

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Allergic rhinitis (AR) is an allergic disease that commonly co-occurs with asthma and, shows clinical symptoms due to the inflammatory mediators induced after exposure to aeroallergens.1 The prevalence of self-reported AR is between 2% and 25% of children worldwide2 and the prevalence of AR symptoms was reported at upto 35% in Korean elementary school children.3 It has increased dramatically in developed countries in the recent decades. Consequently, the burden of health costs and decreased quality of life from AR is a global health concern.34
House dust mites (HDMs), pets, cockroaches, and molds are common causes of perennial AR. Dermatophagoides pteronyssinus (Der p) and Dermatophagoides farina (Der f) were found to be independent risk factors for allergic sensitization with AR in a recent study on preschool children.5 HDMs are the most common triggers of AR.678 The avoidance of allergens is a fundamental treatment principle. Therefore, the avoidance of HDMs could be an effective strategy to prevent and manage AR. There are several recommended methods for reducing exposure to HDMs, such as maintaining room humidity below 50%, encasing mattresses and pillows with impermeable covers, washing the bedding regularly with hot water, removing carpets and furry toys, and vacuuming carpets and beds regularly. However, studies of the effectiveness of these measures have not been conclusive as most studies have found that the methods of avoidance were inconsistent or used in heterogeneous subjects.91011
It is important to reduce the concentration of HDMs in beds and blankets because they are major reservoirs of HDMs, and children spend most of their time in the bedroom and sleep more than 8 hours a day. Isolated use of impermeable mattress covers is not effective in controlling HDM allergens.12 Regular vacuum cleaning with a high-efficiency particulate air (HEPA) filter has been recommended to reduce the number of HDMs13; however, the effect on clinical symptoms is controversial.14
The present study aimed to investigate the effects of vacuuming mattresses on daily clinical symptoms of AR in HDMs-sensitized children and the level of HDMs allergens in dust. We hypothesized that daily vacuuming of mattresses would decrease symptoms of AR in the children and decrease the level of HDM allergens in dust.
MATERIALS AND METHODS
Patients and study setting
This study was performed between April and June of 2014. Forty children (6 to 12 years of age) with mild AR and sensitized only to HDM were recruited from the Department of Pediatrics of Hallym University Kangnam Sacred Heart Hospital, a secondary hospital located in Seoul, the Republic of Korea. This study was designed as a single-blind, randomized parallel trial with a 1-week washout period prior to intervention.
Inclusion/exclusion criteria
Children were recruited if they met the following inclusion criteria: aged between 6 and 12 years, mild persistent AR (symptoms ≥ 4 days per week), and sensitization to HDM but not to pollen, mold, animal dander, or other allergens. The diagnosis and classification of AR were determined according to the Allergic Rhinitis and its Impact on Asthma (ARIA) guideline.14 Sensitization was evaluated by skin prick test and serum specific immunoglobulin E (IgE; ImmunoCAP, ThermoFisher, Uppsala, Sweden) for common allergens in South Korea (Der p, Der f, birch, alder, oak, elm, mugwort, ragweed, hop Japanese, Bermuda grass, timothy grass, cat and dog epithelium, cockroach, Alternaria spp., and Aspergillus spp.). Children were excluded from the study if they 1) were sensitized to at least one of the common inhaled allergens other than HDM; 2) had respiratory infections within 4 weeks prior to the date of enrollment; 3) had undergone treatment related to respiratory allergic symptoms within 2 weeks prior to the date of enrollment; and 4) had no symptoms of AR at the time of recruitment.
Sample size calculation
Thus far, there have been only a few studies of the effects of vacuuming mattresses daily. Wu et al.13 published changes in HDM concentrations before and after daily mattress vacuuming for 8 weeks. In that study, the total dust weight was reduced by 77.7% (95% confidence interval, 70.8–84.7). We used this result to calculate our sample size. We found that to detect a 77.7% reduction in total dust weight at a 5% significance level with 80% power, only 1 child was required for each group.15
Due to concern about the accuracy of the sample size calculation, we did not use the calculation result and decided on a sample size of 40 children, considering the number of new patients visiting the clinic in 1 season because the changes in AR symptoms are affected by the weather change.
Randomization
Research randomizer16 was used to randomly allocate children to either the experimental group (n = 20) or the control group (n = 20).
Intervention
After a 1-week run-in period, the caregivers of the children in the experimental group cleaned the children's rooms the way they usually did and vacuumed their bedding with a hand-held vacuum cleaner with a micro HEPA filter used for bedding only (RS-300, H13 class HEPA filter, 350W, Raycop Korea, Seoul, Korea) provided for the study daily for 2 weeks. Vacuuming was carried out for 15 minutes every day. The caregivers of the children in the control group cleaned the children's rooms the way they did without vacuuming the bedding. The caregivers cleaned the room when the children were not at home so that they did not know which group they belonged to. All families in both groups received hand-held vacuum cleaners. The children were not allowed to take anti-allergic medication during the study. A research nurse who did not have any information about the subjects made 3 calls at intervals of 1 week from the beginning day and asked about the severity of total symptoms, sneezing, rhinorrhea, nasal congestion, and itching using a visual analogue scale. All information related to the symptoms was obtained directly from the children. Another research nurse visited each participant's home twice at the beginning and at 2 weeks. During both visits the nurse obtained a vacuumed dust sample from the mattress; at the first visit, the nurse also provided all the caregivers of the children with the same education on general environmental control (Fig. 1).

Drop-out criteria
The drop-out criteria included the caregivers skipping the room cleaning more than once, respiratory infections, withdrawal of consent, and any medication use for allergic symptoms during the study period.
Outcome measurement
The efficacy of vacuuming mattresses daily was determined by evaluating changes in AR symptoms (total symptoms, sneezing, runny nose, nasal congestion, and itching) over a 2-week period using a visual analog scale as the primary outcome. As secondary outcomes, we compared dust weight and the concentration of Der p1 and Der f1 in house dust in weeks 0 and 2.
Dust collection and enzyme-linked immunosorbent assay (ELISA)
Dust was collected from bed mattress or Korean-style mattress used as a bed on the floor and collected for 2 minutes using a upright vacuum cleaner (VC331LLMA6S, 1,200 W, Samsung, Seoul, Korea) equipped with a filter of 10 μm pore size on a 1 × 1 m2 area.17 All the collected dust was weighed and stored in a −80°C freezer to measure the major allergens (Der p1, Der f1) of HDMs. Dust samples of 100 mg each were mixed with 2 mL of 0.05% Tween 20 in phosphate buffered saline solution and shaken for 2 hours. Each sample was centrifuged at 2,500 rpm for 20 minutes, and then the supernatant was transferred into a new tube and analyzed by ELISA. ELISA analysis was performed according to the protocol presented using a 2-site ELISA (Indoor Biotechnologies, Cardiff, UK).
Statistical analysis
The characteristics between the 2 groups were compared using independent-sample Student's t-test for normally distributed data, or the Mann-Whitney U test for non-normally distributed data. Nominal variables were compared using the χ2 test. Changes in AR symptoms were compared using the Friedman test. Comparisons of continuous variables within groups were performed using Wilcoxon's matched-pairs signed-ranks test. A P value of < 0.05 was considered statistically significant. All analyses were performed using SPSS version 23.0 (SPSS Inc., Chicago, IL, USA).
Ethical consideration
The study protocol was approved by the Research Ethics Committee of Hallym University Kangnam Sacred Heart Hospital prior to initiation of the study (approval No. 2013-12-102). Written informed consent was obtained from each patient and his or her parents at the time of recruitment and before the study-related interview was performed.
RESULTS
A total of 40 children were randomized, evenly assigned to 2 groups and completed the study. The mean age of the enrolled patients was 8.7 ± 2.2 years (minimum-maximum age, 6.0-12.2 years). Baseline characteristics, including age, sex, family history of allergy, exposure to secondary smoking, pet owned, bed use, total eosinophil counts, accompanying atopic dermatitis, and specific IgE to Der p1 and Der f1 were not significantly different between the 2 groups (Table 1).
Table 1
Demographics and baseline characteristics of the study population in week 0
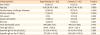
Values are presented as the mean ± standard deviation, the median (interquartile ranges), or numbers (%). Total IgE was analyzed using the t-test, other numeric data were analyzed using the Mann-Whitney U test, and the frequency was analyzed using χ2 test.
IgE, immunoglobulin E.
![]()
AR symptoms
AR symptoms were measured using a visual analog scale ranging from 0 to 10. The symptom scores of total symptoms (experimental vs. control groups, 5.5 [5.0-7.0] vs. 4.5 [2.0-6.0]; P = 0.038) and rhinorrhea (6.0 [2.25-7.0] vs. 2.5 [0.25–5.75], P = 0.043) were significantly higher in the experimental group in week 0. Other symptoms such as sneezing (4.5 [2.0-6.75] vs. 4.0 [1.25-5.0], P = 0.478), nasal obstruction (6.0 [5.25-8.0] vs. 4.5 [2.25-7.0], P = 0.056), and itching (6.0 [4.25-7.0] vs. 3.5 [1.25-7.0], P = 0.134) were similar between the 2 groups in week 0. In the experimental group, all symptom scores decreased significantly after 2 weeks, but there was no significant change in the control group. At week 2, all symptoms such as total symptoms (2.0 [1.0-3.75] vs. 4.0 [3.25-6.0], P < 0.001), sneezing (1.0 [0.0-2.0] vs. 4.0 [2.0-5.0], P < 0.001), rhinorrhea (1.0 [0.0-1.75] vs. 3.0 [2.0-5.75], P = 0.001), nasal obstruction (1.0 [0.0-3.5] vs. 5.0 [3.0-7.0], P < 0.001), and itching (1.0 [0.0-3.0] vs. 4.0 [3.0-5.75], P < 0.001) were substantially lower in the experimental group (Fig. 2).

Dust weight and HDM allergen concentration
No difference in collected dust weight between the 2 groups were detected in week 0. In the experimental group, the collected dust weight was significantly decreased in week 2 (P = 0.006). However, there was no significant change in the control group. The concentrations of Der p1 and Der f1 in the collected dust were similar between the 2 groups at week 0 and did not change during the period of 2 weeks in either group (Table 2).
Table 2
Collected dust weight and the concentration of Der p1 and Der f1

![]()
DISCUSSION
In this study, we evaluated the effects of daily cleaning of bedding with a vacuum cleaner on the symptoms of children with AR. Our results showed a significant improvement in AR symptoms in children whose caregivers vacuumed bedding every day. All AR-related symptoms improved, including total symptom score, sneezing, rhinorrhea, nasal obstruction, and itching after use of the vacuum cleaner in weeks 1 to 2. It suggests that the control of HDM was an effective method to control AR symptoms of children sensitized to HDM when there were no changes in other environmental factors. However, several recent studies have shown different results. A study that evaluated the relationship between vacuum cleaning and sensitization to HDM reported that frequent vacuum cleaning was associated with HDM sensitization and higher serum eosinophil cationic protein concentration.18 Another study of bedroom air quality, vacuuming frequency and the re-admission of pediatric asthma patients, reported that higher levels of airborne Cladosporium and yeast in the child's bedroom, the use of carpet, and the frequent use of vacuum cleaners increased the risk of hospital readmissions due to asthma.19 Wang et al.20 examined the relationship between indoor HDM concentration and AR symptoms. They reported that indoor HDM allergen level affected the severity of AR symptoms. These results suggest that frequent vacuum cleaning accelerates scattering of HDM allergens into the air, therefore exacerbating symptoms of AR. In our study, caregivers cleaned the room when their child went to school or left the house. As a result, the exposure to dust was minimized and the result was different from those of previous studies.
A recent study investigating the effect of daily vacuum cleaning of mattresses on the content of HDM allergens for 8 weeks showed that the amount of dust collected significantly decreased in the first 2 weeks and gradually decreased over a period of 6 weeks and the concentration of HDM allergen tended to decrease steadily for 8 weeks.13 According to another study, the amount of dust collected was influenced by the type and power of the vacuum cleaner. The 1,300 W upright vacuum cleaner collected a larger amount of dust and HDM allergens compared to the 1,100 W canister vacuum cleaner. In the same study, the concentration of HDM allergens in the bottom of a thick carpet was not changed even when it was vacuumed by a vacuum cleaner. Sercombe et al.21 proposed that vacuum cleaning for carpets as a measure of allergen avoidance were unlikely to be successful.21 In our study, the amount of dust collected after 2 weeks of bed cleaning by vacuum cleaner was significantly decreased compared with that collected at the beginning. However, the concentration of HDM allergens in collected dust showed no significant difference before and after experiment. We used a hand-held vacuum cleaner to clean the bedding every day and a general upright vacuum cleaner to collect dust because a hand-held vacuum cleaner was light and easy to operate. These results suggest that, when using a vacuum cleaner to remove the HDM from the bedding, it would be better to use a strong one. However, using a hand-held vacuum cleaner with a weak power every day might help control the symptoms of AR.
Children with AR, similar to those with non-AR, are known to develop rhinitis symptoms in response to nonallergenic irritants, such as cold air, high air pollution, weather change, cigarette smoking, perfume, hair spray, mold odors, bleach, cosmetics, and other substances.22 Therefore, we performed this study for 3 months, during only 1 season, to reduce the effects of non-allergenic irritants and other factors, such as weather changes, that can act as confounding factors.
There were several limitations to our study. First, we performed a single-blind test because it was technically impossible to assess the effectiveness of a vacuum cleaner with a double-blind test. However, we recruited young children between the ages of 6 to 10 who were considered to be relatively less affected by the placebo effect. The caregivers cleaned their child's room when he or she was away from home so that he or she did not know which group he or she belonged to. Secondly, the study had a small sample size and was conducted over a short period of time. However, a short period of study is more advantageous in reducing the factors that can aggravate the symptoms of AR such as upper respiratory infection and weather changes. Thirdly, although the experimental and control groups were randomly assigned, some of the symptom scores in week 0 were different between the 2 groups because of the small sample size. However, the differences between the 2 groups were small in week 0 and all symptom scores significantly decreased only in the experimental group. Finally, we used different vacuum cleaners when collecting dust and cleaning the bedding. This may be one of the reasons why the symptoms of AR were significantly improved, but there was no significant difference in the concentration of HDM allergens in the bedding. However, it would be meaningful to show that using a hand-held vacuum cleaner that is easy to control can help to control AR symptoms.
As a conclusion of this study, daily vacuuming of the bedding for children with AR and sensitized HDM seems to be an effective strategy in the management of children with AR. However, the amount of dust collected was relatively decreased, and the concentration of HDM allergens did not change. Further studies with a large populations and consideration of effect of power difference between vacuum cleaners are warranted.
 XML Download
XML Download