

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Streptococcus pneumoniae is an important human pathogen that causes pneumonia, sepsis, and meningitis, especially in children [123]. This bacterium has more than 93 serotypes, but only a few cause the majority of pneumonias and invasive pneumococcal diseases (IPDs). The serotype distribution differs by patients' age, geographic region, and time of surveillance; these changes are affected by vaccination trends [45].
Following the introduction of the 7-valent pneumococcal conjugate vaccine (PCV7, targeting serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F) in children, IPDs caused by PCV7 serotypes decreased dramatically in many countries [678910]. However, the use of PCV7 led to an increase in infections with non-vaccine serotypes such as 19A [8111213]. PCV7 has led to extensive changes in serotype distribution in Korea [1415]. Since 2010, PCV10 (includes PCV7 plus serotypes 1, 5, and 7F) and PCV13 (includes PCV10 plus serotypes 3, 6A, and 19A) have replaced PCV7 in Korea; national immunization programs (NIPs) have been provided for children since May 2014. Therefore, a survey of serotype distribution is necessary for the design of national strategies following the change in the type of pneumococcal vaccine used.
High rates of drug resistance and the spread of multi-drug resistant (MDR) strains of S. pneumoniae constitute serious public health concerns worldwide [1415]. In Korea, high resistance against most antimicrobial agents continues to be observed in pneumococcal diseases [1617], although the resistance rate to penicillin has decreased since the change in the CLSI breakpoints [18]. We aimed to investigate the serotype distribution and antimicrobial resistance of S. pneumoniae isolated between 2014 and 2016 in Korea.
Go to : 
METHODS
Clinical isolates
A total of 1,855 S. pneumoniae isolates were prospectively collected from 44 hospitals in Korea between May 2014 and May 2016. All isolates were transported to the Inje University Busan Paik Hospital, Busan, Korea and stored until use at −70℃ using 10% skim milk. This study was approved by the Institutional Review Board of Inje University Busan Paik Hospital (No. 14-0256).
Serotyping by sequential multiplex PCR assay
The serotype of all pneumococcal isolates was determined using sequential multiplex PCR (SM-PCR) according to the recommendations of the U.S. Centers for Disease Control and Prevention (CDC) [19]. For DNA extraction, colonies cultured on blood agar plates were mixed with 200 µL of Tris-EDTA buffer solution (Sigma-Aldrich Co., St Louis, MO, USA). This mixture was heated at 100℃ for 10 minutes and then promptly placed on a frozen surface (−20℃) for 5 minutes, followed by centrifugation at 13,000 rpm. SM-PCR was performed with a PCR premix (AccuPower PCR PreMix, Bioneer Inc., Daejeon, Korea), 1 µL of each primer, 5 µL of DNA template, and distilled water in a final volume of 20 µL. Thermal cycling was conducted in a Veriti96-well thermal cycler (Applied Biosystems, Foster City, CA, USA) under the following conditions: 94℃ for 5 minutes; 30 amplification cycles of 94℃ for 30 seconds, 54℃ for 30 seconds, and 72℃ for 30 seconds; and one cycle of 72℃ for 7 minutes. The size of the amplification products was confirmed by electrophoresis on a 2% agarose gel. The Quellung reaction was additionally performed to differentiate serotype 6A from other serotype 6 subtypes using factor antisera (Statens Serum Institute, Copenhagen, Denmark).
Collection of antimicrobial resistance data
The drug resistant results of the pneumococcal isolates were collected from the participating hospitals; the assays were performed mainly by Microscan (Siemens Healthcare Diagnostics, Sacramento, CA, USA), the VITEK2 system (bioMérieux, Marcy-l'Étoile, France), and E-test (bioMérieux). The results were interpreted according to the CLSI guidelines [20]. Separate interpretive breakpoints were used to define the resistance of meningeal isolates to penicillin, cefotaxime, and ceftriaxone. An isolate resistant to three or more classes of antimicrobial agents was considered MDR. We analyzed serotype prevalence by age group, clinical source, and antimicrobial resistance.
Go to :
RESULTS
Characteristics of S. pneumoniae isolates
Of the 1,855 isolates, 1,286 (69.3%) were from male patients and 438 (23.6%) were from patients with invasive disease. The most common source of invasive isolates was blood (N=372; 84.9%), followed by cerebrospinal fluid (N=21; 4.8%), pleural fluid (N=13; 3.0%), abscess (N=13; 3.0%), tissue (N=8, 1.8%), and others (N=11; 2.5%). Non-invasive isolates were recovered from respiratory specimens (N=1,253; 88.4%), wounds (N=127; 9.0%), catheter tips (N=16; 1.1%), urine (N=8; 0.6%), and other sites (N=13; 0.9%).
Distribution of pneumococcal serotypes
The most common serotype was 11A (10.1%), followed by 19A (8.8%), 3 (8.5%), 34 (8.1%), 23A (7.3%), 35B (6.2%), and 15A (5.1%); these serotypes accounted for 54.2% of the isolates (Table 1). Serotypes 23A, 15B, 19A, and 10A were more common in patients ≤5 years old (18.1%, 12.5%, 12.1%, and 8.1%, respectively). In contrast, serotypes 11A, 3, and 34 were much less common in patients ≤5 years old. The frequency of the major serotypes was very similar in patients ≥65 and 6–64 years old. The number of serotypes recovered from ≥65 years and 6–64 years age groups was 35 and 32, respectively, whereas only 20 serotypes were recovered from patients ≤5 years old. Non-typeable (NT) isolates that were not detected by SM-PCR accounted for 6.3% (N=117) of all isolates. These organisms were more common in children ≤5 years old (10.5%).
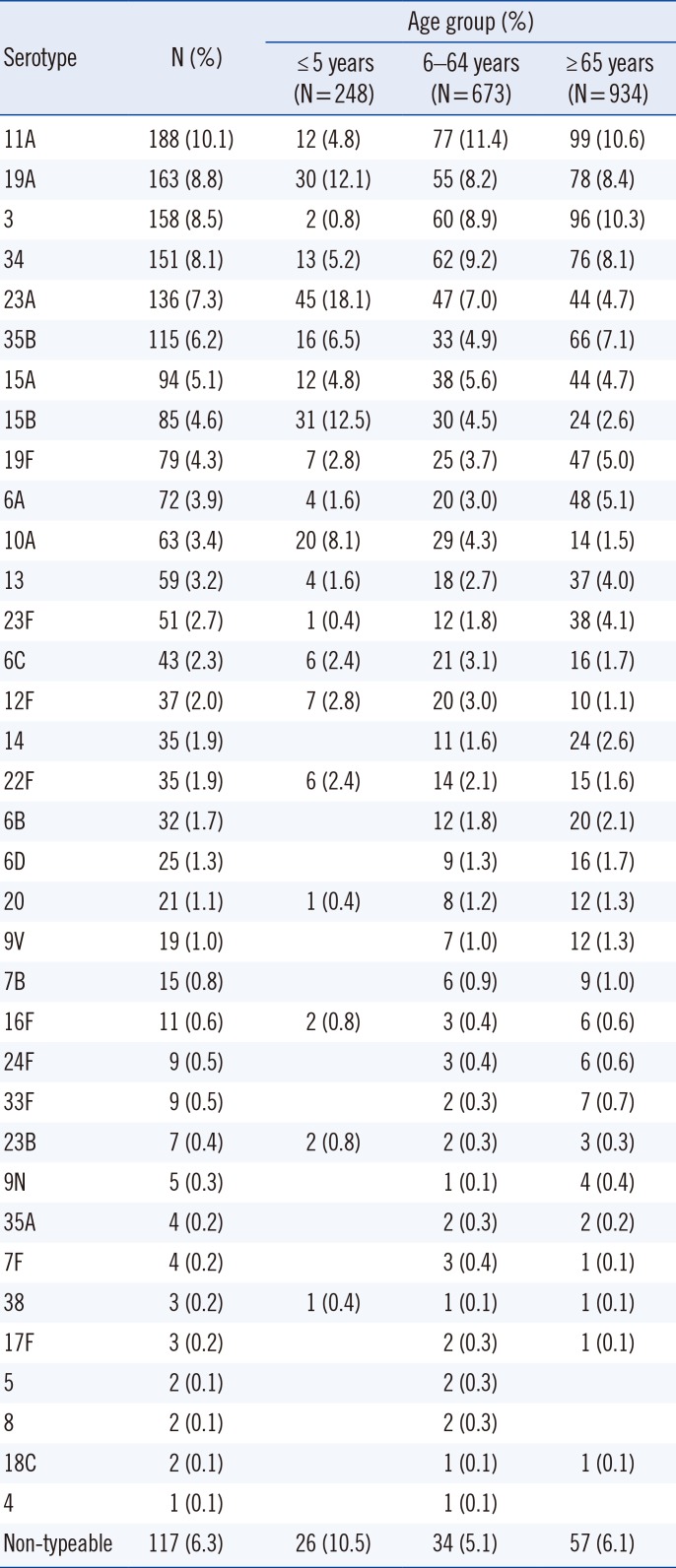
Table 1
Distribution of pneumococcal serotypes by patient age (N=1,855)
![]()
The most common serotype among the invasive isolates was 3 (12.6%), followed by 19A (7.8%), 34 (7.8%), 11A (6.8%), 10A (6.8%), and 12F (6.6%) (Table 2). However, serotypes 3, 10A, and 12F were more prevalent among invasive than noninvasive isolates (7.3%, 2.3%, and 0.6%, respectively). Serotypes 11A, 23A, and 35B were more common among noninvasive isolates (11.2%, 8.2%, and 7.0%, respectively) than invasive isolates (6.8%, 4.6%, and 3.7%).
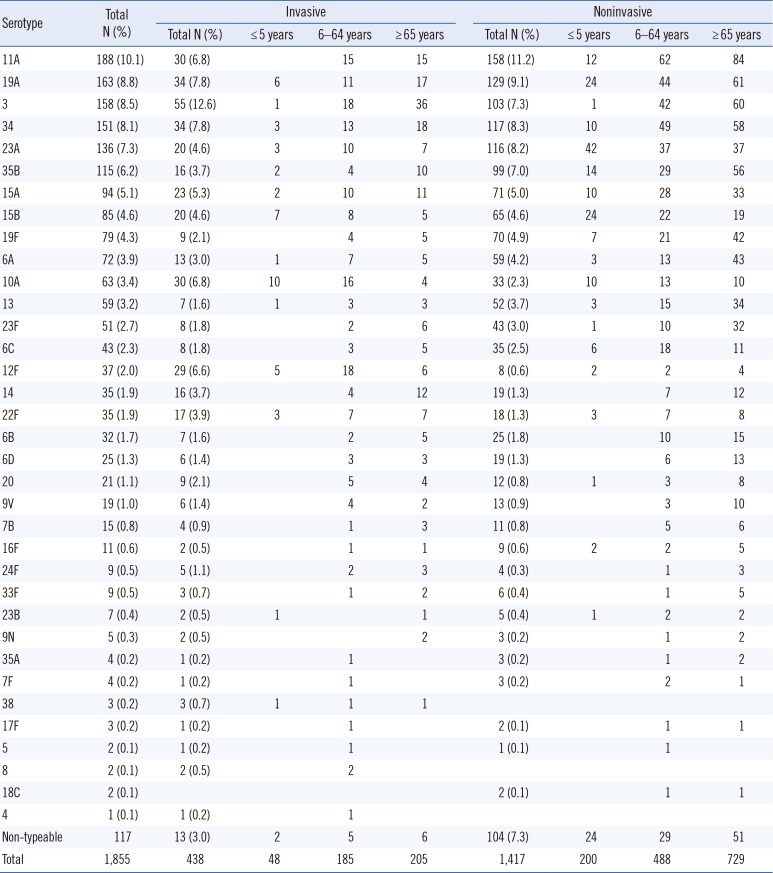
Table 2
Comparison of invasive and noninvasive serotypes by patient age
![]()
Serotypes 10A (20.8%), 15B (14.6%), 19A (12.5%), and 12F (10.4%) were common in patients ≤5 years old, whereas 11A and 3 were rarely observed (0% and 2.1%, respectively). Among the invasive isolates, serotypes 11A and 3 were common in patients ≥65 years old (7.3% and 17.6%, respectively) and 6–64 years old (8.1% and 9.7%, respectively), while serotypes 10A and 12F were less frequent in patients ≥65 years old (2.0% and 2.9%, respectively) than in those ≤5 years (20.8% and 10.4%, respectively) and 6–64 years old (8.6% and 9.7%, respectively).
The coverage rates for PCV7, PCV10, PCV13, pneumococcal polysaccharide vaccine 23 (PPSV23), and vaccine serotype (VT) were 11.8%, 12.1%, 33.3%, 53.6%, and 57.5%, respectively (Table 3). For invasive isolates, the coverage rates of PCV7, PCV10, PCV13, PPSV23, and VTs were 10.7%, 11.2%, 34.5%, 64.2%, and 67.1%, respectively. By age, the coverage rates of PCV7, PCV10, and PCV13 among the invasive isolates were 0%, 0%, and 16.7% in children ≤5 years old and 14.6%, 14.6%, and 42.9% in patients ≥65 years old.
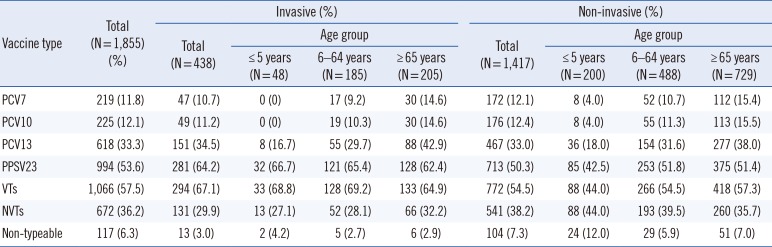
Table 3
Prevalence of vaccine serotypes by patient age, specimen type, and period
![]()
Antimicrobial resistance
The antimicrobial resistance of the S. pneumoniae isolates is shown in Tables 4 and 5. The resistance rates against penicillin, cefotaxime and levofloxacin were 22.8%, 12.5% and 9.4%, respectively. Among the invasive isolates, the resistance rates against cefotaxime, ceftriaxone, and levofloxacin were higher in patients ≥65 years old (7.5%, 5.2%, and 4.9%, respectively) than in patients ≤5 years old (2.6%, 0%, and 0%, respectively).
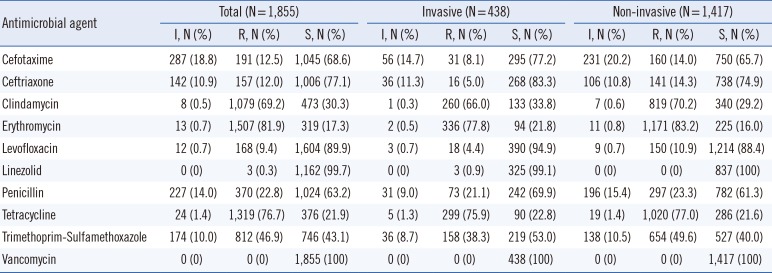
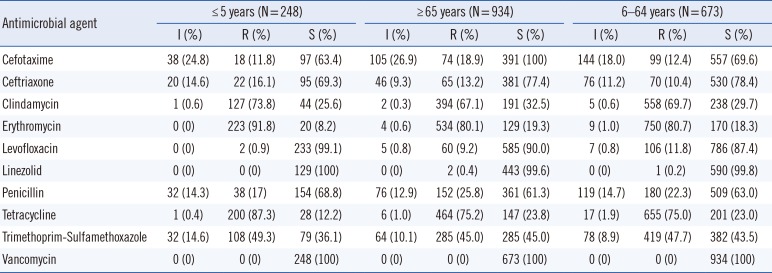
Table 4
Resistance to antimicrobial agents by specimen type
![]()
Table 5
Resistance to antimicrobial agents by patient age
![]()
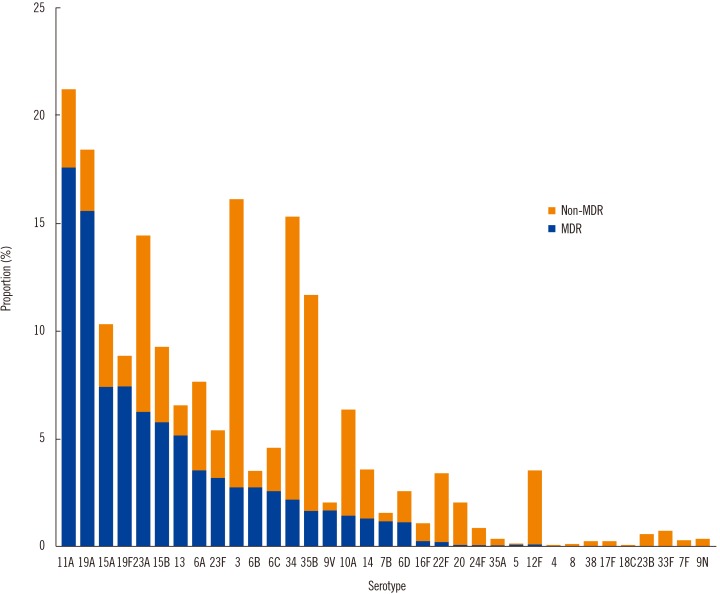
Of the 1,855 isolates, 857 (46.2%) were MDR, including 11A (17.7%), 19A (15.8%), 19F (7.6%), and 15A (7.6%) (Fig. 1). The proportion of MDR was extremely high in serotypes 11A (80.9%), 19A (82.8%), 19F (82.3%), 13 (78.0%), 6B (78.1%), 9V (84.2%), and 7B (80.0%). Serotypes 3, 34, and 6A expressed low-level resistance.
Go to :
DISCUSSION
The prevalence of the common serotypes differed from that in our previous report [16]. Compared with the results from 2011 to 2014, the proportion of non-PCV13 serotypes, such as 11A, 23A, and 15A, remarkably increased. In addition, we confirmed that serotypes 3 and 6A are now less common, whereas there was no change in the prevalence rate of serotype 19A.
The coverage of PCV13 had decreased, whereas the coverage of PPSV23 had not changed since our previous results from 2011 to 2014 [16]. Surprisingly, the coverage rate of the PCV13 serotype among the invasive isolates was much lower in patients ≤5 years old (16.7%) than in the other age groups (6–64 years old [29.7%] and ≥65 years old [42.9%]). We hypothesize that this change resulted from PCV13 use in children ≤5 years old as the NIPs with PCV13 were provided only for children. In addition, this is associated with the high prevalence of serotype 3 in patients ≥65 years old. The 2014 Korean guidelines recommend the administration of PPSV23 or PCV13 to individuals ≥65 years old [21].
Richter, et al. [22] reported a decrease in the prevalence of the PCV13 serotypes in all isolates in the United States from 43.4% (2008–2009) to 27.1% (2012–2013) after the introduction of the PCV13 vaccine. In addition, the prevalence of non-PCV serotypes, such as 11A and 35B, increased among all isolates, while that of serotype 3 slightly increased. Interestingly, they observed a decrease in the prevalence of serotype 19A from 22% to 10% of all isolates, which differs from our results. However, Richter, et al. [23] reported that serotype 19A had not changed between 2010 and 2011. Therefore, we hypothesize that serotype 19A will shortly decrease in Korea. Galanis, et al. [24] and van der Linden, et al. [25] reported an increase in non-PCV13 serotypes in IPD. We confirmed the increase in non-PCV13 serotypes such as 11A, 23A, and 15A; however, there was no observed increase in serotype 23B. Thus, there is a need for a new pneumococcal vaccine, including non-PCV13 serotypes, to prevent IPDs in children.
Previously, we reported the resistance rate against penicillin as 9.0% from 2008 to 2014 [16] and 10.8% from four university hospitals in Busan and Gyeongnam in 2015 [17]. In this study, the resistance rate against penicillin among the isolates from 44 hospitals was 22.8%; thus, there was a striking tendency towards an increase in penicillin resistance. The resistance rates against cefotaxime, ceftriaxone, and levofloxacin were 12.5%, 12.0%, and 9.4%, respectively, which again are higher than those in a previous report [16]. Our findings suggest that resistance rates are increasing in Korea and elsewhere, highlighting the need to monitor antimicrobial resistance continually.
There was a strong association between serotype and antimicrobial resistance. The proportion of MDR S. pneumoniae was extremely high among serotypes 11A, 19A, 19F, 13, 6B, 9V, and 7B. Interestingly, the resistance rate against levofloxacin was quite low in serotypes 19A and 23A. Thus, serotypes showing high resistance should be controlled to diminish the risk of severe, even fatal, diseases caused by this organism.
Go to :
 XML Download
XML Download