than that of control groups (23.6% vs. 12.6%, respectively) [25]. Interestingly, in the present study, higher satisfaction with urine sampling did not result in greater preferences therefore in subsequent screening. This finding may be attributable to perceptions of urine sampling, in that the urine sampling procedure for CCS is quite different from conventional CCS with the Pap test and too similar to general urine analysis. Thus, the participants may not realize that urine sampling can replace Pap test. In this respect, we argue that further education on cervical cancer and CCS may be required prior to implementing urine sampling for CCS. Accordingly, although intentions do no directly reflect actual participation in CCS, our findings suggest that self-sampling might be more advantageous to improving compliance and adherence with CCS than urine sampling.
Our study should be considered in light of several limitations. First, study participants were recruited when they visited a clinic for CCS screening. Thus, the women likely had favorable attitudes toward CCS, although they participated in using 2 additional CCS modalities with which they had not had prior experience. Notwithstanding, our study was performed using women of targeted for CCS in the NCSP, and each participant underwent all 3 CCS modalities. From this point of view, our results may better reflect the perceptions of alternative modalities for CCS among target women, making them of greater practical use to the NCSP. Second, we did not evaluate study outcomes according to history of CCS experience among the study participants, although test satisfaction might depend on CCS experience. However, based on several studies that reported higher acceptability for self-sampling among non-attendees or irregular-screened women for CCS [25,26], the possibility that the satisfaction was overestimated is low, since study participants already had a clinic appointment and might be less likely to become non-attendees. Third, we evaluated preferences for CCS modalities in subsequent screening rounds instead of actual participation due to the limitation of the cross-sectional study design. Nevertheless, intentions to participate in screening have been found to be associated with actual participation [27]. Several vigorous studies reported that offering self-sampling kit increased participation rate for CCS, especially non-attendees women for CCS [28]. Fourth, we only utilized brush and dry type self-sampling devices, and thus, generalization of our findings might be limited. However, regardless of the type of self-sampling device, self-sampling has been generally accepted for CCS [11,29]. Fifth, the accuracy testing of self-sampling and urine sampling methods in our study have not been conducted. Because of the low rates of abnormal cytology (3 cases of atypical squamous cells-undetermined significance), we only identified that the detection rate of HPV 16/18 was 2.0% for vaginal self -sampling and 1.5% for urine sampling, and 99.1% (95% CI=98.1%–99.6%) for overall agreement for HPV 16/18 between the 2 sampling methods [30]. Asciutto et al. [31] reported that the relative sensitivities for high-risk HPV detection were 96.4% (93.5%–99.2%) for vaginal self-sampling and 83.9% (78.4%–89.5%) for urine sampling compared to clinician-collected sampling. Also, a meta-analysis for the accuracy of urine sampling reported that the pooled sensitivity and specificity of urine detection of HPV 16/18 were 73% (56%–86%) and 98% (91%–100%), respectively [13]. Similarly, a recent study which involved Korean women showed that the relative sensitivity and specificity of urine sampling based on clinician-collected cervical sampling for HPV 16/18 detection were 79.2% (57.9%–92.9%) and 100% (95.3%–100.0%), respectively [32]. Nevertheless, our suggestions of the 2 sampling methods as an alternative to the Pap test based on previous studies and our data can be considered controversial, and thus an accuracy testing study using a much larger population should be conducted. Moreover, a cost-effective analysis is required for the use of self-sampling and urine sampling in an organized CCS program. Finally, standardized test methods for self-sampling and urine sampling are absent in Korea and these test methods may be limited as alternative modalities of Pap test. Both test methods might especially vary depending on when and how samples are collected [32]. Thus, further studies to validate and guarantee the accuracy of these test methods are required.
Despite these limitations, our study, to the best of our knowledge, is the first to compare satisfaction with clinician-collected Pap test and self-sampling and urine sampling based on HPV. To date, the majority of studies have compared Pap test and self-sampling, with few assessing urine sampling. In this context, our findings might provide more useful evidence on urine sampling as an alternative CCS modality. In addition, our study participants used 3 modalities for CCS, which allow us to conduct more exact comparisons of both satisfaction with individual screening modalities and preferences for CCS.
In conclusion, we found that participants were more likely to report satisfaction with alternative methods (self-sampling and urine sampling) for CCS than then conventional Pap test. These finding suggest the possible feasibility and acceptability of the alternative modalities in improving CCS rates. That is, self-sampling and urine sampling might contribute to greater participation among non-attendees in CCS, even in developed countries where compliance is over 70%. Moreover, these alternative methods might be promising ways with which to resolve psychological, cultural, and geographical barriers to CCS in countries with low compliance rates.
 XML Download
XML Download