

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Studies have suggested that most people can adapt to traumatic loss with a reduction in grief intensity in about 6 months.1 However, people afflicted with complicated grief (CG) are essentially frozen or stuck in a state of chronic mourning for 6–12 months or longer after the loss.2 The prevalence of CG varies depending on studies. According to a previous study, CG occurs in about 10% of individuals who have experienced bereavement.3 Individuals with CG also suffer from intense longing or yearning for the dead person. CG is known to cause significant distress and functional impairment clinically.4 Therefore, it is clinically meaningful to conduct a study defining the diagnostic criteria for CG and identify factors affecting its onset, course, and treatment.
CG is closely related to other psychiatric symptoms. The prevalence of CG is high among individuals with a history of psychiatric disorder.3 Grief is known to affect the onset and course of other psychiatric symptoms.3 Grief often serves as a stress factor that increases the risk of depression and anxiety disorders, panic disorder, post-traumatic stress disorder (PTSD), insomnia, suicidal thoughts and attempts, and challenges associated with alcohol abuse.567 Particularly, when normal grief is followed by CG, he or she is more likely to manifest comorbid mental disorders. A study has found that 75.2% of individuals diagnosed with CG manifest other psychiatric symptoms of axis I in Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5).78 Due to correlation between CG and other psychiatric symptoms, previous studies have attempted to elucidate CG as a symptom associated with depressive disorder, PTSD, or adjustment disorder rather than as an independent diagnosis.29 However, several studies have suggested that CG is an independent disorder that can be distinguished from other psychiatric disorders.110 In recent years, persistent complex bereavement disorder has been included in the criteria for ‘conditions for further study’ in DSM-5. Further studies are required to determine the correlation between other psychiatric symptoms and CG for independent diagnosis of CG under diagnostic criteria of DSM officially.
Previous studies on the relationship between CG and other psychiatric symptoms have mainly investigated how clinically different symptoms of CG and other psychiatric symptoms are distinguished and what symptoms are mainly coexisted with CG.5111213 Few studies have explored the severity of other coexisting psychiatric symptoms or longitudinal effects of change of coexisting psychiatric symptoms.1415 Accurate diagnosis of CG for prompt intervention requires insight into the effect of other coexisting psychiatric symptoms on change of CG. In particular, a few studies have reported high prevalence of CG and high probability of other psychiatric symptoms in those suffering from traumatic loss.1617 However, studies analyzing the impact of other psychiatric symptoms on change of CG in those afflicted with traumatic loss are limited. Therefore, we conducted a longitudinal study of change in CG involving bereaved families following traumatic loss in the Sewol ferry disaster. We assessed the severity of CG and severity of other psychiatric symptoms including depression and anxiety disorders, PTSD, post-traumatic embitterment disorder (PTED), insomnia, and suicidal risk at 18 months (Time 1) and 30 months (Time 2) after the loss. The objective of this study was to investigate the effect of severity of other psychiatric symptoms at Time 1 and the change of coexisting psychiatric symptoms at Time 2 on change of CG.
METHODS
Participants
We contacted representatives of families who lost their family member in the Sewol ferry disaster at Ansan, Korea, to explain the purpose of this study. Study goals conveyed included identification of the risk and prognostic factors affecting mental health of individuals who had experienced death of a family member. After obtaining agreement from representatives, 93 bereaved family members were surveyed for Time 1 after obtaining informed consent from all participants. Psychiatrists specializing in the field of disaster mental health interviewed participants. Sociodemographic data and psychiatric scales were retrieved from self-reporting questionnaires. One of them died of lung cancer within a year. Thirty subjects refused to participate in the longitudinal study. Six were excluded because of missing data of psychiatric scales. Finally, 56 (60.2%) of 93 subjects were included in the analysis. A flow diagram of the participants in this longitudinal study is presented in Fig. 1.
Fig. 1
Flow diagram of participants in the study of bereaved family members of the Sewol ferry disaster.
ICG = inventory of complicated grief, PHQ-9 = patient health questionnaire-9, GAD-7 = generalized anxiety disorder 7-item questionnaire, PCL-5 = PTSD checklist-5, ISI = insomnia severity index, PTED = post-traumatic embitterment disorder.

Those lost to attritions (n = 37, 39.8%) did not differ from study participants in terms of sociodemographic factors (age: t = 1.506, P = 0.136; gender: χ2 = 0.797, P = 0.399; marital status: χ2 = 3.074, P = 0.233; religion: χ2 = 7.493, P = 0.130; and education: χ2 = 3.491, P = 0.206) or psychiatric symptoms (depression: t = 0.673, P = 0.503; anxiety: t = 0.616, P = 0.540; PTSD: t = 0.891, P = 0.375; CG: t = 1.159, P = 0.250; and embitterment, t = 0.559, P = 0.578) at Time 1.
Measures
Sociodemographic variables included age, gender, relationship with a victim, educational level, marital status, religion, total monthly income of the household, experience of visiting a mental hospital or undergoing counseling for psychological therapy before the accident, and birth order of victim. We used self-reported questionnaires to investigate CG and other psychiatric symptoms.
Inventory complicated grief (ICG)
ICG is a self-rated inventory developed to evaluate the symptom of grief in order to predict functional mental disorders.18 The instrument consists of 19 items related to subjects' immediate bereavement-related thoughts and behaviors. Each item included five response options with scores ranging from 0 to 4. Rating score of ICG ranged from 0 to 76, with a score of 25 or higher suggesting higher risk and warranting therapeutic intervention. There is one validation study about Korean version of ICG in Korean adolescents. It had acceptable psychometric properties.19
Patient health questionnaire-9 (PHQ-9)
PHQ-9 is an inventory used to screen, diagnose, monitor and measure the severity of depression.20 The PHQ-9 includes 9 questions to rate the frequency of symptoms according to scoring severity index from 0 to 3. The score ranges from 0 to 27. Scores from 8 to 11 are used as cut-off for the diagnosis of major depressive disorder. Its total score is interpreted as follows: no clinically significant depression, score of 0–4; mild depression, score of 5–9; moderate depression, score of 10–19; and severe depression, score of 20–27. The Korean version of the PHQ-9 has good psychometric properties. The Cronbach's α value of all items was 0.852. The sensitivity and specificity of the Korean version of PHQ-9 were 81.8% and 89.9%, respectively.20
Generalized anxiety disorder 7-item questionnaire (GAD-7) screener
GAD-7 represents a short, self-reported questionnaire developed for early detection of generalized anxiety disorder.21 It includes 7 items. Each item has a score of 0 to 3. Thus, the rating score of GAD-7 ranges from 0 to 21. A score of 10 is used as the cut-off for the diagnosis of generalized anxiety disorder. Its total score is interpreted as follows: no anxiety, score of 0–4; mild anxiety, score of 5–9; moderate anxiety, score of 10–14; and severe anxiety, score of 15–21. The Korean version of the GAD-7 has good psychometric properties. Cronbach's α coefficient was 0.924. At a cutoff score of 6, the GAD-7 had a sensitivity of 92.2%, a specificity of 89.1%, a positive predictive value of 69.1%, and a negative predictive value of 97.7%.22
PTSD checklist-5 (PCL-5)
PCL-5 is a self-rated inventory developed for screening PTSD symptoms based on DSM-5 criteria.23 It includes 20 items. Each item has five response options with score ranging from 0 to 4. Total score of PCL-5 scale ranges from 0 to 80. A score of 38 is used as the cut-off for PTSD diagnosis.
PTED
PTED self-rating scale is a questionnaire comprising 19 items. Each item has five response options with score ranging from 0 to 4.24 It is used to evaluate bitter reactions to negative life events. A mean total score of ≥ 1.6 (total score over, 30.4) suggests prolonged embitterment with strong clinical relevance. A mean total score of ≥ 2.5 (total score over, 47.5) indicates reactive embitterment of clinically significant intensity. The test-retest reliability of the Korean version of PTED Scale was good (r = 0.76) and the internal consistency was very high (Cronbach's α = 0.962).25
Insomnia severity index (ISI)
ISI is used as a screening measure brief of insomnia.26 The ISI is a questionnaire comprising 7 items assessing the nature, severity, and effects of insomnia. Each item carries five response options with a score ranging from 0 to 4. Its total score ranges from 0 to 28. Total score is interpreted as follows: no clinically significant insomnia, score of 0–7; sub-threshold insomnia, score of 8–14; clinically moderate insomnia, score of 15–21; and clinically severe insomnia, score of 22–28. The Korean version of the ISI has good psychometric properties, the internal consistency the ISI-K total score was confirmed by a Cronbach's α of 0.92.27
P4 suicidality screener
P4 was used for suicidality screening as a self-rated structured algorithm comprising 4 items of past suicide attempts, suicidal ideation, probability of completing suicide, and preventive factors.28 Suicidal risk assessments were divided into minimal, lower, and higher risk.
Functional social support questionnaire (FSSQ)
The FSSQ is a self-rated questionnaire composed of 14 items. Each item has five response options with scores ranging from 1 to 5. Thus, its total score ranges from 14 to 70.29 The lower the total score, the higher the degree of social support.
Data analysis
Frequency analysis was used to determine the probability of other coexisting psychiatric symptoms among subjects manifesting CG at Time 1. Following univariate analysis of demographic variables, we performed independent t-test, one-way analysis of variance and Pearson correlation for univariate analysis to identify mean difference among subgroups of each demographic variable and correlation between change of CG and each demographic variable. We used paired same t-test for analysis of differences in total scores of ICG, PHQ-9, GAD-7, PCL-5, PTED, and ISI over a year. The McNemar-Bowker test was used to analyze changes in suicidality assessed by P4 over a one-year period.
Finally, we performed Linear mixed analyses to analyze the effect of severity of other psychiatric symptoms or change of coexisting psychiatric symptoms on change of CG. We calculated the change of coexisting psychiatric symptoms by subtracting the total score of each scale of Time 1 from the total score of each scale at Time 2 and then dividing by the scores of Time 1. The model included participants as a random effect. Time and severity of other psychiatric symptoms at Time 1 or change of CG were included as fixed factors. The model also included interaction between time and severity of other psychiatric symptoms as Time1 or change of CG, and a fixed intercepts. Additionally, the analysis was performed including variables of fixed effects (age, gender, educational level, relationship with victim, history of psychological therapy, social support at Time 1) to control these factors. All statistical analyses were performed using SPSS version 21.0 for Windows (IBM Corp., Armonk, NY, USA).
Ethics statement
The study procedure was approved by the Institutional Review Boards of the ethical committee of the Seoul St. Mary's Hospital at the Catholic University of Korea (registration No. KC15OIMI0261). Full right was given to the study participants to refuse and withdraw from participation at any time. Informed written consent was obtained from the participants.
RESULTS
General description of total participants
Table 1 shows sociodemographic data and results of univariate analysis correlating sociodemographic variables and change of CG. Bereaved family members included parents (n = 48, 85.7%), siblings (n = 4, 7.1%), grandparents (n = 2, 3.0%), aunt (n = 1, 1.5%), and wife (n = 1, 1.5%) who lived with victims. We analyzed possible correlation between change of CG and each of parameters of age, gender, relationship to the person who died, educational level, marital status, religion, the total levels of monthly household income, visits to a mental hospital or counseling for psychological therapy before the accident, or birth order of victims. As a result of the analysis, no variable showed a significant difference in change of CG between subgroups for each variable shown in Table 1. Further, no significant correlation existed between the level of subjective social support and change of CG.
Table 1
General characteristics of the sample (Time 1, n = 56)

Average change of psychiatric symptoms from Time 1 to Time 2
Based on recommended cut-off scores, we examined average score severity at Time 1 and Time 2. All but 1 participants had total PHQ-9 score exceeding 5 (98.1%) at Time 1. At Time 2, the number of people without depression increased to five (90.7%). Results showed that 83.3% of total participants at Time 1 and 75.9% of participants at Time 2 had total GAD-7 score over 5. Using cut-off score ≥ 38 for PCL-5, 74.1% of participants at Time 1 and 77.8% at Time 2 were diagnosed with PTSD. Thirty-five (64.8%) participants at both Time 1 and Time 2 showed severe embitterment. In ISI evaluation, 75.9% of subjects at Time 1 and 81.5% at Time 2 showed sleep problems with an ISI total score greater than 8. In suicide risk assessment using P4, 48.1% of participants at Time 1 and 40.7% at Time 2 exhibited suicide risk. Two participants with a total ICG score less than 25 at Time 1 showed an ICG score higher than 25 at Time 2.
Next, we used paired sample t-test for analysis of change of CG and change of coexisting psychiatric symptoms for a year (Table 2). Results showed no significant difference in severity of psychiatric symptoms except depression (t = −5.383, P < 0.001) between Time 1 and Time 2. In the case of suicidality, the McNemar-Bowker test was used in the crossover study as P4 represented a nominal variable. Results showed no significant difference in suicide risk during one year (t = 2.416, df = 3, P = 0.491).
Table 2
Differences in psychiatric symptoms scores at Time 1 and Time 2 (n = 56)
Data are shown as mean ± standard deviation. Difference in P4 was analyzed with McNemar-Bowker test.
SD = standard deviation, Diff. = difference, ICG = inventory of complicated grief, PHQ-9 = patient health questionnaire-9, GAD-7 = generalized anxiety disorder 7-item questionnaire, PCL-5 = PTSD checklist-5, PTED = post-traumatic embitterment disorder, ISI = insomnia severity index.
aAt 18 months after the disaster; bAt 30 months after the disaster.
Change of coexisting psychiatric symptoms associated with change of CG from Time 1 to Time 2
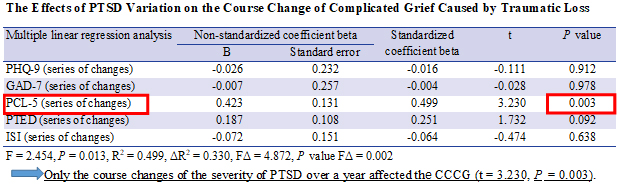
Table 3 presents results of Linear mixed models of change of coexisting psychiatric symptoms related to change of CG. In order to control confounding factors, age, gender, educational level, previous mental hospital visits or a history of counseling for psychological therapy before the accident, relationship to the person who died, and level of subjective social support (FSSQ) were included in the analysis. Among independent variables, aggravation of PTSD symptoms (PCL-5) had a significant effect on change of CG over a year (df = 1,45, F = 9.733, P = 0.003).
Table 3
Results of linear mixed models of change in coexisting psychiatric symptoms related to change of CG
Age, gender, educational level, previous mental hospital visits, or a history of counseling for psychological therapy before the accident, relationship to the person who died, and level of subjective social support (FSSQ) were included as covariates in the analysis.
CG = complicated grief, PTSD = post-traumatic stress disorder, FSSQ = functional social support questionnaire.
Severity of other psychiatric symptoms at Time 1 associated with change of CG from Time 1 to Time 2
Table 4 shows results of Linear mixed models of the severity of other psychiatric symptoms at Time 1 related to change of CG with controlled covariates. Total score of PHQ-9, GAD-7, PCL-5, PTED, or ISI at Time 1 did not significantly affect change of CG for a year These results suggested that each severity of other psychiatric symptoms in Time 1 did not affect change of CG for a year.
Table 4
Results of linear mixed models of the severity of other psychiatric symptoms at Time 1 related to change of CG
Age, gender, educational level, previous mental hospital visits or a history of counseling for psychological therapy before the accident, relationship to the person who died, and level of subjective social support (FSSQ) were included as covariates in the analysis.
CG = complicated grief, PTSD = post-traumatic stress disorder, FSSQ = functional social support questionnaire.
a18 months after the disaster.
DISCUSSION
This study aimed to investigate effects of the severity and changes in severity of coexisting psychiatric symptoms on change of CG. Elucidation of other psychiatric symptoms affecting change of CG can facilitate the evaluation and therapeutic management of the afflicted individuals. These efforts can also alleviate CG and enhance the quality of life of individuals with CG. This study suggests that only a year of PTSD aggravation affects the severity of CG. None of the other psychiatric disorders except for PTSD and no other demographic variable evaluated at Time 1 showed a significant correlation with change of CG.
Individuals who experienced bereavement might manifest both PTSD and CG symptoms.13 A previous study has investigated the role of CG as an independent disorder distinct from PTSD.13 Results showed that most CG patients failed to meet the diagnostic criteria for PTSD, although these two disorders had different clinical course. PTSD and CG are different in that PTSD is characterized by ‘fear’ while CG involves ‘sadness’ and ‘yearning for the deceased.’5 The DSM-IV-TR diagnostic criteria excluded normal bereavement as a PTSD symptom. However, ‘A criteria’ of PTSD in DSM5 includes the case of indirect exposure to a violent or accidental trauma/death. Thus, bereavement due to traumatic event can be diagnosed with PTSD. CG is also included as a persistent complex bereavement disorder under ‘conditions for further study’ section. It is likely to be included as an independent formal diagnosis in subsequent DSM versions.
On the other hand, previous studies have also reported a positive association between severity of CG and PTSD.1130 High rates of coexistence for these two disorders have also been reported.1112 In the case of traumatic loss due to sudden and violent death, prevalence of CG and PTSD will increase concurrently. In general, CG prevalence rate is about 10%. However, the prevalence of CG alone was increased to 78% for cases experiencing violent death.31 The probability of PTSD coexistence is also increased up to 65%.32 The association between PTSD and CG can also be explained by intrusion symptoms.33 Furthermore, previous studies have suggested that intrusion symptoms of PTSD might interfere with the progress of normal grief.3334 Consistent with these results, the present study also found a longitudinal association of CG with PTSD.
Contrary to our study, a previous longitudinal study15 about association between CG and PTSD have revealed that prolonged grief symptoms (PGS) can mediate 83% of post-traumatic stress symptoms (PTS) over a period of time while PTS can mediate 17% of its relationship with PGS over a period of time. That study showed that changes in PGS might precede and potentially impact changes in PTS directly. However, in that study, 89% of participants experienced a period of spousal illness preceding the death, suggesting that the previous study did not investigate traumatic loss exclusively. Another recent study14 has reported that PTSD does not have a significant relationship with CG after a year whereas CG has a significant association with PTSD after a year. However, 89% of subjects participated in that study also experienced bereavement from natural causes while only 11% of subjects reported bereavement from unnatural deaths such as suicides, accidents, and homicides. Therefore, considering the type of loss may be important in future studies on the relationship between CG and PTSD. Furthermore, all of these above-mentioned studies and the present study used self-reported results. Thus, further studies are needed in the future through clinical diagnosis of CG and PTSD.
To the best of our knowledge, this is the first study to investigate the effect of PTSD on change of CG in bereaved families who have experienced traumatic loss. In addition, this study not only determined the relationship between PTSD and CG, but also investigated the effect of changes in severity of coexisting psychiatric symptoms on change of CG. Results of this study suggest that it is important to continuously evaluate and treat various coexisting psychiatric disorders, especially for PTSD in order to manage the course of CG of traumatic loss. Further studies analyzing effects of PTSD and other coexisting psychiatric disorders on change of CG are required.
In this study, psychiatric symptoms showed higher prevalence than those in other studies of traumatic losses.1112 In the present study, 84 of 87 participants suffered from CG even after 18 months since the accident (Time 1). After 30 months since the accident (Time 2), 54 of 56 people who were followed up were diagnosed with CG. Participants also showed high prevalence rates of other coexisting psychiatric symptoms. The prevalence of psychiatric symptoms in bereaved families can be greatly influenced by external factors such as the relationship between the deceased and bereaved families and the type of death. In particular, individuals experiencing loss of children or spouse show high prevalence of psychiatric symptoms.35 Losses due to shocking incidents such as the September 11 attacks are associated with even longer and intense periods of mourning.16 In addition, the fact that the Sewol ferry accident is classified as a man-made disaster can also affect the prevalence of psychiatric symptoms.36 It is also important to consider that participants are in the midst of political issues, and that the problems associated with reimbursement are continuing. Some participants were also probably in the process of lawsuits or compensation. These may affect research participation and research results. Thus, the fact that these self-reported results were from selection biased samples should be also considered when interpreting these results.
There was no significant change in the severity of psychiatric symptoms except for depression in the present study. Although mourning symptoms can be alleviated over time generally, repeated stress conditions regarding Sewol ferry disaster may trigger continuously CG and persist CG.37 The cause of the accident is still under investigation. Such vagueness is an important aspect that still bothers participants and affects their psychiatric symptoms. The previous result also showing that prevalence of PTSD is increased over time after intentional traumatic events, indicating that the overall public health burden of PTSD is greater in those who are exposed to intentional traumatic events.38 Conversely, depressive symptom was decreased in a year while CG and other psychiatric symptoms were not changed. In addition, depressive symptoms had no association with change of CG in the present study. Although CG may share some symptoms and/or coexist with depressive disorder, our results support the opinion of a previous study suggesting that symptoms of CG are distinct from symptoms of bereavement-related depression.39 There is emerging evidence suggesting that CG has a unique clinical entity different from depression. Unlike depression, CG has been found to persist despite passage of time or treatment of the bereaved with tricyclic antidepressants, suggesting that CG might resolve differently than depression.39 These two symptoms (CG and depression) also showed different mental and physical health outcomes.39
Fundamentally, CG begins with negative events. Although negative life events are linked primarily or secondarily to depression, they also show a reciprocal relationship where earlier depressive symptoms can predict later negative events.40 Our study showed that change of CG was only related to PTSD, not depression or other psychiatric symptoms. This finding seemed to be associated with this result. Further research is needed to determine whether these fundamental differences could determine the entity of these two symptoms.
This study has several limitations. First, this study included a small number of participants. They were deeply distrustful of the government and the society. They barely trusted the privacy of the information obtained by researchers. Therefore, participation rate was not high. This study might also have selection-bias. However, this study was conducted with a very homogenous group of bereaved families who lost their close family member in the traumatic event of Sewol ferry disaster on the same day. Large-scale studies may provide additional results to highlight factors affecting the progression of CG, including those derived from this study. Second, a limited number of psychiatric visits or counseling sessions for psychological therapy before the accident were included in this study while other individual traumatic events were not controlled for. However, as discussed above, subjects acted as a group since the accident. They largely shared additional traumatic experiences reproduced by governmental actions after the accident. Third, the starting point of this study was 18 months after the accident. This study, as part of the national cohort study, prompted the need for a national study investigating individuals and families experiencing disasters after Sewol ferry disaster. However, the planning for the study was extensive and prolonged. It was complicated by difficulties in obtaining participants' informed consent. Although they were not followed up immediately after the accident, this long-term longitudinal study of the course of CG appears meaningful. Finally, this study is limited by its dependence on self-reported questionnaires. Furthermore, a wide range of factors such as substance use that could influence the change of CG were not considered in the analysis. Future studies will need to consider a variety of factors that can affect change of CG.
Despite these limitations mentioned above, to the best of our knowledge, this study is the first of its kind to analyze effect of change of coexisting psychiatric symptoms on change of CG of bereaved families in the aftermath of the Sewol ferry disaster and experience of long-term CG. Only changes in the severity of PTSD over a year affected change of CG. Thus, it is important to accurately assess the severity of PTSD and its course for prompt evaluation of PTSD and treatment of long-term CG, especially for families afflicted with traumatic bereavement.
 XML Download
XML Download