

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a multifactorial and highly heterogeneous disease which is clinically characterized by the appearance of nasal polyps (NP) in the nasal cavity. CRSwNP causes typical symptoms such as nasal obstruction, nasal discharge, and/or loss of smell.1 Functional endoscopic sinus surgery (FESS) is an effective intervention for patients with medically recalcitrant CRSwNP. However, despite repeated FESS combined with aggressive medical therapy, some patients tend to be poorly controlled and have a high recurrence rate of NP.234 Generally, a subset of CRSwNP patients will fail to respond to conventional FESS followed by oral or topical corticosteroids and antibiotics, and these patients are categorized as refractory CRSwNP. A large database analysis of the US population showed that the overall revision rate in chronic rhinosinusitis (CRS) patients was 6.65% (4,078/61,339) and that NP was a major risk factor for revision surgery.5 Furthermore, a recent cohort study of patients with CRSwNP reported 40% NP recurrence rate after FESS despite appropriate medical therapy.6
It is well known that refractory CRSwNP is associated with cystic fibrosis and aspirin-exacerbated respiratory disease.78 [REMOVED HYPERLINK FIELD]In addition, eosinophilic CRSwNP is traditionally known to have a higher recurrence rate than non-eosinophilic CRSwNP.9 However, some studies have showed there is neither involvement nor contribution of different types of mucosal remodeling features, inflammatory patterns, or atopic conditions on the pathogenesis of refractory CRSwNP.1011 A retrospective study of CRSwNP patients who underwent revision surgery over a 25-year period by a single surgeon reported that there is no association between sex, prior surgery, asthma, computed tomographic stage, allergic mucin or eosinophilia on time to revision surgery.12 Previous studies demonstrated that surgical samples obtained from surgery exhibit different histological and cytokine pattern compared to primary surgical samples.813 However, with the advent of biologicals, specific endotypes of refractory CRS requiring revision surgeries remain undetermined. Furthermore, it is important to consider the impact of different subtypes such as eosinophilic versus non-eosinophilic disease. Therefore, in this study, we analyzed cytokines levels in cases of refractory CRSwNP and identified several key inflammatory markers associated with specific subtypes.
MATERIALS AND METHODS
Patients and tissue samples
In this cross-sectional study, sinonasal tissues were collected from CRSwNP patients and control subjects from February 2014 to April 2017 by 4 well-trained experienced surgeons at the Samsung Medical Center, Seoul, Republic of Korea. The diagnosis of CRS was established based on the 2012 European position paper on rhinosinusitis and NP guidelines.1 Patients who underwent FESS once were defined as having primary NP (pNP). Seventy subjects who underwent primary FESS were selected based on the absence of recurrent polyps at subsequent outpatient visits with a follow-up time of over 24 months. Patients who were uncontrolled with medications, including antibiotics and corticosteroids, and then underwent FESS two or more times, were defined as having refractory NP (rNP). Usually, patients were prescribed oral corticosteroids (prednisolone, 10–30 mg per day) for 1–2 weeks or oral antibiotics more than two weeks based on a bacterial culture result. Some of the asthmatic patients should be pre-medicated with several days' systemic corticosteroids to prevent anesthesia or surgery-induced pulmonary complications according to the local Institutional Review Board (IRB) guidelines and hospital policy. Sinonasal NP tissues from rNP patients who had bilateral diffuse polyposis were collected in the middle meatus at the time of revision surgery. Patients who underwent skull base surgery or endoscopic dacryocystorhinostomy with no signs or symptoms of nasal inflammation were included as control subjects. Patients were excluded if they were at less than 18 years of age or had unilateral disease, primary ciliary dyskinesia, cystic fibrosis, or eosinophilic granulomatosis with polyangiitis. Atopic status was evaluated by screening for serum specific immunoglobulin (Ig) E antibodies to common aeroallergens using ImmunoCAP® assays (Phadia AB, Uppsala, Sweden) according to the manufacture's recommendations. A diagnosis of asthma was made by an allergist based on spirometry (change in FEV1 of 12% or more following administration of a short-acting β-agonist) or methacholine challenge test. Endoscopic examination was used to obtain the Lund-Kennedy score and computed tomography (CT) images were staged with the Lund-Mackay score.1415 Bacterial cultures were taken when mucopurulence was observed during endoscopy. Demographic details of subject's characteristics are shown in Table. CRSwNP was classified as either eosinophilic NP (ENP) or non-ENP (NENP), where tissue eosinophilia was defined as an eosinophilic count exceeding 10% of the total inflammatory cells per high power field in NP tissue.16 The IRB of Samsung Medical Center approved this study (IRB No. SMC 2017-02-129) and informed consent was obtained. Biospecimens for this study were provided by the Samsung Medical Center Biobank.
Table
Demographics of subjects evaluated in protein analysis
Data are expressed as median (interquartile range) or number (%).
pNP, primary nasal polyps; rNP, refractory nasal polyps; IgE, immunoglobulin E; ECP, eosinophil cationic protein; ENP, eosinophilic nasal polyps; NENP, non-eosinophilic nasal polyps; NA, not applicable.
*P value < 0.05 was considered statistically significant for all analyses; †Statistically significant between primary and revision ENP; ‡Statistically significant between primary and revision NENP.
Measurement of cytokines in tissue homogenates
NP tissues from CRSwNP and UP tissues from control subjects were obtained. Tissues were homogenized and supernatants were stored at −80ºC until analyzed as previously described.171819 Protein concentrations for tissue extracts were determined using a Pierce 660-nm Protein Assay Kit (Thermo Scientific Inc., Rochester, NY, USA). Samples were thawed at room temperature and vortexed to ensure complete mixing. Multiplex cytokine analysis kits (B-cell activating factor [BAFF], C-C motif chemokine ligand [CCL]-11, CCL-24, interleukin (IL)-5, IL-8, IL-13, IL-17A, IL-23, interferon [IFN]-γ, myeloperoxidase [MPO], matrix metalloproteinase [MMP]-1, MMP-2, MMP-3, MMP-7, MMP-9, tissue inhibitor of metalloproteinase [TIMP]-1 and transforming growth factor [TGF]-β1) were obtained from R&D systems (cat. No. LMSAHM) and data were collected using a Luminex 100 (Luminex, Austin, TX, USA). Data analysis was performed using MasterPlex QT V.2.0 (MiraiBio, Alameda, CA, USA). All assays were run in duplicate according to the manufacturers' protocol. The sensitivity of each cytokine was as follows: BAFF (1.01 pg/mL), CCL-11 (14.6 pg/mL), CCL-24 (1.34 pg/mL), IL-5 (0.5 pg/mL), IL-8 (1.8 pg/mL), IL-13 (32.4 pg/mL), IL-17A (1.8 pg/mL), IL-23 (11.4 pg/mL), IFN-γ (0.4 pg/mL), MPO (20.4 pg/mL), MMP-1 (2.7 pg/mL), MMP-2 (108 pg/mL), MMP-3 (5.3 pg/mL), MMP-7 (23.2 pg/mL), MMP-9 (13.6 pg/mL), TIMP-1 (3.42 pg/mL) and TGF-β1 (2.1-24.6 pg/mL). Mucosal tissue eosinophil cationic protein (ECP) were measured by ImmunoCAP® and the sensitivities for ECP were 2 μg/L. Anti-dsDNA quantitative IgG and IgA enzyme immunoassays (EIAs; Alpco Diagnostics, Salem, NH, USA) were also assessed. The detection range for all EIAs was 30 to 150,000 IU/mL. Protein levels in tissue homogenates were normalized to the concentration of total protein (mg/mL).
Immunohistochemical staining (IHC)
IHC was performed with the Polink-2 plus polymerized horseradish peroxidase (HRP) broad DAB Detection System (Golden Bridge International Labs, Bothell, WA, USA) as previously described.20 Briefly, after deparaffinization sections were incubated in 3% hydrogen peroxide to inhibit endogenous peroxidase activity. Heat-induced epitope retrieval was performed by microwaving samples in 10 mmol/L citrate buffer (pH 6.0). Sections were then incubated for 60 min at room temperature with primary antibody consisting of mouse anti-human neutrophil elastase (HNE; 1:500; R&D Systems, Minneapolis, MN, USA). The sections were then incubated in a broad antibody enhancer, followed by polymer-HRP and stained using the DAB Detection System reagent. Finally, slides were counterstained with hematoxylin.
Statistical analysis
Data were tested for normality of distribution using the Shapiro-Wilk test and are reported as median with interquartile range due to a nonparametric distribution. Data were analyzed by the Kruskal-Wallis test with the Dunn multiple comparison test. Tests for statistical differences for binary classification were analyzed using Fisher's exact test. Correlations were tested using Spearman's rank correlation coefficients. A P value of less than 0.05 was considered statistically significant. Principal component analysis (PCA) was used to describe patterns of inflammatory mediators. Analyses were performed using Stata software v14.0 (StataCorp, College Station, TX, USA) and Graphpad prism software 6.0 (GraphPad software Inc, La Jolla, CA, USA).
RESULTS
Clinical characteristics of refractory CRSwNP
Refractory CRSwNP patients underwent revision surgery despite primary FESS and postoperative medical treatments have more extensive disease, worse postoperative courses and were younger compared to patients with primary CRSwNP (Table). In addition, preoperative endoscopic and CT scores were higher in rNP than in pNP. Compared to pNP subjects, rNP subjects showed higher infection rate (mucopurulence and culture-positive rate) and more frequent use of antibiotics and suffered from symptomatic bacterial infection.
Immunological profiles of refractory CRSwNP
To characterize the inflammatory profiles of refractory CRSwNP patients, multiplex bead-based immunoassay for inflammatory cytokines was performed in 70 pNP, 86 rNP and 23 control subjects (Fig. 1). Th2 inflammatory markers, such as IL-5, ECP, CCL-11, CCL-24 and IL-13, were up-regulated in pNP and rNP, but not significantly different between pNP and rNP subjects. Interestingly, levels of Th1 cytokine (IFN-γ), BAFF and Th17-associated mediators, such as MPO, IL-8, IL-17A and IL-23, were increased in rNP compared to pNP. With respect to remodeling markers, both pNP and rNP exhibited lower levels of TGF-β1 compared to controls and levels of TGF-β1 were lower in rNP than in pNP. MMP2/TIMP1 and MMP9/TIMP1 ratios were all up-regulated in rNP compared to controls and pNP.
Fig. 1
Inflammatory mediators in rNP. (A) Eosinophils-associated inflammatory markers, (B) Neutrophils-associated inflammatory markers and (C) Remodeling markers. Data were evaluated by Kruskal-Wallis test and Dunn multiple comparison test. A P value < 0.05 was considered statistically significant.
ECP, eosinophil cationic protein; CCL, C-C motif chemokine ligand; IL, interleukin; IFN, interferon; MPO, myeloperoxidase; TGF, transforming growth factor; MMP, matrix metalloproteinase; TIMP, tissue inhibitor of metalloproteinase; BAFF, B-cell activating factor; pNP, primary nasal polyps; rNP, refractory nasal polyps.

We next asked whether levels of inflammatory mediators could make a discrimination between rNP and pNP in each subtype. To do so, a multivariate analysis of multiplex data was performed by exploratory factor analysis using PCA of the correlation matrices of major mediator levels measured (ECP, BAFF, CCL-24, IL-5, IL-8, IL-13, IL-17A and IFN-γ). PCA retained 2 components explaining 47.1% of all variance in the data (Fig. 2). The first component (component 1) accounted for 26.3% of the variance and consisted of IFN-γ, BAFF and IL-17A in decreasing order. The second component (component 2) accounted for 20.8% of the variance and was composed of CCL-24, ECP and IL-5. Component 1 was predominantly represented by BAFF and Th17/Th1related markers, whereas component 2 was consistent with a Th2 profile (Supplementary Tables S1 and S2). When factor scores were analyzed using the Mann-Whitney test, components 1 and 2 were significantly different among groups (data not shown). We also found that component 1 was able to discriminate between pNP and rNP in both eosinophilic and non-eosinophilic subtypes. These findings demonstrated that BAFF- and Th17/Th1-related markers are the main biomarkers for characterizing rNP regardless of tissue eosinophilia. Interestingly, neutrophilic infiltration in refractory ENP (rENP) and refractory NENP was also enhanced based on IHC using anti-HNE compared to pNP (Fig.3). Eosinophilic infiltration was increased in pNP and rNP compared to control tissues, whereas no difference was observed between pNP and rNP (Fig. 3).
Fig. 2
Principal component analysis in rNP. Component 1 (Th1/Th17 and BAFF) can help to discriminate between pNP and rNP in both eosinophilic and non-eosinophilic subtypes.
ECP, eosinophil cationic protein; CCL, C-C motif chemokine ligand; IL, interleukin; IFN, interferon; BAFF, B-cell activating factor; rNP, refractory nasal polyps; p, primary; r, refractory; NP, nasal polyps; ENP, eosinophilic nasal polyps; NENP, non-eosinophilic nasal polyps.
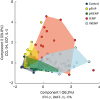
Fig. 3
Neutrophilic infiltration in rNP. (A) Enhanced neutrophilic infiltration in rNP, refractory ENP, refractory non-ENP. (B) Immunohistochemical staining using anti-HNE. (C) Increased eosinophilic infiltration in primary and rNP compared to control tissues.
rNP, refractory nasal polyps; p, primary; r, refractory; ENP, eosinophilic nasal polyps; NENP, non-eosinophilic nasal polyps; HNE, human neutrophil elastase; HPF, high power field.

Immunological profiles of refractory CRSwNP according to asthma comorbidities
To investigate the differences in the inflammatory profiles of NP in asthmatic rNP versus non-asthmatic rNP, we used a multiplex bead-based immunoassay for inflammatory cytokines in 20 asthmatic rNP and 66 non-asthmatic rNP (Fig.4). MPO, IFN-γ, IL-17A and BAFF were increased, therefore, appear to be common signature mediators in both non-asthmatic and asthmatic rNP cases. Moreover, ECP and CCL-24 were up-regulated in asthmatic rNP compared to pNP and controls. Eosinophilic inflammation may affect the refractoriness of the disease in asthmatic rNP patients.
Fig. 4
Inflammatory mediators in rNP with asthma vs. without asthma. Data were evaluated by Kruskal-Wallis test and Dunn multiple comparison test. A P value < 0.05 was considered statistically significant.
ECP, eosinophil cationic protein; CCL, C-C motif chemokine ligand; IL, interleukin; MPO, myeloperoxidase; IFN, interferon; BAFF, B-cell activating factor; TGF, transforming growth factor; pNP, primary nasal polyps; rNP, refractory nasal polyps; A: asthmatic, NA: non-asthmatic.

Autoantibodies in refractory CRSwNP
High levels of BAFF are associated with autoimmune diseases; additionally, NP tissues from patients with revision surgery showed higher levels anti-dsDNA IgG antibody compared to primary surgery tissues.21 Therefore, we measured levels of anti-dsDNA IgG and IgA antibodies levels in pNP and rNP (Fig. 5). The rNP demonstrated a higher level of anti-dsDNA IgG and IgA compared to controls. In subgroup analysis, asthmatic rENP showed higher levels of anti-dsDNA IgG and IgA antibodies compared to the other groups (Fig. 5).
Fig. 5
Autoantibodies production in rNP. (A) Anti-dsDNA IgG and IgA in primary and rNP. (B) Anti-dsDNA IgG and IgA according to asthma comorbidity. (C) Anti-dsDNA IgG and IgA according to each phenotype of rNP.
Ig, immunoglobulin; pNP, primary nasal polyps; rNP, refractory nasal polyps; A, asthmatic; NA, non-asthmatic; ENP, eosinophilic nasal polyps; NENP, non-eosinophilic nasal polyps.

DISCUSSION
To date, several studies have reported that multiple stimuli, such as bacterial substances, induce neutrophil infiltration and enhance Th17 inflammation, and that cross-talk between neutrophils and Th17 cytokines may be associated with more severe forms of inflammatory disease such as rheumatoid arthritis, systemic lupus erythematosus, and Sjogren's syndrome.22232425 In the present study, we found that neutrophil-related mediators (MPO and IL-8)and Th17-associated cytokines (IL-17A and IL-23) were up-regulated in patients with refractory CRSwNP. Consistent with our results, one prior study showed that neutrophil-related infiltration and Th17-associated cytokines were associated with steroid resistance and disease severity in airway inflammatory diseases.26 Additionally, other previous study revealed that Th17 cell and its associated cytokines (IL-17A and IL-17F) prompt steroid resistance by up-regulating glucocorticoid receptor-beta in asthma.27 Th2/Th17-predominant asthma subgroups manifested the most severe form of disease compared to Th2-high subgroups, because Th2/Th17 cells were resistant to dexamethasone-induced cell death. Moreover, the number of Th2/Th17 cell and IL-17 concentration correlated with clinical parameters such as PC20 for methacholine, eosinophil counts and FEV1.28 Therefore, the mechanism by which Th17 or neutrophilic inflammation is induced has been a challenging topic with respect to managing uncontrolled airway inflammation.
In this study, refractory CRSwNP was defined in patients who required revision sinus surgery due to poor response to medical treatments including corticosteroids and antibiotics after primary FESS, and they represented more severe neutrophilic inflammation (IFN-γ, BAFF, MPO and IL-8) and higher levels of Th17-associated cytokines (IL-17A and IL-23), which may include steroid-resistant endotype in CRSwNP similar to severe asthma. This result was not consistent with that of a previous study which analyzed tissue homogenates at the first surgery in recurrent and nonrecurrent CRSwNPs and demonstrated that the expression level of IFN-γ at the first surgery of nonrecurrent CRSwNPs were higher than those from recurrent patients.8 These results imply that higher level of IFN-γ at the first surgery is associated with a lower risk of recurrence. Unfortunately, it is difficult to investigate risk factors for recurrence based on our data, since the design of our study was not a longitudinal study. However, up-regulation in levels of IFN-γ in revision surgeries of this study was prominent compared to primary cases. These observations may be explained, in part, by clinical settings, such as uncontrolled infections, which induce the Th1/Th17 axis. Additionally, there may be a regional difference, since the majority of Korean NPs account for NPs of non-eosinophilic type in which the Th1/Th17 axis play a main role.
Interestingly, there is increasing evidence that recurrent infections or biofilms-forming bacteria contribute to refractory CRS.293031 According to one study with a large sample size adopted multiple logistic regression analysis to identify independent risk factors for revision ESS, biofilms and positive bacteria cultures were independent risk factors for revision surgery as well as asthma.31 Another clinical study also demonstrated a total bacterial culture rate of 83% in revision cases.30 In uncontrolled bacterial infection, Th17 cytokines, such as IL-17A and IL-23, may be enhanced and play a role in immune defenses against extracellular bacteria by recruiting neutrophils. In addition, bacterial substances can induce BAFF in various immune cells.323334 Furthermore, lipopolysaccharide-induced IL-8 production was enhanced by BAFF stimulation in a human macrophage-like cell line, THP-1.35 Bacterial infection induces BAFF expression and may trigger class-switching, production of Ig and activation of effector T cells. Consistently, this phenomenon has been observed in viral infections and mycobacterial infection as well.363738 Specifically, Pseudomonas aeruginosa infection in patients with cystic fibrosis induced high levels of BAFF in bronchoalveolar lavage fluid, and BAFF expression was increased in lung homogenates of mice infected with P. aeruginosa.36 Therefore, we speculate that recurrent infections, which may be a significant feature in refractory CRSwNP requiring revision surgery, are able to induce up-regulation of Th17-related inflammation and BAFF.
BAFF is a potent stimulator of B-cell proliferation and class switching and is a surrogate marker for autoimmunity.24 Previous studies have provided evidence for local autoimmunity phenomenon by showing that BAFF is up-regulated in NP.39 Autoantibodies, such as anti-dsDNA IgG and IgA antibodies, were also locally increased in NP, especially in patients who had undergone revision surgery.21 In the present study, autoantibodies (anti-dsDNA IgG and IgA) were present at higher levels in rNP compared to controls. Particularly, asthmatic rENP exhibited the highest levels of anti-dsDNA IgG and IgA among NP subtypes. Given that ECP and CCL-24 were up-regulated in asthmatic rNP (Fig. 4), refractoriness of asthmatic NP may be attributed to eosinophilic inflammation and autoantibodies as well as neutrophilic inflammation.
In our study, refractory CRSwNP was defined as disease non-responsive to maximal medical treatment after primary surgery. Additionally, some of asthmatic patients should be pre-medicated with several days' systemic corticosteroids to prevent anesthesia- or surgery-induced pulmonary complications according to the local IRB guidelines and hospital policy. For these reasons, this study has the unavoidable limitations of human studies. These preoperative medications may underestimate the expression of Th2 cytokines. Despite these limitations of study design, Th1 and Th17 were up-regulated in all phenotypes of refractory CRS and asthmatic rNP showed higher levels of eosinophilic markers and autoantibodies. These findings suggest that inhibition of these pathways may provide a new treatment strategy for CRSwNP, particularly in rNP.
 XML Download
XML Download