

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Kivexa is a fixed-dose combination tablet containing 600 mg of abacavir sulfate (ABC) and 300 mg of lamivudine (3TC), which is approved for treatment of human immunodeficiency virus (HIV) infection. Lamivudine and abacavir, the components of Kivexa, are recommended in international and local guidelines and widely used since their approval in 1995 and 1998 worldwide [123]. Triple combination treatment, as known as highly active antiretroviral therapy (HAART), has been long established as the standard treatment for HIV, using two nucleoside/tide reverse transcriptase inhibitors plus one other agent from a protease inhibitor (PI) or a non-nucleoside/tide reverse transcriptase inhibitor (NNRTI) class. Since then, the dual nucleoside combination of ABC and 3TC demonstrated antiretroviral efficacy when used with one other antiretroviral agents [456]. Kivexa has been developed as a fixed-dose combination to improve patients' convenience and improve adherence.
Kivexa was approved in Korea in 2011. We conducted a post-marketing surveillance study to evaluate safety and effectiveness of Kivexa from the real world setting.
Materials and Methods
1. Study design and population
An open label, multi-center, non-interventional post-marketing surveillance was conducted to monitor safety and effectiveness of Kivexa from July 2011 to July 2017 in 23 hospitals in Korea. Patients with confirmed HIV infection taking Kivexa according to prescribing information were included. Subjects who commenced Kivexa before the study period were also included and the observation started on the day of consent. Patients who have contraindication to the component of Kivexa such as moderate to severe hepatic impairment (Child-pugh class B or C), renal insufficiency (eGFR<50 mL/min/1.73 m2) or confirmed HLA-B*5701 carriers were excluded. Primary outcome was defined as the occurrence of any adverse events during the study period. Secondary outcomes included the occurrence of adverse drug reactions, the occurrence of serious adverse events and the effectiveness of Kivexa. Effectiveness was measured by the changes of proportion of subjects with plasma HIV-1 RNA less than 50 copies/ml throughout the study period. Regarding the non-interventional study design, a subjective assessment of ‘clinical improvement’ was also included for subjects with observation period greater than 24 weeks. A total of 780 subjects were planned to be enrolled with consideration of an estimated 20% drop out rate, to provide 600 evaluable subjects for the primary analysis. This study was approved by the Institutional Review Board of each participating hospitals.
2. Definitions
Based on WHO-ART 092 [7], an adverse event (AE) was defined as any untoward medical occurrence in a subject temporally associated with the use of a Kivexa, regardless of relation to the medicinal product. Serious adverse event (SAE) was defined as any untoward medical occurrence that with any dose that; 1) results in death, 2) is life-threatening, 3) requires inpatient hospitalization or prolongation of existing hospitalization, 4) results in persistent or significant disability/incapacity, or 5) is a congenital anomaly/birth defect. An adverse drug reaction (ADR) was defined as all noxious and unintended responses related to Kivexa administration. Physicians classified the causality into 6 category; “certain”, “probable/likely”, “possible”, “unlikely”, “conditional/unclassified,” and “unassessable/unclassifiable” by WHO-UMC causality categories [8]. If the causality between Kivexa and AEs are considered “certain”, “probable/likely”, “possible” “conditional/unclassified,” and “unassessable/unclassifiable,” AEs were classified as ADRs. ADRs that are not stated in Korean prescribing information were classified as unexpected ADR.
3. Demographic and clinical data
Each physician decided patient visit schedules based on their routine practices. At the initial visit, demographic information (including subject's sex, age, weight, and pregnancy), medical history (including result of HLA-B*5701 test, allergy history, renal impairment, hepatic impairment, other concomitant diseases, duration on Kivexa, time since HIV diagnosis and HIV treatment history), concomitant medications, laboratory values including viral load, CD4+ cell counts (if any) were recorded. Because of the non-interventional design of the study, not all the subjects had their HIV-1 RNA viral load and CD4+ T cell counts every visit. Physicians were guided to record any treatment-emergent adverse events during the follow up visits. Any results of HIV RNA viral load and CD4+T cell counts as a part of standard of care within the study period were collected for analysis. At 48-week visit, the effectiveness of Kivexa was subjectively evaluated as “improved”, “no change”, “worsened” or “not assessed” by the investigator's medical judgment.
4. Statistical analysis
Continuous variables were expressed as the mean±standard deviation and discrete variables are expressed as the frequency and rate. Once all AEs were classified by preferred terms and system-organ classes, the frequency and percentage of each AE were calculated. Statistical calculation was carried out using SAS version 9.0 (SAS Institute Inc, Cary, NC, USA).
Results
1. Characteristics of study participants
Among 640 enrollments, a total of 600 patients were included in safety analysis within the 6 years of post-marketing surveillance, excluding 40 subjects with protocol deviation (Fig. 1). Total observation period was 1,003.8 person-years. 551 subjects (91.8%) were male. Age was 47.2 ± 12.4 and 54 (9.0%) subjects were over 65 years old. 19.7% of participants were diagnosed with HIV infection within a year at the study entry. 312 subjects were naïve to abacavir. Four of the participants reported pregnancy during observation period. 19 subjects with a human leukocyte antigen (HLA)-B*5701 test was all negative. During the screening, there were no patients positive for HLA-B*5701. Patients on Kivexa plus a PI, NNRTI and integrase strand transfer inhibitor (INI) were 58.3%, 25.2% and 13.8%, respectively. Six of the participants had renal impairments (chronic kidney disease stage 2 to 3), 18 subjects had hepatic impairment with hepatic impairment score of Child-Pugh class A (Table 1).

Table 1
Baseline characteristics of study participants

2. Safety and Tolerability
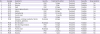
Three hundred and ten subjects reported 674 adverse events. The incidence of upper respiratory infection (10.83%, 65/600) was the most common, followed by diarrhea (3.33%, 20/600) and nausea (3.00%, 18/600). A total of 109 cases with adverse drug reactions were reported by 71 subjects. Nausea (2.33%, 14/600) was the most common, followed by vomiting (1.00%, 6/600), diarrhea and dizziness (0.8%, 5/600 each) (Table 2). The incidence of adverse events according to the class of co-administered antiretroviral agents is shown in Table 3.
Table 2
Adverse drug reaction and reported in >1 subjects and its expectedness
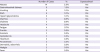
Table 3
The incidence of adverse events according to the class of co-administered antiretroviral agents

Subjects who switched antiretroviral regimen while on Kivexa were included both antiretroviral groups, resulting in a total number of subjects that exceed 600.
Incidence: number of subjects who reported adverse events/number of subjects who were on each class of antiretroviral agent at the time of adverse event
CI, confidence interval. 95% CI was calculated by Exact Method.
aChi-square test p-value for the occurrence of adverse events according to the use of each antiretroviral agents.
Thirty-one cases of serious adverse event were reported from 25 subjects. None of the cases were considered as Kivexa related based on physician's medical judgement. A 59 years old male hospitalized with unstable angina. He was diagnosed with HIV infection 8 years before, had been taking Kivexa with darunavir (400 mg, twice a day) and norvir (100 mg, once a day) at the time of unstable angina for over three years. No underlying disease but spinal stenosis reported, and he was smoker. The investigator reported the event was not associated with Kivexa administration, and the patient continued Kivexa (Table 4).
Table 4
Clinical characteristics of cases with serious adverse events

To the query to assess whether the adverse event is related to hypersensitivity or allergic reaction, 15 subjects were suggested as possible allergic reactions. All 15 subjects were tested and did not have HLA-B*5701. Details of cases and clinical outcomes are listed in Table 5. None of the suggested allergic cases met the criteria for serious adverse event.
Table 5
Clinical characteristics of cases with suggested hypersensitivity or allergic reaction
Four of the 49 female subjects became pregnant during the study period. One of the two subjects who were pregnant at the time of enrollment reported tongue pain (mild, resolved, causality unassessable), and one subject of the two who became pregnant during the observation period reported hypertriglyceridemia (mild, unresolved, causality possible), heartburn (mild, resolved, causality unlikely), and vomiting (mild, resolved, causality unlikely). There were no adverse birth outcomes.
3. Effectiveness
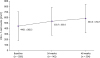
Among 600 patients with safety evaluation, 552 subjects were assessed for 48 week effectiveness. Forty-eight subjects were excluded because their observation period was less than 48 weeks. By subjective medical judgement of the investigator, 459 (83.2%) were evaluated as ‘improved’, 91 (16.5%) were ‘no change’, and 2 (0.4%) were ‘worsened’. HIV RNA results of baseline and 48 weeks of observation period were collected from 505 subjects. From 196 subjects with HIV RNA >50 copies/mL at the beginning of observation, 172 (87.8%) were fully suppressed to under 50 copies/mL at 48 week. Of 309 patients with HIV RNA <50 copies/mL at baseline, 292 (94.5%) stayed suppressed through 48 weeks of Kivexa administration (Fig. 2). CD4+T cell count increased from 442.1 ± 262.3 cells/mm3 at baseline to 580.6 ± 258.7 cells/mm3 at 48 weeks of follow up from patients with a baseline and week 48 observation (P <0.0001) (Fig. 3).
Figure 2
Proportion of subjects with human immunodeficiency virus (HIV) RNA <50 copies/mL at baseline and 48 weeks of Kivexa treatment.
A. 1) at baseline, 2) at 48 weeks after Kivexa treatment.
B. Proportion of subjects who achieved HIV RNA <50 copies/mL at 48 weeks 1) in subjects with HIV RNA >50 copies/mL at baseline, 2) in subjects with HIV RNA <50 copies/mL at baseline.

Discussion
This post marketing surveillance (PMS) has been conducted to observe the safety of Kivexa in clinical setting as a requirement of Korean regulatory authority.
We observed a total of 1,004 person-years with 600 subjects for 6 years, from 2011 to 2017. The high proportion of male subjects (90%) and the proportion of elderly subjects over 65 years old (9.0%) is somewhat reflective of the HIV population in Korea [910]. Over a half of the subjects took Kivexa with PI, which also reflects high usage of PI in Korea, compared to other Asian countries [1112]. Since INIs were introduced from 2010 in Korea, subjects that used Kivexa with INIs began to be enrolled later, and thus have lower representation in the study population (Table 1).
Kivexa generally showed good tolerability, yet there were adverse events associated with Kivexa administration. The three most common adverse drug reactions were nausea, gastrointestinal distress, and vomiting. This observation was different from the previous 3TC and Ziagen PMS reports where diarrhea was observed as the most common adverse events (4.72%, 1.8%, respectively), however the gastrointestinal trouble accounted were similar [13]. When list up all the adverse events that reported from over 1 subject, there were no events related to cardiac events.
Subjects taking NNRTI with Kivexa reported less AE than those taking PI and INI, and those receiving INI with Kivexa reported more AE than those receiving NNRTI and PI (Table 3). This incidence comparison has limitations because it did not take into account the causality with Kivexa, and each class includes couple of different antiretroviral agents.
A total of 25 subjects experienced serious adverse events. Among them, one 59 years old male reported unstable angina. He had no underlying disease related to cardiovascular risk factors but had a history of spinal stenosis. Since the association between abacavir and ischemic heart is still inconclusive [14151617], the occurrence of ischemic heart disease was subject for close observation. The investigator evaluated the unstable angina case unrelated to the study drug, and there was no further other cardiac event was reported. Thus, in this Ziagen PMS report, there were no drug-related ischemic heart disease observed with the administration abacavir in Korea [13].
Investigators were asked to evaluate any adverse event related to allergic reactions or suspected hypersensitivity, 15 adverse events 15 cases were suggested as possible allergic reactions (Table 5). A 48 years old male presented nausea, vomiting, headache, febrile sensation and giddiness on his 48th day of Kivexa administration. He did not have a previous HLA-B*5701 test. The investigator reported this might be related to Kivexa, and the patient's symptoms resolved after he stopped Kivexa. The series of symptoms and resolution of symptoms after Kivexa cessation suggest this as a possible case of abacavir hypersensitivity. Abacavir hypersensitivity reaction can occur in 5–8% of patients and can be lead to serious toxicity without appropriate and timely management [1819]. It is well documented that abacavir hypersensitivity is strongly associated with HLA-B*5701 allele, thus HLA-B*5701 test before commencing abacavir containing regimens are recommended. However, the prevalence of HLA-B*5701 is quite low in Asian population (0–1%) compared with those of other ethnicities (3–4.98%) [20212223]. One report evaluated the prevalence of HLA-B*5701 allele among the Korean HIV patients, however there were no subjects in study with a positive HLA-B*5701. The authors suggested that it might be more cost-effective to closely monitor the occurrence of hypersensitivity compared to testing for all the Korean HIV population [21]. Although the responsible company constantly communicates the necessity of HLA-B*5701 test and the risk of ABC hypersensitivity, the testing rate for HLA-B*5701 of this study was very low, which reflects the clinical significance of HLA-B*5701 testing in real world in Korea.
In the effectiveness analysis, we observed positive virologic and immunologic improvement with Kivexa contained regimen with an increasing of proportion of subjects with HIV RNA below 50 copies/mL and an increasing mean CD4+T-cell counts. Kivexa was administrated with either PI, NNRTI or INI in most cases, and thus it was not feasible to assess the effectiveness of Kivexa own. And with the design of post-marketing surveillance, we could not analyze the cases with virologic failure.
This study has several limitations. Firstly, with the design of non-interventional surveillance, we could not obtain the information beyond the information that investigator collected and presented. As we could not follow up with the serial HIV RNA level or CD4+ T cell count with ongoing treatment, the consistency of effectiveness analysis including HIV RNA and CD4+T cell counts could not be attained. We also could not collect actual laboratory result such as serum creatinine, or vital sign such as body temperature and patients' adherence. Secondly, to include enough subjects to report in restricted surveillance period, subjects who have already commenced Kivexa before the study period were included along with Kivexa naïve patients, which might be a reason for some loss of acute adverse events. Finally, a sample size of 600 patients may not be large enough to detect rare adverse events.
In conclusion, we present the result of surveillance of Kivexa use in Korean HIV-positive population. Kivexa was generally well tolerated and the incidence of adverse drug reaction was substantially low. There were no cardiovascular adverse events related to Kivexa in this population and ABC hypersensitivity was rare. Similar to the PMS results of other antiretroviral agents, the safety results must be interpreted comprehensively since Kivexa was administrated other antiretrovirals. The results were similar to the PMS results of single components of Kivexa, and there was no significant new safety information [13]. Kivexa is still widely used by itself as a backbone, and its components abacavir and lamivudine is also available as a fixed dosed combination tablet with dolutegravir in Korea. This data may be helpful to understand the safety profile of lamivudine/abacavir containing regimens in Korea.
 XML Download
XML Download