

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endometrial cancer (EC) is the most prevalent malignancy in industrialized countries, accounting for about 317.000 new cases in 2012 [12]. Incidence is rising, and with up to 81% of EC patients being obese, the global obesity epidemic is one of the leading causes of this increasing incidence [2345]. Obesity mainly leads to low-grade endometrioid endometrial carcinomas (EECs) [3]. Low-grade EEC patients, i.e., grade 1–2, bear around 7% risk of disease-related mortality [6]. On the other hand, patients with high-grade EC, i.e., grade 3 EEC and non-endometrioid endometrial carcinoma (NEEC) bear a 35% risk of disease-related mortality [6789]. Although the 7% of patients with disease-related mortality in low-grade EEC is limited, actual numbers are numerous due to the fact that around 80% of patients present with low-grade EEC. Because a substantial number of disease-related mortality occur in this patient group, improved pre-operative risk stratification to select those low-grade patients with poor outcome is crucial [6789]. In addition to preoperative tumor grade, myometrial invasion (MI) and tumor size, which can be assessed by ultrasound or magnetic resonance imaging (MRI), are important prognosticators in the preoperative risk stratification [1011].
Although the clinical value of cancer antigen 125 (CA-125) in the work-up of EC is questioned in the European Society for Medical Oncology-European Society of Gynaecological Oncology-European Society for Radiotherapy and Oncology consensus guidelines, the Society of Gynecologic Oncology guidelines state that CA-125 measurement can be considered in patients with obesity or co-morbidity that are not fit enough for comprehensive staging [1213]. Moreover, CA-125 has been incorporated in the preoperative prediction model developed by the Korean Gynecologic Oncology Group, adequately identifying EC patients with a normal CA-125 with a low risk (<4%) of lymph node metastasis [1415]. In the current prospective study, we evaluated the prognostic value of CA-125 in relation to established preoperative prognosticators in a large comprehensive cancer region, with a focus on identification of patients with poor outcome in clinically early-stage low-grade EEC patients.
MATERIALS AND METHODS
1. Patients
From September 1st 2011 until December 1st 2013, 432 consecutive endometrial carcinoma patients who underwent surgical treatment at one of the nine participating hospitals in the Netherlands were prospectively included in the PIpelle Prospective ENDOmetrial carcinoma (PIPENDO) study [16]. Except for two centers, the preoperative work-up was standardized. CA-125 testing was advised in all patients. In patients with preoperative low-grade carcinomas, an additional abdominal computed tomography (CT)-scan was performed when CA-125 was elevated. In patients with preoperative high-grade carcinomas, abdominal CT-scanning was performed in all patients, regardless of CA-125 level. According to the Dutch guidelines, surgical staging including lymph node dissection in clinical stage I endometrioid type EC is recommended only in case of clinical suspicion of lymph node metastasis or in case of preoperative high-risk histology (i.e., serous and clear cell carcinomas). Patients without preoperative CA-125 test result were excluded from analysis. The study design followed the reporting of observational studies in epidemiology statement.
2. Data collection
Patient characteristics, including body mass index (BMI), menopausal status, parity, CA-125 level and CT-findings were prospectively collected. Preoperative and postoperative pathology data included histological grade and type, MI, cervical invasion, lymph node metastasis and International Federation of Gynecology and Obstetrics (FIGO) stage. All preoperative biopsy and hysterectomy slides were reviewed by a pathologist with special interest in gynecologic pathology (NV), blinded for patient characteristics and outcome. In case of discrepancy with the original diagnosis the case was evaluated independently by a second pathologist (JB). Discrepancies were resolved at simultaneous consultation. Low-grade carcinomas comprised grade 1 or 2 EECs, high-grade carcinomas comprised grade 3 EECs and NEECs, including serous, clear cell, undifferentiated carcinomas and carcinosarcomas. Patients with proven carcinoma in the hysterectomy specimen, but with a preoperative diagnosis of complex atypical hyperplasia were considered as preoperatively low-grade. Follow-up data, including the presence of recurrence, overall and disease-specific survival (DSS) rate, were collected. Preoperative CA-125 serum levels were determined by radioimmunoassay according to the local protocol in the various hospitals.
3. Statistical analysis
Clinicopathological differences between subgroups were compared using the χ2 and Fisher's exact tests for categorical data and the Mann-Whitney Utest for continuous variables. CA-125 was analyzed as a dichotomous value, with a cut-off value of 35 IU/mL. The association between prognostic features and disease-free survival (DFS) and DSS was determined using Cox regression analysis. Features identified by univariable regression analysis with p<0.20, were used for multivariable regression analysis. DFS was defined as the length of time, after completing primary treatment, during which women survived without any clinical sign of disease recurrence. DSS was calculated from the date of primary treatment to the date of death caused by the disease or, for surviving patients, to the date of the last follow-up. Kaplan-Meier curves for DFS and DSS were generated, for both preoperatively classified low-grade and high-grade patients, comparing patients with normal and elevated CA-125 using the Log-rank test. The p-values less than 0.05 were considered to indicate a significant difference. SPSS version 22 (SPSS IBM, New York, NY, USA) statistical software was used to perform the statistical analyses.
4. Ethical approval
This study is revised by the local medical ethical committee of the Elisabeth-Tweesteden Hospital Tilburg on 11 May 2011 and was exempt from Institutional Review Board (IRB) approval (Protocol 1129, METC, ETZ, Tilburg). This was due to the fact that this was an observational study without subjecting patients to specific procedures. All patients did not object against using their clinical data or tumor material, according to the Dutch law no further patient approval was needed.
RESULTS
1. Patients
A total of 432 consecutive patients with EC were included in the PIPENDO study (Supplementary Fig. 1). One patient with a double endometrial and ovarian tumor was excluded after revision, because uterine origin could not be ascertained. A total of 333 patients underwent CA-125 serum testing (77.3%) and were included for analysis. Of the excluded patients, 42 patients did not undergo CA-125 serum testing, as they were treated in one of the two centers that had not implemented this into their local guideline yet, and 57 patients did not undergo testing despite stated in their guideline. Excluded cases were not statistically different from the study cohort with respect to variables as shown in Table 1 (data not shown). The median age was 66 (range: 41–89). Revised preoperative diagnosis consisted of low-grade EC in 240 (72.1%) and high-grade EC in 93 patients (27.9%). CT-scan was performed in 149 patients and was suspicious for extra-abdominal disease in 29 patients (19.5%). Lymphadenectomy was performed in 73 patients (21.9%). The distribution of FIGO stage was I in 275 patients (82.6%) and stage II–IV in 58 patients (17.4%). Sixty-three patients (18.9%) developed recurrent disease during follow-up and 43 patients (12.9%) died as a consequence of the disease.
Table 1
Baseline characteristics of patients with low-grade and high-grade EC, in association with CA-125 level
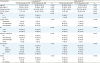
Values are presented as median (range) or number (%).
BMI, body mass index; CA-125, cancer antigen 125; CT, computed tomography; EC, endometrial carcinoma; EEC, endometrioid endometrial carcinoma; FIGO, International Federation of Gynecology and Obstetrics; MI, myometrial invasion; NEEC, non-endometrioid endometrial carcinoma.
*Based on preoperative histological findings.
![]()
2. Preoperative prognosticators
The associations between clinicopathological features and CA-125 in patients with low-grade and high-grade EC are shown in Table 1. In patients with low-grade EC, CA-125 was normal in 177 patients (73.8%, median level 17 IU/mL, range: 3–34 IU/mL) and elevated in 63 patients (26.3%, median level 66 IU/mL, range: 35–1,200 IU/mL). In patients with high-grade EC, CA-125 was normal in 59 patients (63.4%, median level 18 IU/mL, range: 2–34 IU/mL), and elevated in 34 patients (36.6%, median level 58 IU/mL, range: 36–210 IU/mL). In both patients with high-grade and low-grade EC, elevated CA-125 was significantly associated with poor prognostic features including advanced FIGO stage, deep MI and lymph node metastasis, as well as poor outcome including recurrence and disease-related mortality. Most patients recurred either at regional or distant sites, and only a minority experienced a local recurrence.
As preoperative prognostic features were included age, BMI, preoperative tumor grade, tumor type and CA-125 serum level. As shown in Table 2, age, preoperative tumor grade, tumor type and CA-125 were significantly associated with DFS in univariable analysis by Cox regression. In multivariable analysis age, preoperative tumor grade and CA-125 were significantly associated with DFS.
Table 2
Univariable and multivariable analysis of preoperative clinicopathological parameters as prognosticators of DFS
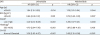
BMI, body mass index; CA-125, cancer antigen 125; CI, confidence interval; DFS, disease-free survival; EEC, endometrioid endometrial carcinoma; NEEC, non-endometrioid endometrial carcinoma; HR, hazard ratio.
*Based on preoperative histological findings.
![]()
As shown in Table 3, preoperative tumor grade, tumor histology and CA-125 were significantly associated with DSS in univariable analysis by Cox regression. In multivariable analysis preoperative tumor grade, tumor type and CA-125 were independently associated with DSS.
Table 3
Univariable and multivariable analysis of preoperative clinicopathological parameters as prognosticators of DSS
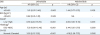
BMI, body mass index; CA-125, cancer antigen 125; CI, confidence interval; DSS, disease-specific survival; EEC, endometrioid endometrial carcinoma; NA, not applicable; NEEC, non-endometrioid endometrial carcinoma; HR, hazard ratio; TS, tumor size.
*Based on preoperative histological findings.
![]()
Multivariable analysis was subsequently performed with both preoperative and postoperative prognosticators, including MI, FIGO stage and the presence of lymphovascular space invasion (LVSI). CA-125 remained independently associated with both DFS and DSS (Supplementary Tables 1 and 2).
3. Outcome based on preoperative tumor grade
In patients with preoperative low-grade EEC, elevated CA-125 was significantly associated with advanced FIGO stage, deep MI, recurrence and disease-related mortality (Table 1). When CA-125 was normal, 14 patients (7.9%) experienced recurrence and 5 patients (2.8%) died due to disease, compared to 12 patients (19.4%, p=0.028) and 7 patients (11.1%, p=0.011) when CA-125 was elevated (Fig. 1).
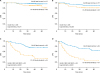 | Fig. 1Kaplan-Meier survival analyses for DSS (A) and DFS (B) in low-grade patients, and DSS (C) and DFS (D) in high-grade patients according to preoperative serum CA-125 levels.CA-125, cancer antigen 125; DFS, disease-free survival; DSS, disease-specific survival; EEC, endometrioid endometrial carcinoma; NEEC, non-endometrioid endometrial carcinoma.
|
In patients with preoperative high-grade EC, elevated CA-125 was significantly associated with advanced FIGO stage, deep MI, recurrence and disease-related mortality (Table 1). When CA-125 was normal, 17 patients (28.8%) experienced recurrence and 13 patients (22.0%) died due to disease, compared to 20 patients (58.8%, p<0.001) and 18 patients (52.9%, p<0.001) when CA-125 was elevated (Fig. 1).
DISCUSSION
Improved preoperative risk stratification is crucial in the worldwide increasing incidence of EC [2345]. In the current prospective multicenter study we have demonstrated that elevated preoperative CA-125 is associated with several poor prognostic features, and is an independent prognosticator for reduced DFS and DSS. Separate analyses have shown that patients with low-grade EC and elevated CA-125 had a significantly lower DFS and DSS compared to patients with low-grade EC and normal CA-125 and therefore should be considered as high-risk endometrial carcinoma. Whether adjuvant treatment should be applied in these high-risk patients needs to be determined.
The study strengths are that it comprises a large-scale prospective, multicenter study cohort including all consecutively treated patients with EC within a regional network of collaborating hospitals [16]. A second strength is that all preoperative and postoperative histology was reviewed by a pathologist with special interest in gynecologic pathology, blinded for patient characteristics and outcome. Third, this study evaluates CA-125 expression across subgroups, providing information about the value of CA-125 in addition to histology-based risk stratification. As a consequence, an additional subgroup is identified that should be considered as high-risk. Finally, this study focuses on preoperative markers, analyzing what factors contribute to risk stratification in a preoperative setting. A limitation of this study included the fact that 22.7% of patients were excluded because of lack of preoperative CA-125 testing. However, these patients did not differ from the studied group. Furthermore, histopathological data on lymph node status is limited, because — due to national guidelines — lymphadenectomy is only performed in a selective population. However, based on existing data, routine lymphadenectomy in early-stage low-grade patients has no beneficial effect on survival, and results in an increased surgical related morbidity. On the contrary, a substantial number of patients with lymph node metastasis in low-grade EC is currently missed as demonstrated by the poor outcome in a selected group [17].
Currently, for the preoperative identification of low-grade patients as high-risk, assessment of MI and tumor size are recommended in international guidelines [1213]. However, in a preoperative or intraoperative setting, the assessment of deep MI by MRI, transvaginal ultrasound or frozen section is accompanied with several challenges. Regarding assessment of deep MI by transvaginal ultrasound, sensitivity and specificity are 82% and 81%, respectively; for MRI, sensitivity and specificity are 82% and 86%, reflecting only moderate diagnostic performance [1819]. Moreover, moderate inter-observer agreement is reported for both ultrasound (k-value: 0.45–0.58) and MRI (k-value: 0.39) [2021]. For intra-operative assessment of MI by frozen section, sensitivity and specificity are high: 85% and 97%, respectively [22]. However, time constraints and costs of performance should be taken into account when performing this procedure. Because preoperative assessment of serum CA-125 level is easily accessible compared to imaging techniques and interpretation does not require high-level expertise, it could be an attractive alternative for measurement of MI or tumor size to preoperatively identify high-risk patients.
CA-125 was elevated in 29.1% of patients, comparable to earlier studies showing 11%–34% of EC patients revealing elevated CA-125 serum levels [23242526]. In our study, elevated CA-125 was associated with poor prognostic features including advanced FIGO stage, deep MI and lymph node metastasis. On the contrary, no association was found with preoperative tumor grade and our results demonstrated that elevated CA-125 was associated with poor outcome in both low-grade and high-grade EC. Although no association was found with preoperative tumor grade, other studies did find associations with postoperative tumor grade [2327]. This could be contributed to the finding that preoperative assessment of tumor grade is discordant with postoperative tumor grade in 33%, and in 8% a discordance between preoperative low-grade and surgical high-grade exists [28].
In multivariable analysis analyzing variables that are available before surgery, age >65, high tumor grade and elevated CA-125 were associated with reduced DFS; high tumor-grade, NEEC-histology and elevated CA-125 were associated with reduced DSS. Among the strongest prognosticators for lymph node metastasis is the presence of LVSI [293031]. However, assessment of LVSI is based on histological examination of the surgical uterine specimen, and thus cannot be reliably determined preoperatively. Instead, preoperative clinical markers, such as age, preoperative tumor grade and CA-125 serum levels could be used in patient counseling and informed decision making.
In addition, preoperative immunohistochemical biomarkers have been subjected to extensive research [32]. Of these biomarkers, immunohistochemical expression of estrogen receptor and progesterone receptor have prospectively been validated as independent prognosticators for lymph node metastasis and poor outcome [6]. Also, L1 cell adhesion molecule expression has retrospectively been validated in large cohorts as a strong preoperative prognosticator for high-risk features including non-endometrioid histology, LVSI, and poor outcome [3334]. Until now, none of these biomarkers has been incorporated in standardized routine care. To optimize the clinical applicability of these immunohistochemical biomarkers, the combined value should further be elucidated. Furthermore, the prognostic value of immediate postoperative and follow-up CA-125 serum levels remains unclear, and future research should focus on the ability of follow-up CA-125 to detect recurrent disease.
Concluding, this study has shown that elevated CA-125 is an independent preoperative prognosticator for poor outcome in EC patients, even in patients identified as low-risk based on preoperative histology. Preoperative assessment of CA-125 could be an attractive additional tool, next to tumor histology and assessment of MI/tumor size in preoperative risk stratification. Patients with low-risk EC and elevated CA-125 represent a group with substantial risk of poor outcome and should be considered as high-risk endometrial carcinoma. Whether adjuvant treatment should be applied in these high-risk patients needs to be determined.
 XML Download
XML Download