

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pelvic actinomycosis is a rare infectious disease that is known to be associated with long-standing intrauterine device (IUD) use (1). Peritoneal proliferation of Actinomyces induces a chronic, suppurative illness characterized by an infiltrative and granulomatous response with abscess formation (2). Timely recognition of the infection is important to minimize morbidity and to avoid unnecessary surgery (3). However, its rarity, together with the sometimes non-specific imaging and clinico-laboratory findings, complicates the differential diagnosis, leading to delayed diagnosis. In this report, we described a case of pelvic actinomycosis primarily involving the uterine myometrium, mimicking uterine malignancy in a patient with long-standing IUD use.
CASE REPORT
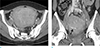
A 56-year-old woman presented to the hemato-oncology department for general weakness, constipation, and abdominal discomfort for 2 months and an 11 kg weight loss over 6 months. Her physical examination was unremarkable with normal vital signs and no fever. The initial laboratory findings on presentation revealed a mild anemia with a hemoglobin level of 11.6 g/dL (normal, 12–16) and hematocrit 35.5% (normal, 36–48), leukocytosis with white blood cell (WBC) count of 24,800/µL (normal, 4,000–10,000/µL) with neutrophilia of 80.9%, and an elevation of C-reactive protein (CRP) to 9.1 mg/dl (normal, 0.0–0.5). The serum albumin level was normal (4.0 g/dL; normal, 3.5–5.2), but total protein (9.0 g/dL; normal, 6.4–8.3) and globulin (5.0 g/dL; normal, 1.2–2.5) were elevated with decreased albumin/globulin ratio (0.8; normal, 1.1–2.0). The patient denied any specific medical or family history except for hypertension. However, the patient had an IUD in situ for approximately 20 years before presentation. An initial contrast-enhanced abdominal CT revealed the uterus to be diffusely enlarged with a poorly defined lesion with heterogeneous enhancement with multiple focal areas of low-attenuation, measuring about 11.6 × 10.3 × 11.3 cm in size (Fig. 1a, b). There was IUD in situ (Fig. 1b). The adjacent sigmoid colon showed mild luminal narrowing with wall thickening and soft tissue stranding in the surrounding mesocolon. Both ovaries were normal, and there was no ascites. Based on the clinico-laboratory suspicion of multiple myeloma, our differential diagnosis included an extramedullary manifestation of multiple myeloma involving the sigmoid colon and mesocolon. The uterine findings were thought to be uterine adenomyosis. The colonoscopic findings of the sigmoid colon revealed mucosal nodularity, and the histopathological results of the colonoscopic biopsy revealed chronic nonspecific inflammation with no malignant cells. The result of the bone marrow biopsy was negative for malignancy. Therefore, the diagnosis was not obvious at the time of initial presentation. The patient was scheduled for laboratory follow-up without any special treatment.
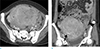
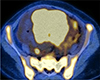
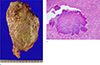
A follow-up laboratory examination performed 3 months later revealed worsening of the anemia with a hemoglobin level of 7.6 g/dL and hematocrit 24.6%, persistent leukocytosis with WBC count of 26,900/µL with neutrophilia of 83.1%, and an elevation of CRP to 14 mg/dl. The bone marrow biopsy was repeated, and the result was again negative for malignancy. Tumor markers, including cancer antigen (CA) 125 (134.7 U/ml; normal, 0–35 U/ml) and CA 19–9 (52.7 U/mL; normal, 2–37), were elevated. A follow-up contrast-enhanced abdominal CT revealed an increase in the size of the poorly-defined uterine lesion with heterogeneous enhancement and multiple focal areas of low-attenuation within the uterus (Fig. 2a, b). Mural thickening of the sigmoid colon with surrounding soft tissue stranding also worsened, and the extent increased to the rectum and perirectal area (Fig. 2b). New findings on the CT included bilateral hydronephrosis and hydroureter with luminal narrowing and wall thickening of the distal ureter bilaterally. On pelvic magnetic resonance imaging (MRI), the lesion of the uterus showed mild high signal intensity on both T1- and T2-weighted images with a poorly defined margin and small cystic foci (Fig. 3a). On gadolinium-enhanced fat-suppressed T1-weighted images, the uterine mass showed heterogeneous enhancement with multiple tiny hypointense foci with ring-like enhancement (Fig. 3b). The lesion showed diffusion restriction on diffusion weighted imaging (Fig. 3c, d). On whole-body 2-deoxy-2-[fluorine-18] fluoro-D-glucose positron emission tomography/computed tomography (PET-CT) scan, the lesion of the uterus was highly avid (maximum standardized uptake value, 20.0 g/ml) (Fig. 4). Diffuse hypermetabolism was seen in the bone marrow cavity of the whole skeletal system and spleen (maximum standardized uptake value, 8.3 g/ml). Based on the clinico-laboratory and imaging findings, the differential diagnosis included pelvic actinomycosis and leiomyosarcoma with direct tumor infiltration to adjacent structures. The patient underwent total abdominal hysterectomy, bilateral salpingo-oophorectomy, and partial omentectomy to confirm the diagnosis and to remove the mass. Cut sections of a huge globoid uterine corpus revealed markedly thickened myometrium with multifocal, ill-defined abscesses and pus-like material (Fig. 5a). The histopathologic findings were characterized by the presence of multifocal microabscesses fused together to form a poorly defined, huge mass. The abscesses contained numerous colonies of actinomycoses in the form of sulfur granules which were composed of masses of gram-positive bacteria with branching filaments arranged in a radial pattern (Fig. 5b). The patient was treated with high doses of penicillin, and her follow-up laboratory findings were normalized.
DISCUSSION
Actinomycosis is an uncommon, chronic, suppurative infection caused by the Actinomyces species. These organisms are seen as part of the normal flora in the oral cavity, gastrointestinal tract and female genital tract. Because the organism is unable to cross normal mucosal barriers, infection occurs when the mucosal barrier is broken, yielding a characteristic granulomatous response with abscess formation, necrosis, and reactive fibrosis (2). Common sites of involvement include the cervicofacial, abdomino-pelvic and thoracic regions, and the abdominopelvic form accounts for 20% of Actinomyces infections (12). The association between pelvic actinomycosis and a long-standing IUD is well known (1). Our patient had an IUD in situ for about 20 years before surgery.
The clinical findings of pelvic actinomycosis are variable and nonspecific and include lower abdominal pain, palpable mass, and weight loss (4). These clinical findings, as well as imaging findings, often lead to the misdiagnosis of neoplasm. However, fever and leukocytosis with elevated CRP levels due to chronic and localized inflammatory processes have been reported (5). In our case, the patient's laboratory findings revealed hyperglobulinemia, which confused the diagnosis upon initial presentation. Although uncertain, we thought that the laboratory finding was associated with infectious disease, and this finding has been reported in animals (6).
Although the radiologic findings are also nonspecific, cross sectional imaging, including CT or MRI, is a useful modality because it provides the extent and characteristics of actinomycosis (3). The CT or MRI in pelvic actinomycosis shows a poorly defined mass with heterogeneous enhancement or a multiloculated fluid collection with irregularly thickened walls. Upon investigating 10 confirmed cases of abdominal actinomycosis, Ha et al. (3) reported that all patients had at least one mass; 7 demonstrated mostly solid masses with focal areas of low attenuation, and three had mostly cystic masses with thickened walls. These findings reflect the histopathologic features of intense fibrosis, granulation tissue, and abscess, which may mimic tubo-ovarian abscess or malignancy, and, subsequently, lead to delayed diagnosis (7). Characteristically, however, these solid and cystic lesions infiltrate adjacent mesenteric fat and organs and extend across tissue planes. It is well known that the infiltrative nature of the lesion is due to the proteolytic enzyme secreted by Actinomyces (5). Interestingly, although quite a few cases of pelvic actinomycosis have been reported (358), there were no cases with imaging findings showing pelvic actinomycosis that involved primarily the uterine myometrium, like our case. In our case, pelvic actinomycosis was misdiagnosed as uterine adenomyosis on initial presentation, and as malignancy, including uterine sarcoma, on follow-up. Other reported cases mimicked pelvic inflammatory disease with tubo-ovarian abscesses or ovarian malignancy, leading to delayed diagnosis. However, extensive infiltration to adjacent tissue manifesting as wall thickening of the rectosigmoid colon, hydroureter, and soft tissue stranding are not unusual findings for uterine malignancy. In addition, on gadolinium-enhanced MR images, the huge uterine mass revealed multiple tiny hypointense foci with ring-like enhancement and diffusion restriction, correlating with multiple microabscesses on the macro- and microscopic findings of the surgical specimen. These findings were also atypical for a malignant mass. Alfuhaid et al. (9) described similar findings in ovarian masses: a salt and pepper appearance consistent with microabscesses. Pelvic actinomycosis appears as a hypermetabolic pelvic mass on F-18 FDG PET/CT scan (8). Therefore, the FDG PET/CT scan has no additional value in distinguishing pelvic actinomycosis from malignancy.
Definitive diagnosis of actinomycosis can generally be made by histologic identification of sulfur granules and/or culture of Actinomyces (13). Actinomycosis can be managed with high dose antibiotics, although surgical resection is often required for definite diagnosis and assistance with medical treatment.
In conclusion, pelvic actinomycosis has nonspecific imaging and clinico-laboratory findings that can mimic multiple disease processes. However, pelvic actinomycosis must be included in the differential diagnoses of patients with an infiltrative pelvic mass extending across tissue planes or in patients with findings of multiple microabscesses, particularly in a patient with an IUD, even the lesion primarily involve the uterus. Early diagnosis is critical to minimize delayed diagnosis and subsequent disease morbidity.

 XML Download
XML Download