

 PDF
PDF ePub
ePub Citation
Citation Print
Print



POEMS syndrome is a rare paraneoplastic syndrome caused by plasma cell (PC) neoplasm, characterized by polyneuropathy, organomegaly, endocrinopathy, M-protein, and skin changes. Other important clinical features include papilledema, extravascular volume overload, sclerotic bone lesions, Castleman disease, thrombocytosis/erythrocytosis, elevated vascular endothelial growth factor (VEGF) levels, thrombotic diatheses, and abnormal pulmonary function tests [1]. This disease comprises 1–2% of PC dyscrasias [2]. Although the pathogenesis is unclear, disease activity may be related to increased VEGF levels [3].
Its diagnosis is challenging because this is a rare disease and the clinical presentation may be complex. This disease can be misdiagnosed as chronic inflammatory demyelinating polyradiculoneuropathy, monoclonal gammopathy of undetermined significance (MGUS), or neuropathy and immunoglobulin light chain amyloid neuropathy [45]. Correct diagnosis is important because the treatment regimens differ for these diseases, which can be critical for patient outcomes [6]. Although the characteristic bone marrow (BM) findings of POEMS have not been established, a recent study has reported PC rimming around lymphoid aggregates and megakaryocytic hyperplasia in BM biopsies of patients with POEMS syndrome [7]. We attempted to identify the key clinical features and characteristic BM findings of POEMS syndrome. To the best of our knowledge, this is the first comprehensive report on clinical and BM findings for such patients in Korea. This study was approved by the Institutional Review Board of Asan Medical Center, Seoul, Korea (IRB-2015-0328).
We retrospectively reviewed the medical records and BM analyses of 24 patients diagnosed as having POEMS syndrome at Asan Medical Center between December 2002 and July 2016. Their median age was 55 (range: 24–84) years, and the male-to-female ratio was 1.3:1. Clinical factors, such as polyneuropathy (peripheral and sensory or sensorimotor), extravascular volume overload (edema, ascites, or pleural effusion), organomegaly (lymphadenopathy, splenomegaly, or hepatomegaly), endocrinopathy (hypothyroidism, adrenal insufficiency, diabetes mellitus, or hypogonadism), skin changes (hyperpigmentation or hypertrichosis), and associated laboratory and imaging analyses findings were extracted from the medical records and analyzed considering the diagnostic criteria of POEMS syndrome [1]. Four patients who lacked data such as X-ray scans were included because they were highly suspicious of POEMS syndrome clinically.
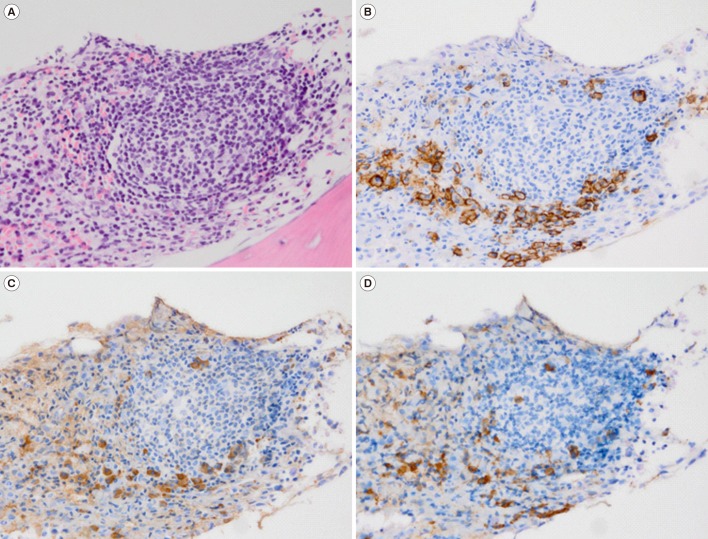
BM analysis included peripheral blood smear, BM aspirate smear, touch print, clot section, and biopsy section. The peripheral blood smear, BM aspirate smear, and touch print were prepared by Wright-Giemsa stain, and the clot and biopsy sections were prepared by hematoxylin and eosin stain. Immunohistochemistry (IHC) stains were performed on the clot or biopsy sections using monoclonal antibodies specific for CD138, κ, and λ (DAKO, Glostrup, Denmark), according to routine protocols for automated IHC using Ventana Benchmark XT (Ventana Medical Systems, Tucson, AZ, USA). We performed additional IHC stains on the remaining BM biopsy or clot sections for patients without IHC findings and reviewed the BM analyses again. Visual detection of a monoclonal band following serum protein electrophoresis (PEP) was used to confirm the presence of monoclonal protein. The percentage of monoclonal protein was quantified using a densitometer, and the absolute concentrations of monoclonal protein (g/L) were calculated from total serum protein concentrations. The five color-flow cytometric BM aspirate findings using CD138/CD38/CD19/CD45/CD56 were included for six patients. Quantitative data were summarized as median (range) or count and percentage.
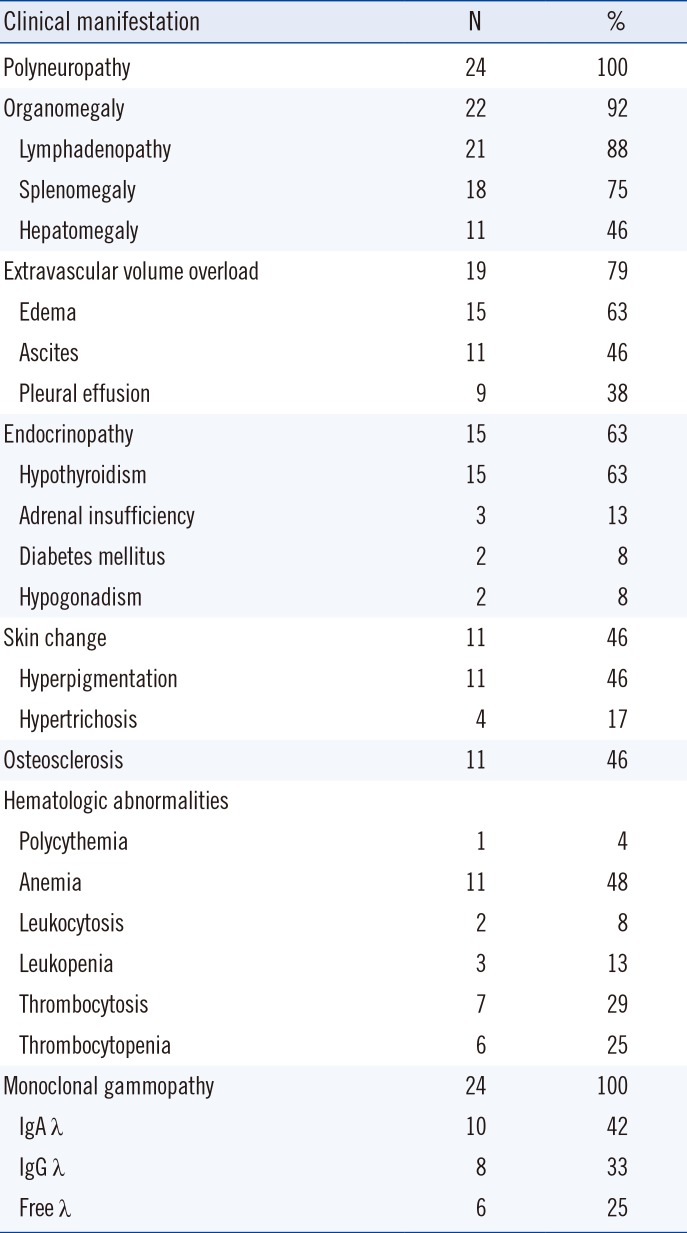
The clinical, laboratory, and BM findings are summarized in Tables 1 and 2. The most frequent clinical manifestations included polyneuropathy, monoclonal gammopathy with λ clonality, organomegaly, extravascular volume overload, endocrinopathy, skin changes, and osteosclerotic changes of the bone based on the X-ray or computed tomography scan. Anemia was the most common hematologic abnormality.
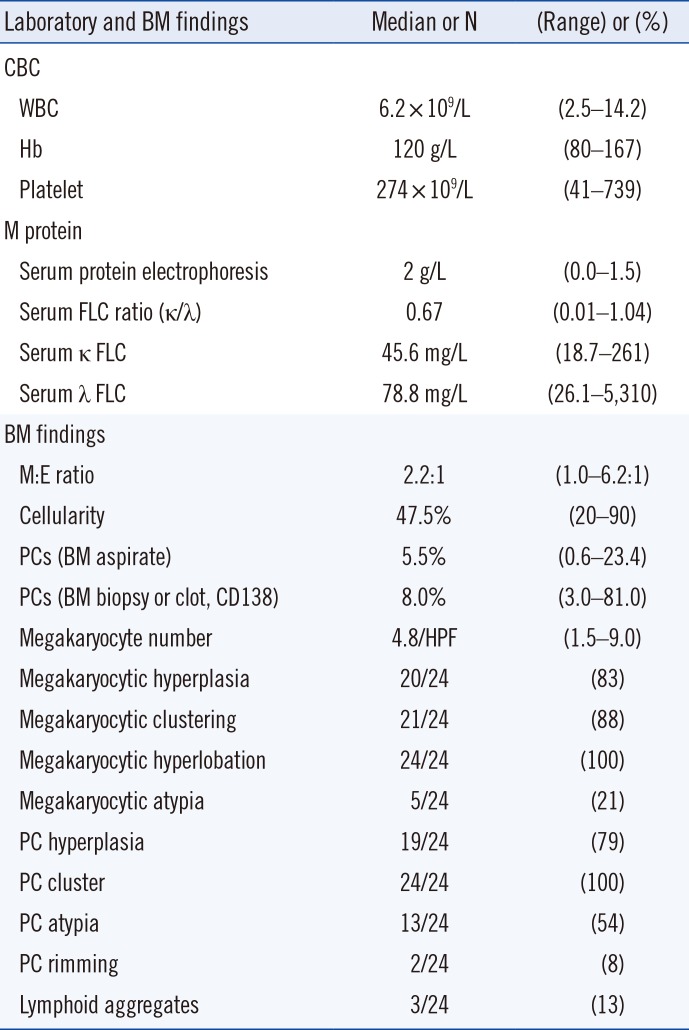
The patients showed variable complete blood counts. M-proteins on serum PEP were found in 18 patients (75%). Serum and urine immunofixation electrophoresis (IFE) revealed monoclonal gammopathy in 22 patients (IgA λ type in 10 patients, IgG λ type in eight patients, and free λ type in four patients). One of the two patients who showed no restriction in serum or urine IFE showed a λ type monoclonal band in cerebrospinal fluid immunoelectrophoresis, and the other patient showed increased serum free κ (34.8 mg/L) and λ chain (86.6 mg/L) and λ clonality in IHC of the BM biopsy. Urine PEP or IFE showed Bence-Jones proteinuria in 13 patients (54%). Serum VEGF levels were checked in four patients, with a median level of 4,070 pg/mL (3,330–6,230 pg/mL; reference range: <500 pg/mL).
In BM analyses, the median proportion of PCs was 5.5% (0.6–23.4) on BM aspirate smears and 8.0% (3.0–81.0; N=17) in the BM biopsies or clot sections (CD138). PC hyperplasia (>3% in BM nucleated cells) was found in 19 patients (79%), PC clusters (at least three PCs localized in a cluster) were found in all patients (100%), and PC atypia, such as multinucleation, was found in 13 patients (54%). Lymphoid aggregates were found in three patients (13%), and PC rimming around the lymphoid aggregate was found in two patients (8%), which did not show any restricted λ or κ clonality (Fig. 1). The myeloid:erythroid (M:E) ratio and cellularity were variable. Megakaryocytic hyperplasia (>4/high-power field [HPF]) was found in 20 patients (83%), including a slight increase (4–6/HPF) in 13 patients (54%) and an overt increase (>6/HPF) in seven patients (29%). Megakaryocyte clusters (at least three megakaryocytes localized in a cluster) were found in 21 patients (88%), megakaryocyte hyperlobation (>8 lobes in the nucleus) in all patients (100%), and megakaryocyte atypia, such as separated nuclei, in five patients (21%).
Flow cytometry of the BM aspirate from six patients revealed a neoplastic immunophenotype (CD138+/CD38+/CD19−/CD45−/CD56+) in two patients and a normal immunophenotype (CD138+/CD38+/CD19+/CD45+/CD56−) in the other four patients. The cytogenetic analyses of the BM aspirates (N=22) showed no chromosomal abnormalities, except for loss of the Y chromosome in one patient, which was probably an age-related event. A lymph node biopsy was performed in six patients:Castleman disease was found in two patients (33%), while the other patients showed reactive hyperplasia.
Management of POEMS syndrome depends on the presence of disseminated BM involvement [8]. BM analysis can be requested to evaluate the extent of POEMS syndrome, but it can also be requested when MGUS needs to be ruled out or a workup for other myeloproliferative conditions, such as erythrocytosis or thrombocytosis, needs to be conducted.
Plasmacytosis (median 5.5% in BM nucleated cells) was mild on BM aspirate smears, consistent with previous reports [79]. The PC counts on BM aspirate smears were lower than that in BM biopsies or clot sections, implying that BM aspirates can be diluted with peripheral blood during the procedure. Lymphoid aggregates (13%, 3/24) were infrequent, and PC rimming around the lymphoid aggregate was polyclonal (8%, 2/24), compared with a previous report in which approximately half of the patients showed monoclonal and polyclonal PC rimming around the lymphoid aggregates [7]. The unusual distribution of clonal PCs relative to the lymphoid aggregates may be the result of immune dysfunction or dysregulation. This finding is unique to POEMS among the PC dyscrasias; various cytokines, other than paraprotein, surrounding the clonal PCs are hypothesized to cause the characteristic distribution [31011].
VEGF appears to play a pathogenic role in this disorder by increasing vascular permeability, angiogenesis, and monocyte/macrophage migration, potentially resulting in arterial obliteration, which is responsible for several findings such as organomegaly, edema, and skin changes in patients with POEMS [10]. Platelets contain numerous proteins that regulate angiogenesis and are a major source of VEGF [12]; megakaryocytic hyperplasia might be related to increased VEGF levels.
Additional characteristic BM findings included megakaryocytic hyperlobation (100%), cluster formation (87%), and hyperplasia (83%). These findings were differentiated from myeloproliferative neoplasm (MPN) due to negative JAK2 V617F [7]. In our study, only two patients had a JAK2 analysis, and the findings were wild-type. Increased VEGF level may affect the maturation and redistribution of megakaryocytes in BM [13]. However, megakaryocytic hyperplasia did not lead to peripheral thrombocytosis in our study, as only 29% showed peripheral thrombocytosis compared with 83% with megakaryocytic hyperplasia in BM.
Our study showed 100% λ clonality, similar to the findings of Dispenzieri [8] (100%), Nakanishi, et al. [14] (95%), and Li, et al. [9] (97%). Monoclonal gammopathy is almost always restricted to λ type monoclonal protein. However, the pathognomonic relationship is yet to be elucidated.
In summary, the characteristic BM findings of POEMS syndrome are mild plasmacytosis and megakaryocytic hyperplasia, hyperlobation, and cluster formation. POEMS syndrome should be considered when a BM analysis is requested for a patient showing clinical symptoms with monoclonal gammopathy.
 XML Download
XML Download