

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Uterine myoma, also known as fibroid or leiomyoma, is a common benign gynecologic tumor that affects more than 70% of women of reproductive age [1]. Women with uterine myoma are generally asymptomatic and the myoma is detected either during routine gynecologic examinations or incidentally during procedures. Sonography is the most affordable imaging tool to differentiate uterine myoma from other pelvic masses. Patients may undergo hysterectomy or myomectomy for treatment of symptomatic myomas. Similar to endometriosis and adenomyosis, uterine myoma is associated with hormonal imbalance, including increased estrogen or decreased progesterone levels [2]. Uterine myoma symptoms may also share the common pathophysiology of gynecologic malignancies such as endometrial and ovarian cancer [3]. Thus, it seems plausible that a previous diagnosis of uterine myoma may serve as a marker of increased future risk of ovarian cancer.
Epithelial ovarian carcinoma is more common in postmenopausal women aged over 50 years of age [45]. In contrast, hereditary ovarian carcinoma occurs more frequently in premenopausal women [67]. Because of the lack of obvious symptoms, the majority of ovarian cancers are diagnosed at late stages. The carcinogenesis of ovarian cancer is complex and is not yet fully understood. Previous studies reported that continuous ovulation, excessive gonadotropin secretion, retrograde carcinogen transportation, and hormonal imbalance may play a role in the pathogenesis of ovarian cancer [38]. Despite recent advances in surgical treatment, the prognosis of ovarian cancer remains poor, especially in more advanced stages.
To our knowledge, several studies have reported uterine myoma is associated with an increased risk of endometrial [910], or other uterine malignancies [111213]. However, the association between uterine myoma and risk of ovarian cancer remains uncertain. Therefore, this study used a nationwide sample to assess whether women with a previous diagnosis of uterine myoma have an increased risk of developing ovarian cancer.
MATERIALS AND METHODS
1. Data source
The National Health Insurance (NHI) program covers over 99% of the population in Taiwan [14]. This retrospective population-based case-control study was conducted using the data from the National Health Insurance Research Database (NHIRD), which comprised comprehensive administrative and claims data. For privacy and data security, all personal identification numbers in the NHIRD have been encrypted by the National Health Research Institute. In addition, diagnostic and procedural codes were classified according to the International Classification of Diseases, 9th revision, clinical modification (ICD-9-CM) coding system. This study was approved by the Institutional Review Board of the Taichung Veterans General Hospital in Taiwan (approval No. CE13151B-1, Taiwan), and the requirements for informed consent were waived.
2. Study samples
The primary outcome was the occurrence of ovarian cancer during the study period as defined using diagnostic codes. Patients aged 25 years and older with newly diagnosed ovarian cancer (ICD-9-CM code 183) between 2006 and 2010 were identified in the Registry for Catastrophic Illness Patients (RCIP) of the NHIRD. For the completeness and accuracy of RCIP data, at least two gynecological oncologists have to review medical records, laboratory data, and imaging findings before approving a catastrophic illness certificate for ovarian cancer. We excluded ovarian cancer patients with a diagnosis of other cancer because their risk might possibly be reduced by optimal pharmacological or surgical therapy. In addition, cases who underwent oophorectomy (one or both sides) before the index date were also excluded because their risk of ovarian cancer may have differed. The index date was defined as the date of first ovarian cancer diagnosis.
The control group was selected from a random sample of 1,000,000 individuals in the NHIRD claims data. Patients diagnosed with ovarian and other cancers or who had undergone oophorectomy before the index date were excluded. The index date for the controls was defined as the date of the first disease diagnosis. We used frequency-matching based on age group, urbanization level, insurance premium, and index date with a ratio of four controls for one case. A flow diagram of sample selection is shown in Fig. 1.

3. Uterine myoma exposure
The primary exposure of interest in this study was uterine myoma, which was defined as women with a previous diagnosis of uterine myoma (ICD-9-CM 218 or 219.9) with at least three outpatient visits or one hospitalization within the year preceding the index date to increase the diagnosis accuracy. This method has been applied by our group in a previous study on uterine myoma [15]. Uterine myoma was diagnosed based on the patient's medical history, clinical features, bimanual palpation, and ultrasonography. In addition, the Taiwan's National Health Insurance Administration (NHIA) checks the accuracy and completeness of claim data electronically that includes auto-adjudication and profile analysis. Also, a small percentage of all claims is selected for professional review by physicians with various specialties who are contracted with NHIA to peer review the rationality of medical procedures and services.
4. Covariates
The covariates in our analysis included patient's age, urbanization level, insurance premium, comorbidities, hormone replacement therapy (HRT) use, and the number of medical visits.
The urbanization of the patients' residential area was classified into four levels, with 1 indicating the highest level of urbanization and 4 the lowest. Insurance premiums were classified into three levels: ≤15,840, 15,841-45,800, and ≥45,801 new Taiwan dollars (NTD) per month. The insurance premiums were determined according to personal monthly income.
The following comorbidities were selected: hypertension (ICD-9-CM codes 401-405), diabetes (250), hyperlipidemia (272), and endometriosis (617.0, 617.1 or 617.9) that occurred within five years before the index date. In addition, women who took estrogen (estradiol and oestrogen) alone or combined with progesterone within five years prior to their index date were defined as patients with HRT use. The HRT was selected based on the Anatomical Therapeutic Chemical (ATC) system of medications of G03CA03, G03CA07, G03CA57, and G03FA04 from the NHIRD, respectively. However, use of oral contraceptives was not measured in this study. We also calculated the cumulative exposure time of HRT by summing the total number of days of HRT use within the five years prior to the index date. Furthermore, the number of medical visits (outpatient visits and hospitalizations) within 1 year before the index date was also calculated. Because women with prior uterine myoma tend to use healthcare services more than those without prior uterine myoma, which may observe the difference in risk of ovarian cancer.
5. Statistical analysis
Differences in the distribution of characteristics between cases and controls were examined using Student's-t and chi-squared tests as appropriate. Univariate and multivariate logistic regression analyses were performed to estimate the associations between previous uterine myoma and occurrence of ovarian cancer. Odds ratios (OR) and 95% confidence intervals (95% CI) were calculated. The regression models were adjusted for the number of medical visits within the year before the index date. The association of previous uterine myoma with the risk of ovarian cancer in all patients was calculated and stratified analysis by age group and HRT use was conducted. Additionally, we further assessed the impact of surgical interventions for the treatment of uterine myoma on the subsequent occurrence of ovarian cancer in patients with previous uterine myoma. All statistical analyses were two-tailed tests and the level of significance was 0.05. All analyses were performed using SAS 9.3 software (SAS Institute Inc., Cary, NC, USA).
RESULTS
We identified 4,088 newly diagnosed patients with ovarian cancer as cases and 16,348 matched controls without ovarian cancer (Fig. 1). Table 1 shows the distributions of characteristics between the cases and controls after matching by age group, urbanization, insurance premium, and index date. There were no significant differences in hypertension (p=0.736), diabetes (p=0.511), hyperlipidemia (p=0.338), HRT use (p=0.146), and cumulative exposure duration of HRT (p=0.075) between the two groups. The cases were more likely to be diagnosed with endometriosis (2.0% vs 0.8%, p<0.001) and to have medical visits (20.9 vs. 16.9 times, p<0.001) than controls before the index date (Table 1).
Table 1
Basic characteristics of newly diagnosed patients with ovarian cancer and matched controls
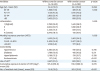
Values are presented as number (%).
HRT, hormone replacement therapy; NTD, New Taiwan Dollars; SD, standard deviation.
*HRT was defined as the use of estrogen alone or combined with progesterone within 5 years before the index date; †Cumulative exposure duration of HRT was calculated only for patients who received HRT.
![]()
Table 2 shows data on the women with previous uterine myoma associated with the subsequent occurrence of ovarian cancer. A prior diagnosis of uterine myoma occurred in 20.7% of cases and in 10.1% of matched controls (p<0.001; Table 2). Women with previous uterine myoma (adjusted OR [aOR]=2.26; 95% CI=2.06−2.49) was significantly associated with subsequent occurrence of ovarian cancer after adjusting for age, urbanization, monthly insurance premium, comorbidities, HRT use, and number of medical visit.
Table 2
Association between previous uterine myoma and subsequent occurrence of ovarian cancer, stratified by age group and use of hormone replacement therapy

CI, confidence interval; HRT, hormone replacement therapy; OR, odds ratio.
*Adjusted for age, urbanization, monthly insurance premium, hypertension, diabetes, hyperlipidemia, endometriosis, HRT use, and number of medical visit; †Adjusted for age, urbanization, monthly insurance premium, hypertension, diabetes, hyperlipidemia, endometriosis, and number of medical visit; ‡Adjusted for urbanization, monthly insurance premium, hypertension, diabetes, hyperlipidemia, endometriosis, HRT use, and number of medical visit.
![]()
After adjustment, the results of the stratified analysis showed that women with previous uterine myoma had a significantly higher probability of subsequent ovarian cancer than that in women without uterine myoma (Table 2). In particular, a higher aOR was observed in patients with previous uterine myoma using HRT (aOR=2.51; 95% CI=2.24−2.82) compared to that in those not using HRT (aOR=1.79; 95% CI=1.51−2.13). The aOR was the highest in patients aged ≥65 years (aOR=4.29; 95% CI=2.86−6.44), followed by that in patients aged 25–39 years (aOR=4.25; 95% CI=3.01−5.99), 40–54 years (aOR=2.16; 95% CI=1.90−2.45), and 55–64 years (aOR=1.91; 95% CI=1.56−2.33).
Furthermore, patients with previous uterine myoma who underwent gynecologic surgery (aOR=0.38; 95% CI=0.31−0.47) had a lower risk of ovarian cancer than that in those patients without uterine myoma after adjustment (Table 3). The occurrence of ovarian cancer was lower in patients with previous uterine myoma who underwent myomectomy (aOR=0.55; 95% CI=0.39−0.77) or hysterectomy (aOR=0.33; 95% CI=0.26−0.42) for treatment.
Table 3
Surgical interventions for uterine myoma and subsequent occurrence of ovarian cancer risk among patients with previous uterine myoma

CI, confidence interval; OR, odds ratio.
*Adjusted for age, urbanization, family income, hypertension, diabetes, hyperlipidemia, hormone replacement therapy use, endometriosis, and number of inpatient/outpatient visit.
![]()
DISCUSSION
This nationwide case-control study observed an association between previous uterine myoma and increased risk of subsequent ovarian cancer. The notable findings of this study are that women with previous uterine myoma had a 2.26-fold increased risk of ovarian cancer compared to the risk in those women without previous uterine myoma, even after adjusting for socio-demographic characteristics and coexisting conditions.
Our finding was consistent with those reported by Danish [11] and Canadian [12] studies indicating that uterine myoma diagnoses were associated with an increased risk of ovarian and uterine malignancies. The risk was higher in women diagnosed with uterine myoma within the period preceding the diagnosis of ovarian cancer. However, increased gynecologic monitoring after the benign diagnosis could not be excluded as a reason for this observation [11]. In addition, women with uterine leiomyoma and endometriosis may also have an increased the subsequent risk of ovarian and other gynecologic malignancies [13]. This may partially explain the association between prior uterine myoma and the occurrence of ovarian cancer.
In the present study, women with previous uterine myoma were predisposed to develop ovarian cancer. A number of women were diagnosed with uterine myoma discovered incidentally during routine gynecologic examinations. Increased gynecologic surveillance among women with uterine myoma may increase the discovery of ovarian cancer or expedite eventual cancer diagnosis [11]. Thus, early uterine myoma detection may also increase the likelihood of the detection of ovarian cancer diagnoses.
In addition to the stratified analysis according to HRT use, an increased risk of ovarian cancer was observed among patients with uterine myoma regardless of HRT use compared to the risk among those women without prior uterine myoma. Similar to the previous reports [1617], our results showed that patients with uterine myoma using HRT had a 2.51-fold increased risk of overall ovarian cancer. However, a recent meta-analysis by Shi et al. [18], suggested that different HRT regimens and duration of HRT use may vary in their association with types of ovarian carcinoma, although the evidence to date is inconsistent. In addition, we also observed a positive association between prior uterine myoma and the risk of ovarian cancer among women not using HRT. Differences in the number of patient medical visits may partially explain the difference observed in the risk of ovarian cancer. Uterine myoma can result in heavy menstrual bleeding and pelvic pain, which may be the main reasons for seeking treatment [19]. Patients developed ovarian cancer after a prior diagnosis of uterine myoma, regardless of HRT use. Thus, increased gynecological symptoms and greater frequency of medical visits may be associated with the subsequent detection of ovarian carcinoma.
In contrast, a previous uterine myoma was strongly associated with an increased risk of ovarian cancer in all age groups and especially in women aged 25–39 and ≥65 years. The variation between age groups may be due to differences in uterine leiomyoma growth by women's age and tumor size at presentation, which may provide an indication as to the likely course of the future tumor development [20]. In addition, ovarian steroids estrogen and progesterone influenced leiomyoma growth, although the underlying mechanisms are unclear [2122]. Previous studies reported that ovarian leiomyomas can be considered malignant ovarian tumors [23]. Thus, it is possible that the pathogenesis of uterine myoma may lead to a risk of ovarian cancer. Unfortunately, our results could not confirm this possibility.
Clear cell carcinoma and endometrioid carcinoma of ovary are related to endometriosis. Endometriosis and uterine myoma are both common estrogen-related gynecological diseases in women of reproductive age. In the study by Chiang et al. [24], the age-adjusted incidences of clear cell and endometrioid carcinoma during 2005-2008 were 1.19 and 1.11 per 100,000 person-years in Taiwan, respectively. In addition, Nezhat et al. [25] reported that women who have symptomatic leiomyoma may be at higher risk for endometriosis. However, data about the coexistence of endometriosis in women with uterine myoma were not available, which may affect the outcome measure.
Our results also revealed that patients with prior uterine myoma who had undergone hysterectomy or myomectomy had significantly reduced risks of ovarian cancer of 67% and 45%, respectively. These findings were consistent with those of previous studies of a reduced lifetime risk of ovarian cancer in women who underwent hysterectomy [2627] or tubal sterilization [27]. A meta-analysis study confirmed that tubal ligation and hysterectomy were associated with a 26%–30% decreased risk of ovarian cancer [28]. In addition, previous studies demonstrated that use of oral contraceptive and hormonal contraception was associated with a reduced risk of ovarian cancer [2930]. However, Gallotta et al. [31] found that the incidence of endometriosis among patients with apparent early stage ovarian malignancies who were referred for optimal surgical procedures was approximately 18%. Our study suggests that this correlation may be even stronger, though this needs to be verified by further studies. Therefore, it is possible that the development of ovarian cancer may be related to the presence of endometriosis, adenomyosis, or fibromatosis.
Several mechanisms for the protective effect of hysterectomy or tubal ligation against ovarian cancer have been proposed. Recent studies suggest that ovarian cancer predominantly arises within the fallopian tubes or the uterus [272832]. Hysterectomy may protect the ovaries from carcinogens ascending from the lower genital tract or fallopian tubes [32]. The risk of ovarian cancer may be altered by the decreased blood supply to the ovaries after surgery, resulting in decreased estrogen levels. Furthermore, surgical prevention may prevent exfoliation of pre-invasive or invasive tissues when surgeons observe abnormal changes in the ovaries during hysterectomies.
A large pooled analysis of 21 prospective studies within the Ovarian Cancer Cohort Consortium (OC3) indicated that age at menopause, endometriosis, and tubal ligation were associated with endometrioid and clear cell tumors; oral contraceptive use was associated with serous and clear cell tumors [33]. However, hormone therapy use and family history of breast cancer were associated with serous and endometrioid tumors [33]. Therefore, significant heterogeneity of risk factors across ovarian cancer subtypes have been observed, and future work is needed to further evaluate risk factors and biomarkers for ovarian cancer subtypes.
Our study had several strengths for evaluating the relationships of previous uterine myoma with subsequent ovarian cancer risk, including a population-based database with a large sample size. First, the case-control design with appropriate case and control matching during the observational period was an appropriate method for evaluating this relationship. Second, multivariate regression analysis was conducted to adjust for potential confounding biases. Third, stratified analysis according to HRT use and age group was used to strengthen our main findings.
This study had several limitations. First, information on the severity of uterine myoma symptoms, patient genotypes (i.e., BRCA-1 and BRCA-2), biochemical measures, and lifestyle factors such as diet, physical activity and smoking were not available for analysis. In addition, detailed information regarding body mass index, pregnancy history, histologic subtype of ovarian cancer, and categories of precursor lesions at diagnosis, such as germ cell, epithelial, stromal, and mesenchymal tumors, was not included in this study. These unmeasured factors may partially influence the occurrence of ovarian cancer. However, we adopted frequency matching to balance the two groups and to minimize the confounding effects of these factors on the relationship with ovarian cancer. Second, diagnostic bias may occur when physicians make a diagnosis without comprehensive information on a woman's previous uterine myoma. To minimize the potential diagnostic bias, we enrolled only patients with at least three outpatient visits or one hospitalization for the treatment of uterine myoma. Third, linking uterine myoma and ovarian cancer without considering other well-known risk/protective factors could impair the entire work.
In conclusion, women with a common benign gynecologic condition, such as uterine myoma, may have an increased risk of ovarian cancer. This study provides evidence that previous uterine myoma is related to an elevated risk of subsequent ovarian cancer. However, a lower risk of ovarian cancer was observed among patients with prior uterine myoma who underwent myomectomy and hysterectomy. Patients should discuss the advantages and disadvantages of treatment options with their physicians when deciding to undergo surgical interventions. Although the relationship between previous uterine myoma and ovarian cancer might not be causal, these findings suggest that women with prior uterine myoma should be made aware of their risk of ovarian cancer. Further research is needed to clarify the effects of uterine myoma on the pathogenesis of ovarian cancer.
 XML Download
XML Download