

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Uterine cervical cancer is the fourth most common malignancy in women worldwide, and accounts for 7.5% of all female cancer-related deaths with estimated 266,000 deaths in 2012 [1]. Definitive concurrent chemoradiotherapy (CCRT) is a standard therapy for locally advanced cervical cancer at stages IIB–IVA according to the International Federation of Gynecology and Obstetrics (FIGO) [2]. At earlier stages (FIGO stage IB–IIA), radiotherapy (RT) with or without chemotherapy has shown survival outcomes comparable to those following radical surgery, with a lower risk of complications [3]. Thus, RT has been one of the standard treatment options for uterine cervical cancer.
Although the significance of residual disease after RT remains undefined, a previous study reported that uterine cervical cancer which does not regress promptly (post-treatment 1 to 3 months) was likely to recur. However, they only used physical examination or biopsy without imaging, and the timing of evaluation was varied [4]. A recent retrospective study demonstrated that 10% of the patients with FIGO stage IB2–IVA who received CCRT showed the presence of residual tumor based on magnetic resonance imaging (MRI) checked at 3 months after therapy [5]. They reported that residual tumor size of ≤2 cm was a significantly good prognostic factor for overall survival (OS) (hazard ratio [HR]=0.26; 95% confidence interval [CI]=0.08–0.86; p=0.027), and local progression-free survival (PFS) (HR=0.10; 95% CI=0.03–0.39; p=0.001). Although MRI is more effective than computed tomography (CT) in evaluating the response after CCRT [6], MRI assessment is still challenging with the limitation of false positives detected due to post-treatment changes [7]. Also, false-positive results might cause unnecessary repeated imaging and salvage treatments.
The 18F-fluorodeoxyglucose positron emission tomography (18F-FDG PET) which measures the metabolic viable disease can be a better choice as the follow-up modality after RT in uterine cervical cancer patients [8]. A number of prospective and retrospective studies have evaluated the use of 18F-FDG PET to assess the response and predict survival following RT in uterine cervical cancer. However, the significance of post-RT 18F-FDG PET response evaluation has not been well-established, and the procedure is not routinely performed in clinical settings. Therefore, we performed a systematic review and meta-analysis to evaluate the prognostic value of post-treatment 18F-FDG PET in patients with uterine cervical cancer who received definitive RT with or without chemotherapy.
METHODS
This systematic review and meta-analysis were done in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines [9]. The protocol was registered to the International Prospective Register of Systematic Reviews (registration No. CRD42018104860). The research question of the present meta-analysis was as below: “Could response evaluation using post-RT 18F-FDG PET predict the survival outcomes in patients with cervical cancer?”
1. Literature search
PubMed and Embase databases were searched up to July 22, 2018. Search queries included synonyms of “uterine cervical cancer,” “18F-FDG PET,” and “radiotherapy” as the following (uterus OR uterine) AND (cervix OR cervical) AND (FDG OR fluorodeoxyglucose) AND (PET OR "positron emission tomography") AND (radiation OR chemoradiation OR radiotherapy OR chemoradiotherapy). There was no language restriction. To find the additional relevant studies, the references of retrieved articles were also checked.
The inclusion criteria was based on the Patient/Intervention/Comparator/Outcome/Study design criteria [9]: 1) “patients” with uterine cervical cancer; 2) response outcomes of post-treatment 18F-FDG-PET as “intervention”; 3) no “comparator” on this study; 4) OS or PFS as “outcome”; and 5) “study design” as original articles or brief report. The exclusion criteria were as follows: 1) not in the field of interest; 2) insufficient survival information; 3) inclusion of recurrent cases; and 4) overlapping study population.
2. Data extraction and quality assessment
The characteristics of study, clinicopathological factors, and 18F-FDG PET were extracted using a standardized form: 1) study characteristics: first author, year of publication, institution, enrollment period, number of patients, and design (prospective or retrospective/consecutive enrollment); 2) clinicopathological characteristics: age, stage, pathology, treatment, interval between the date of therapy and 18F-FDG PET, response, endpoint, and follow-up period; and 3) 18F-FDG PET characteristics: vendor, model, injected dose, uptake time, scan time, reconstruction methods, and attenuation methods. There was a study which reported disease-specific survival instead of OS, it was also included for OS analysis with flexibility [10].
The methodological quality of included studies was assessed using Quality in Prognostic Studies (QUIPS) tool [11]. Two independent reviewers performed literature selection, data extraction, and quality assessment. If there was any discrepancy, it was resolved via discussion.
3. Statistical analysis
Primary endpoint was OS, and secondary endpoint was PFS. As an effect size of prognostic value, HRs from comparisons amongst response groups (i.e. complete metabolic response [CMR], partial metabolic response [PMR], stable metabolic disease [SMD], and progressive metabolic disease [PMD]) were used. HRs with 95% CIs from univariate Cox regression were extracted. If not available, CIs were indirectly calculated based on p-values from log-rank test [12]. When Kaplan-Meier curves were presented, HRs and their CIs were extracted using Engauge Digitizer version 10.4 (http://markummitchell.github.io/engauge-digitizer/) and methodology by Tierney et al [13]. Of note, we included 2 studies having suspected overlapping study population, as they reported HRs from the comparison of different response groups [1014].
The HRs were meta-analytically pooled using the random-effects model. Heterogeneity was evaluated with Higgins I2 [15]. Assessment of publication bias was not feasible, because of the paucity of studies in each subgroup [16]. Statistical analyses were done with Review Manager (version 5.3.5; The Cochrane Collaboration, London, UK). The p-value <0.05 was considered statistically significant.
RESULTS
1. Study characteristics
Fig. 1 describes the study selection process. Initial literature search retrieved 853 articles, of which 26 articles were considered potentially eligible. After full-text review, 15 articles were excluded as following: No survival analysis (n=8), overlap in study population (n=5), or inclusion of recurrent cases (n=2). Ultimately, 11 original articles with 1,104 patients were included [1014171819202122232425]. The characteristics of the study, clinicopathological factors, and PET are summarized in Tables 1 and 2. Since Schwarz et al. [10] included 2 study populations (retrospective and prospective cohorts) and reported results from each, we pooled their results separately in all synthesis. To avoid confusion, we specified the number of study cohorts (a total of 12) instead of the number of studies (a total of 11). Among the 12 cohorts, 4 were prospectively enrolled. The FIGO stages ranged from I to IV. The median interval between the end of treatment and PET ranged from 1.0 to 5.0 months. The metabolic responses were classified as CMR, PMR, or PMD upon visual assessment (qualitative) in 10 cohorts. Except 2 studies which used their own scoring system [2023], the rest defined CMR as the absence of abnormal FDG uptake noted on the pre-treatment 18F-FDG PET, and PMR was defined as any persistent abnormal uptake at these sites. PMD was defined as new foci of abnormal FDG uptake. One used quantitative assessment based on European Organization for Research and Treatment of Cancer (EORTC) criteria. Kunos et al. [19] stratified treatment response based on standardized uptake value (SUV) ratio or difference between pre- and post-RT (Table 2).

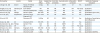
Table 1
Study and clinicopathological characteristics of studies included in meta-analysis

| Study characteristics | Clinicopathological characteristics | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First author | Year | Institution | Enrollment period | No. of patients | Study design | Median age (yr) | Stage | Pathology | Tx | Median interval (Tx–PET, mo) | Response (%) | Compare | Endpoint | Median f/u (mo) | |
| Chong et al. [17] | 2015 | Kyungpook National University Medical Center | 2005–2014 | 56 | R | 51.5* | IIB–IIIB | SqCC, AC | CCRT | 5.0 | CMR (66) | CMR | PMR/PMD | PFS | 42.0 |
| PMR (30) | |||||||||||||||
| PMD (4) | |||||||||||||||
| Grigsby et al.[14] | 2003 | Washington University School of Medicine | 1998–2001 | 76 | R | 50.0* | IA2–IVB | SqCC, AC, ASC, SCC | CCRT/RT | Range, 2.4–10.4 | CMR (82) | CMR | PMR/PMD | PFS | 21.3 |
| PMR/PMD (18) | |||||||||||||||
| Herrera et al. [18] | 2016 | Lausanne University Hospital | 2007–2014 | 38 | R | 52.5 | IB1–IVA | SqCC, AC | CCRT | 3.0 | CMR (76) | CMR | PMR | PFS, OS | 37.0 |
| PMR (24) | |||||||||||||||
| Kunos et al. [19] | 2011 | Case Comprehensive Cancer Center | 2004–2009 | 51 | R | 49.0 | IB2–IVA | SqCC, AC, ASC | CCRT | 2.6 | Post/Pre-Tx SUV ratio >0.33 (29) | >0.33 | <0.33 | PFS | 15.0 |
| <0.33 (71) | |||||||||||||||
| Liu et al. [20] | 2018 | Chang Gung Memorial Hospital | 2009–2013 | 55 | P | 56.0 | I-IIIA | SqCC | CCRT | Range, 2–3.0 | CMR (60) | CMR | PMR/PMD | OS | 81.0 |
| Equivocal (24) | |||||||||||||||
| PMR/PMD (16) | |||||||||||||||
| Oh et al. [21] | 2013 | Samsung Medical Center | 2009–2010 | 59 | P | 53.5 | IB1–IVA | SqCC, AC | CCRT | 1.0 | CMR (73) | CMR | PMR/PMD | PFS | 25.0 |
| PMR (20) | |||||||||||||||
| PMD (7) | |||||||||||||||
| Onal et al. [22] | 2014 | Baskent University Faculty of Medicine | 2006–2012 | 152 | R | CMR group: 58.0 | IB2–IVA | SqCC, AC | CCRT | 3.9 | CMR (80) | CMR | PMR/PMD | PFS, OS | 28.7 |
| PMR/PMD group: 57.0 | PMR (15) | ||||||||||||||
| PMD (5) | |||||||||||||||
| Scarsbrook et al. [23] | 2017 | Leeds Teaching Hospitals NHS Trust | 2011–2014 | 96 | R | 47.0* | IB1–IVA | SqCC, AC, ASC, NEC | CCRT | 3.3* | CMR (42) | CMR | PMR | PFS, OS | Range 18–54.0 |
| Indeterminate (25) | |||||||||||||||
| PMR (18) | |||||||||||||||
| PMD (15) | CMR | PMD | |||||||||||||
| Schwarz et al. [10] | 2007 | Washington University School of Medicine | 1998–2006 | 152 | R | 49.0 | IB1–IVA | SqCC, AC, ASC, CCC | CCRT | NR | CMR (75) | CMR | PMR | PFS, DSS | Range 28–70 |
| PMR (12.5) | |||||||||||||||
| PMD (12.5) | CMR | PMD | |||||||||||||
| Schwarz et al. [10] | 2007 | Washington University School of Medicine | 2003–2006 | 92 | P | 51.0 | IB1–IVA | SqCC, AC, ASC, CCC | CCRT | 3.1* | CMR (70) | CMR | PMR | PFS, DSS | 25* |
| PMR (16) | |||||||||||||||
| PMD (13) | CMR | PMD | |||||||||||||
| Siva et al. [24] | 2015 | Peter MacCallum Cancer Centre | 2002–2007 | 105 | P | 54.0 | IB–III | SqCC, AC, Others | CCRT | Range, 3–6.0 | CMR (70) | CMR | PMR | OS | 62.3 |
| PMR (9) | |||||||||||||||
| PMD (21) | CMR | PMD | |||||||||||||
| Yoon et al. [25] | 2016 | Yonsei University College of Medicine | 2005–2013 | 172 | R | 55.0 | IB1–IVA | SqCC, AC, ASC, SCC | CCRT/RT | 1.5 | CMR (11) | CMR/PMR | SMD/PMD | PFS, OS | NR |
| PMR (72) | |||||||||||||||
| SMD (12) | |||||||||||||||
| PMD (5) | |||||||||||||||
AC, adenocarcinoma; ASC, adenosquamous carcinoma; CCC, clear cell carcinoma; CCRT, concurrent chemoradiotherapy; CMR, complete metabolic response; DSS, disease-specific survival; f/u, follow-up; NR, not reported; OS, overall survival; P, prospective; PET, positron emission tomography; PFS, progression-free survival; PMD, progressive metabolic disease; PMR, partial metabolic response; R, retrospective; RT, radiotherapy; SCC, small cell carcinoma; SMD, stable metabolic disease; SqCC, squamous cell carcinoma; SUV, standardized uptake value; Tx, treatment.
*Data reported as mean values.
Table 2
Characteristics of PET
| First author | Vendor | Model | Dose (MBq) | Uptake time (min) | Scan time (min/bed) | Reconstruction | Attenuation correction | PET/CT | Methods of response evaluation |
|---|---|---|---|---|---|---|---|---|---|
| Chong et al. [17] | GE/CTI | Reveal RT-HiREZ/Discovery STE | 8.1/kg | 60 | 3 | OSEM | CT | Yes | Qualitative |
| Grigsby et al. [14] | Siemens/CTI | ECAT EXACT | NR | NR | NR | NR | NR | PET alone | Qualitative |
| Herrera et al. [18] | GE | Discovery 690FX/TOF | 3.5/kg | 60 | NR | NR | CT | Yes | Qualitative |
| Kunos et al. [19] | Phillips | Gemini TF/GXL | 370–444 | 60 | 1–3 | NR | CT | Yes | Quantitative (SUV ratio) |
| Liu et al. [20] | GE/Siemens | Discovery ST16/Biograph mCT | 370 ± 10% | 50 | NR | OSEM | CT | Yes | Qualitative |
| Oh et al. [21] | GE | Discovery STE | 5.0/kg | 60 | 2.5 | OSEM | CT | Yes | Qualitative, Quantitative (SUV difference) |
| Onal et al. [22] | GE | Discovery STE 8 | 370–555 | 60 | 3 | NR | CT | Yes | Qualitative |
| Scarsbrook et al. [23] | Phillips | Gemini TF 64 | 400 | 60 | NR | OSEM | CT | Yes | Qualitative |
| Schwarz et al. [10] | NR | NR | NR | NR | NR | NR | NR | PET alone | Qualitative |
| Schwarz et al. [10] | Siemens | Biograph LSO 2 | 555–740 | 45–60 | 2–4 | OSEM | CT | Yes | Qualitative |
| Siva et al. [24] | GE | Discovery LS/STE | 370 | NR | NR | NR | CT | Yes | Qualitative |
| Yoon et al. [25] | GE | Discovery LS/ST | 5.5/kg | 60 | 3 | OSEM | CT | Yes | Quantitative (EORTC) |
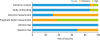
2. Quality assessment
Fig. 2 presents risk of bias assessment using the QUIPS tool. Two different study cohorts in Schwarz et al. [10] were separately assessed. For selection bias, 6 cohorts including the retrospective cohorts of Schwarz et al. [10] had a moderate risk, as the study populations were enrolled retrospectively and not consecutively [14171925]. All the included cohorts had a low-risk of attrition bias. Regarding prognostic factor measurement, 9 cohorts had a moderate risk of bias as it was not clearly mentioned whether image analyses were done in a blind manner [1417182021222324]. For outcome measurement, 10 cohorts had a moderate risk of bias, because it is unclear whether the outcome was measured without knowledge of prognostic factors or the methods for outcome measurement was not clearly reported [141718192122232425]. In regard to confounding bias, 2 cohorts had a high-risk as no or incomplete multivariate analysis was performed [2223]. Regarding statistical analysis, all the studies had a low-risk of bias.
3. OS
The prognostic value of 18F-FDG PET response for OS or disease-specific survival was assessed in 8 cohorts. Most cohorts (7/8) compared CMR to PMR and/or PMD. However, Yoon et al. [25] compared responders (CMR and PMR) to non-responders (SMD and PMD) so that the study was not included for quantitative synthesis. The study reported that maximum SUV responders demonstrated significantly low HRs in OS (HR=0.01; 95% CI=0.00–0.17; p=0.002) and PFS (HR=0.07; 95% CI=0.01–0.60; p=0.016) compared to non-responders in multivariate analysis. As a result, a total of 7 cohorts were included for OS quantitative synthesis, and 3 subgroup analyses were possible according to the pattern of comparison as follows: 1) CMR vs. PMR, 2) CMR vs. PMD, and 3) CMR vs. PMR/PMD (Fig. 3).
Fig. 3
Forest plots for HRs of OS comparing (A) CMR to PMR, (B) CMR to PMD, and (C) CMR to PMR/PMD.
CI, confidence interval; CMR, complete metabolic response; HR, hazard ratio; OS, overall survival; PMD, progressive metabolic disease; PMR, partial metabolic response; SE, standard error.

Pooled HR of CMR compared to PMR was 0.19 (95% CI=0.11–0.31) in 5 cohorts. Moderate heterogeneity was found (I2=50%). Pooled HR of CMR compared to PMD was more evident at 0.07 (95% CI=0.04–0.12) in 4 cohorts, and pooled HR of CMR compared to both PMR and PMD was 0.20 (95% CI=0.12–0.34) in 2 cohorts without significant heterogeneity (I2=0%).
4. PFS
The HRs of 18F-FDG PET response regarding PFS was evaluated in 9 cohorts. Since Kunos et al. [19] reported the outcome in a different way using the ratio of post-therapy to pre-therapy SUVs, it was excluded for quantitative synthesis. They presented that the post-therapy/pre-therapy SUV ratio <0.33 was associated with a 35% improvement in 6-month PFS (p=0.004).
With a total of 8 cohorts included in quantitative synthesis, 3 subgroup analyses were performed same as OS analyses (Fig. 4). The pooled HR of CMR was 0.17 (95% CI=0.10–0.29) compared to PMR in 4 cohorts, 0.02 (95% CI=0.01–0.06) compared to PMD in 3 cohorts and 0.12 (95% CI=0.07–0.19) compared to both PMR and PMD in 4 cohorts. No heterogeneity was present in all subgroup analyses (I2=0%).

DISCUSSION
The present study demonstrated that response evaluation using post-RT 18F-FDG PET could be a strong prognostic factor for both OS and PFS in uterine cervical cancer patients. Patients who resulted in CMR showed significantly lower risk of progression and death compared to populations with PMR or PMD. The HR of CMR compared to PMR was 0.19, and it was more prominent compared to PMD with HR of 0.07 in OS analyses. Although HR comparing CMR to both PMR and PMD (0.20) was higher than that of CMR compared to PMR, we speculated that the small number of included studies was susceptible for bias of sampling error.
About one-third of cervical cancer patients experience recurrence mostly within the first 2 years after RT [26], and majority of them might have been presented with PMD or PMR, if they had undergone post-treatment 18F-FDG PET evaluation. Early intervention could be considered for patients who expect poor prognosis, with PMR or PMD detected using post-RT 18F-FDG PET to improve their survival. Several previous studies failed to show the benefit of surgery following CCRT compared to definitive CCRT [27]. However, a considerable proportion of patients presented with pathological complete response (range, 38%–86%), and these patients may have concealed the benefit of surgery for cases of residual tumor. Response evaluation using post-RT 18F-FDG PET could be valuable in identifying appropriate candidates for surgery after CCRT. Furthermore, the decision of a surgical salvage heavily depends on the location and extent of failure. The extent of hysterectomy also affects survival, as Sun et al. [28] reported significantly better OS among patients who received extrafascial hysterectomy than those who treated with extended hysterectomy after CCRT for advanced cervical cancer (5-year OS, 53.5% vs. 40.7%; p<0.05). This made the role of post-RT imaging more crucial.
The traditional response evaluation tool was Response Evaluation Criteria in Solid Tumors (RECIST) criteria using the diameter of the tumor [25]. However, size measurement is often difficult in the tumors with obscure margins, cystic lesions, and scar tissue. Sometimes, tumors do not shrink but are stabilized with necrotic and cystic changes without viability. Although CT or MRI has been more commonly used for post-treatment imaging than 18F-FDG PET in the clinical setting, CT or MRI using RECIST criteria inevitably could not reflect these phenomena. On the other hand, 18F-FDG PET allowed measurement of tumor response even in the absence of anatomical changes, by evaluating metabolic activity of the residual tumor [8]. Yoon et al. [25] reported that 18F-FDG PET parameters were better prognostic markers compared to RECIST criteria, although CT which has lower diagnostic value than MRI was used. Their findings also suggested that the tumor diameter itself may not decrease due to fibrotic changes, inflammation or necrosis, and the more important factor seemed to be glucose metabolism. Post-treatment 18F-FDG PET is generally not advocated due to lack of definite evidence [2]. However, National Comprehensive Cancer Network (NCCN) guidelines recommends 18F-FDG PET/CT as a preferred follow-up modality owing to its detection ability for both locoregional and distant recurrences [29].
Few studies reported the accuracy of 18F-FDG PET in detecting residual tumor compared to pathologic results. There was a single prospective trial comparing the diagnostic performances of MRI and 18F-FDG PET/CT in predicting pathologically assessed residual disease after neoadjuvant CCRT [30]. Although there was no difference in overall accuracy (MRI, 84.6% vs. PET/CT, 85.0%; p=0.900), sensitivity was higher for MRI (62.8%) than for PET/CT (47.1%, p<0.001), while specificity was higher for PET/CT (96.5%) than for MRI (91.2%, p<0.001). To improve the accuracy of post-RT response evaluation, combination of MRI and 18F-FDG PET has emerged with promising predictive power through combining advanced anatomical information and tumor metabolic information. A pilot study demonstrated an increase in diagnostic confidence in 80%–90% of the patients who received CCRT. Also, change of opinion was observed in 70% and change of policy in 50%, especially in the group with residual tumor [31]. Although there is still a lack of strong evidence regarding the benefit of assessing treatment response, PET/MRI demonstrated an improved diagnostic performance during initial staging workup with accuracy of 83.3% for cervical tumor staging, which was better than that of PET/CT (53.3%, p=0.008) [32], and detection of lymph node metastasis [33].
Although the timing of imaging can considerably affect the results of response evaluation, optimal timing of post-treatment imaging is still undefined. Despite using 18F-FDG PET is still difficult to discriminate treatment-related changes from residual tumors. Therefore 18F-FDG PET was examined 3 months after the completion of CCRT [34]. Most studies included in the present analysis also reported their median interval between the completion of RT and 18F-FDG PET around 3 months. However, the overall timing was varied, ranging from 1.0 to 10.4 months. CMR rate at 3 months post-RT was ~70% (Table 1). Oh et al. [21] which obtained 18F-FDG PET at l month as per protocol, reported similar response outcomes with CMR of 73% similar to the results of PET at 3 months, while Yoon et al. [25] with a median interval of 1.5 month reported CMR of only 11%. Due to the conflicting response results and concern of treatment-related metabolic response, recommended timing of post-treatment 18F-FDG PET appeared to be 3 months. However, with the advent of combined imaging modalities such as PET/MRI, further studies analyzing the effectiveness of shortened interval between end of treatment and imaging are needed.
Absence of objective response criteria is another issue. All studies included in quantitative synthesis in the present report qualitatively assessed the metabolic response (Table 2). Except 2 studies, the rest of 7 studies utilized same definition for response assessment. However, qualitative evaluation had fundamental limitation of inter-observer variation. To resolve the challenge on lack of uniformity, quantitative approaches such as EORTC or PET response criteria in solid tumors (PERCIST) criteria has been widely adopted [35]. The pooled HRs in the present study might not be directly applied to the quantitative response evaluation tools. Yoon et al. [25] was the only study which utilized EORTC criteria, and there was no study using PERCIST rule. However, considering the fair agreement of visual versus quantitative assessment [36], introduction of EORTC or PERCIST criteria to post-RT 18F-FDG PET in uterine cervical cancer may be of significant clinical value, and could provide reproducible response outcomes and improved prognostic power.
There were several limitations in this meta-analysis. First of all, majority of the studies included were retrospective trials so that there might be a tendency toward overestimation of pooled HRs. Secondly, the number of studies for quantitative synthesis was small. In addition, due to the different patterns of reporting, the studies were divided into 3 subgroups with small number of study cohorts included. Furthermore, 1 subgroup analysis comparing CMR and PMR/PMD included only 2 cohorts [2022], and one of them weighed more than 90% [22]. As described previously, this could be vulnerable to sampling error. Thirdly, study and clinicopathological characteristics were varied in most studies (Table 1) and it might be a bias for survival. Meta-regression analysis could evaluate the impact of these factors. However, it was impossible in the present study due to the paucity of the number of studies in each subgroup. Despite the disadvantages, the present study is the first systematic review and meta-analysis of the role of 18F-FDG PET evaluation in patients with uterine cervical cancer who received RT.
In conclusion, patients with cervical cancer which resulted in CMR during post-RT 18F-FDG PET were at considerably lower risk of death or progression. As 18F-FDG PET has the advantage of detecting metabolic activity of the tumor, 18F-FDG PET could be a reasonable follow-up modality after RT for cervical cancer. Future studies to find the most optimal modality, timing, and assessment criteria for evaluating post-treatment response and prognosis are warranted.
 XML Download
XML Download