

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The diagnosis of gestational diabetes mellitus (GDM) is not yet completely and universally resolved. Despite the latest attempt to universalize diagnostic criteria by the International Association of Diabetes and Pregnancy Study Groups (IADPSG) [1], with the support of the Hyperglycemia and Adverse Pregnancy Outcomes (HAPO) study [2], a consensus has not yet been reached. A systematic review carried out by the Cochrane Library concluded that there is not enough evidence to recommend any strategy universally, and that each one should be applied according to the risks of the population to be treated [3].
In many countries, a two-step strategy is used following the American Diabetes Association (ADA) [4] and American College of Obstetrician and Gynecologists (ACOG) criteria [5]. The strategy begins with universal screening based on the glucose challenge test (GCT), followed by an oral glucose tolerance test (OGTT) of 100 g and four blood extractions for pregnant women with a GCT value ≥140 mg/dL.
The performance of the OGTT as a diagnostic test is very high; however, the sensitivity (S) of the GCT ranges between 70% and 88% for the 140 mg/dL cut-off point [6]. In addition, the reproducibility of the OGTT is low [7], especially when compared with that of other biomarkers such as glycated Hb (HbA1c) [8]. Furthermore, it is an important source of expense for laboratories and causes great inconvenience to pregnant women, as they must spend at least one hour in the hospital for the GCT. In addition, the test itself causes discomfort and is frequently associated with nausea and vomiting [3]. Researchers have looked for other parameters that can be tested so as to replace the GCT or at least reduce the number of pregnant women subjected to the GCT. One possible biomarker, HbA1c, is currently used as a fundamental parameter for the diagnosis and monitoring of diabetes mellitus [1011].
However, the dilutional anemia associated with pregnancy and the reduction in the half-life of red blood cells (also characteristic of pregnancy) have prevented the extension of HbA1c reference ranges from non-pregnant to pregnant women. Nevertheless, many HbA1c characteristics could make it a very useful biomarker of GDM. For example, it has a clear correlation with average glycemia during the three to four months prior to measurement; it is standardized and has great precision andreliability; its determination is routine in most clinical laboratories; and the procedure is very simple for the patient, without the need to fast.
Research supports the use of HbA1c as a biomarker of GDM. The United States Preventive Service Task Forces commissioned a systematic review [6] that included four studies proposing the use of HbA1c as a screening test for GDM. The HAPO study also established a statistically significant relationship between HbA1c and a series of pregnancy complications [11]. However, the evidence is still insufficient, and clinical guidelines have not incorporated HbA1c in relation to GDM, except as a marker of pre-gestational diabetes [4]. We provide new results that support the use of HbA1c as a screening and diagnostic tool for GDM. To the best of our knowledge, this is the first study to examine the use of HbA1c as a screening test in the context of the National Diabetes Data Group (NDDG) strategy [12].
METHODS
Study design and population
This retrospectivecase-control study was conducted between December 1, 2016 and May 20, 2017. We randomly selected 607 pregnant women who attended Macarena University Hospital, Sevilla, Spain, for the GCT. We excluded those who were not between the 24th and the 28th week of gestation and those with a history of diabetes and other pathologies that could interfere with HbA1c determination, such as hemoglobinopathies. Our study was approved by the Research Ethics Committee of the Virgen del Rocío and Virgen Macarena University Hospitals, Seville, Spain (code: PFR-DG-2017-01).
HbA1c measurement
Whole blood samples (5 mL EDTA tubes) were collected from pregnant women at the same time as that for GCT blood extraction. HbA1c was determined in fresh samples, using G8 (Tosoh Corporation, Shiba-Mianto-ku, Tokyo, Japan), an HPLC ion exchange, preceded by a pre-filter to avoid the rapid deterioration of the column, with a detection system comprising a photometer that quantifies the different Hb fractions identified by their specific retention times.
The instrument was calibrated according to the manufacturer's specifications, and we performed daily controls with the two internal controls provided by the manufacturer and three levels of the Liquichek Diabetes Control, provided by Bio-Rad (Irvine, CA) and prepared from whole human blood, as an external quality control. Instrument precision is CV=0.65% [13]. It is certified by the National Glycohemoglobin Standardization Program. The GCT values were obtained for all participants, and the OGTT value was measured in participants with a GCT value ≥140 mg/dL, using the Advia 2400 glucose hexokinasemethod (Siemens Healthineers, Erlangen, Germany), calibrated according to the manufacturer's specifications. We performed a daily controlon glucose hexokinase method with two levels of the internal control provided by the manufacturer and an external control provided by the Spanish Society of Clinical Medicine.
GDM diagnosis
We diagnosed GDM following the recommendations of the Spanish Group of Diabetes and Pregnancy [14]; GDM screening is performed for all pregnant women. The screen consists of 50 g of GCT followed by 100 g of OGTT when GCT glycemia is ≥140 mg/dL. The 100 g OGTT follows the recommendations and cut-off points detailed by the NDDG for diagnosing GDM when two or more measures are equal to or greater than the following cut-offs: fasting, 105 mg/dL; 1 hour, 190 mg/dL; 2 hours, 165 mg/dL; and 3 hours, 145 mg/dL [12].
Statistical analysis and diagnostic performance
The Kolmogorov-Smirnov was used to determine the normal distribution of the data. Participants were divided into two groups: normal and GDM. The mean and SD were calculated for HbA1c, GCT, body mass index (BMI), and age. We determined meandifferences with 95% confidence interval (CI) for these parameters between the two groups. The Student's t-test was used to compare mean HbA1c between groups.
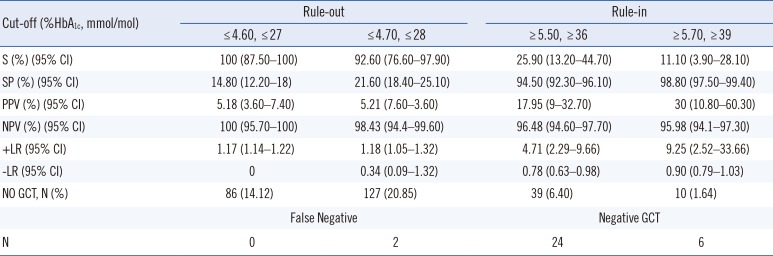
The ROC curve was constructed, and the area under the ROC curve (AUC) with 95% CI was determined. S, specificity (SP), positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (+LR), and negative likelihood ratio (−LR) were calculated with 95% CI for four cut-off points, two of which maximize S and two that maximize SP, using IBM SPSS20 (IBM Corp., Armonk, NY, USA).
Assuming a diagnostic strategy in which HbA1c was used as a screening test to avoid the GCT in pregnant women at low risk of GDM (below the lower cut-off), or to perform the confirmatory OGTT in those at high risk (above the higher cut-off) without a previous GCT, we calculated the percentage of participants who would avoid the GCT. In addition, we calculated the false negatives that would occur using the low cut-off points and the negative GCTs that would correspond to the high cut-off points.
RESULTS
HbA1c level, GCT value, age, and BMI were normally distributed.Of 607 participants, 580 formed the normal group (mean age= 31.9±5.8 years, mean BMI=27.2±4.9 kg/m2, and mean GCT value=115.3±27.8 mg/dL). The GDM group included 27 participants (5.4%; mean age=33.2±4.4 years, mean BMI=29.5±6.9 kg/m2, and mean GCT value=185.6±33.7 mg/dL). As shown in Table 1, HbA1c level differed significantly between groups but age and BMI did not.
Table 2 shows the cut-off points for HbA1c based on the ROC curve. Choosing 4.6% HbA1c (27 mmol/mol) as a low cut-off prevented false negatives in the study population and decreased the number of GCTs performed (86 pregnant women were identified as low-risk) by 14.1%. Using 4.7% HbA1c (28 mmol/mol) as the low threshold resulted in two false negatives and a reduction of 20.8% in the number of GCTs (127 pregnant women who do not require a GCT). In terms of the high thresholds, 6.4% of pregnant women would directly proceed to a confirmatory OGTT.
DISCUSSION
We proposed inclusion of HbA1c in GDM diagnostic strategy, which can reduce the number of pregnant women subjected to the GCT. Our results confirm that mean HbA1c levels were lower in the normalgroup,similar to previous results [1624]. Although the difference in HbA1c level between groups is smaller than the difference in the mean GCT value between groups (70.26 mg/dL; Table 1), these parameters reflect two different, although related, situations. The GCT value is an indicator of altered postprandial glycemia that begins during the third trimester in GDM, while HbA1c level indicates an increase in average glycemia, which begins weeks before in GDM [15]. We believe that both parameters can be useful in GDM diagnostic strategies.
The incidence of GDM in our study population (5.4%, Table 1) is similar to the 5% GDM incidence reported for Andalucia, our region [17]. Thus, our population (and region) can be considered at low-risk for GDM. Universal screening based on the GCT or other OGTTs is excessive, especially in low-risk populations; the characteristics of each population should be studied and the diagnostic strategy should be adapted according to the incidence [3412].
We propose a low threshold determined between the 24th and 28th gestational weeks as a screening test prior to the GCT. These low threshold results are promising; a simple, cheap, and non-aggressive test, such as for HbA1c, could lead to a 14% reduction in the number of women subjected to the GCT, with no false negatives, or a 21% reduction with only two false negatives. The low performance at the high cut-off could be explained in part by the fact that our participants are from a low-risk population. Another important reason is that according to the protocol of our region, pregnant women undergo high-risk screening during the first trimester [20]. Thus, many high-risk pregnant women had already been detected before the 24th week when we recruited our population. In addition, of the 39 participants who would have avoided the GCT, 24 had a negative GCT result. However, it is important to remember that S of the GCT using 140 mg/dL as the cut-off is between 70% and 88% [6]; consequently, some of these negative GCT results could be false negatives.
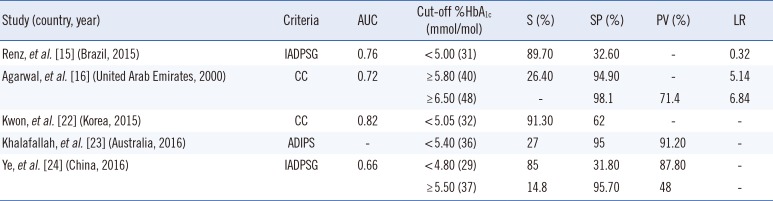
Similar results were reported by one of the few studies that followed diagnostic criteria comparable to ours (two-step strategy, GCT+OGTT). Agarwal, et al. [16] analyzed a high-risk population from the United Arab Emirates following the Carpenter and Coustan criteria [21], which are more inclusive than those of the NDDG [12]. However, the results are quite similar (Table 3). A notable difference is that our study identified only two false negatives (in 607 participants) when using the mentioned cut-off, while Agarwal, et al. [16] reported nine false negatives (in 426 participants).
More recently, Kwon, et al. [22] published a similar study, also based on the Carpenter and Coustan criteria [21]; however, their population included 321 Korean women at risk of GDM (positive GCT). They proposed the use of HbA1c as a screening test, with an AUC=0.824 and a cut-off point of 5.1%, with S=91.3%. However, they did not report any data regarding test performance that would allow us to compare it with our results.
In recent years, especially since the publication of Lowe, et al. [11], new studies proposing the use of HbA1c as a biomarker of GDM have been emerging [1516]. These studies (diagnostic performance parameters are listed in Table 3) support our proposal of HbA1c as a useful tool in the diagnosis of GDM. All of these studies propose screening thresholds to be used in an attempt to reduce the number of GCTs or OGTTs by identifying GDM in high-risk populations or using the more inclusive IADPSG criteria [1]; thus, they used lower Sthan our study, which aimed at identifying GDM in low-risk women.
When comparing our work with the aforementioned ones, Ye, et al. [24] reported an AUC of 0.66, similar to our AUC (0.68); however, the value proposed by Renz, et al. [15] (AUC=0.757) is somewhat higher (Table 3).
The HbA1c cut-off points chosen for all these studies, with the exception of Ye, et al. [24], are always higher than the levels in our population. This could be explained by ethnic differences in Hb glycosylation [25] but also because of our higher level S.
A possible limitation of our study is that it was carried out in the context of a two-step diagnostic strategy. This strategy follows national and international recommendations (Spanish Group of Diabetes and Pregnancy [14], ADA [4], ACOG [5]); however, a significant number of pregnant women in our population have been subjected to only a GCT. Asthe GCT has S between 70% and 88% with cut-off point of 140 mg/dL [6], some of these pregnant women could have had false negatives, a situation that we cannot control and is beyond the objectives of this study.
In a low-risk population, it is difficult to justify subjecting all pregnant women to a test as unpleasant and costly as the GCT. We provide an alternative for 14% of pregnant women, identified as at low risk of GDM, for whom the GCT could be avoided by measuring HbA1c, a routine marker.

 XML Download
XML Download