

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The worldwide incidence of triplet pregnancies has increased considerably over the last 30 years [12]. There is no doubt that this increase in triplet births has been the result of a growing utilization of assisted reproductive technology (ART) and an increasing tendency for women to delay childbearing [23]. Although the birth rate has been decreasing annually in Korea, the rate of multiple pregnancy has increased with the advancement of ART [456]. Recent data in Korea have indicated a current multiple pregnancy rate of 32.9 per 1,000 live births in 2013 [7]. As in many other industrialized nations, the birth rate of triplets and higher-order multiples in Korea has exhibited a four-fold increase from 0.15 per 1,000 live births in 2003 to 0.59 per 1,000 live births in 2013 [7].
Triplet pregnancies are associated with increased risks of maternal complications, such as pregnancy-associated hypertension and gestational diabetes mellitus (GDM), and neonatal complications, which are mostly associated with preterm births [89]. Efforts are being made to reduce the complications associated with preterm births. Advances in perinatal care, including tocolytics, antenatal corticosteroids, and postnatal surfactant administration, have decreased the rate of neonatal morbidity for preterm births [10]. Some studies have shown that a complete course of an antenatal corticosteroid is associated with decreased risks of respiratory distress syndrome (RDS) and severe intraventricular hemorrhage (IVH) in triplet pregnancies [1112]. New tocolytics, such as atosiban, have also been added to traditional betamimetics and magnesium sulfate. However, only a few studies have addressed changes in the perinatal outcomes of triplet pregnancies, and these studies have shown inconsistent results [131415].
In ART pregnancies, selective fetal reduction (SFR) can be considered in some triplet pregnancies to improve neonatal outcomes by reducing the rates of early preterm births [1617]. Considering the medical and ethical issues of SFR, the importance of providing accurate information on the most recent outcomes of triplet pregnancies cannot be overestimated. In this context, we considered it necessary to compare previous and the most recent outcomes of triplet pregnancies in Korea and to analyze the associated factors.
Materials and methods
This study retrospectively reviewed a total of 65 consecutive triplet pregnancies delivered at the two largest tertiary-care hospitals in Korea: the Asan Medical Center (AMC) and the Samsung Medical Center (SMC), from January 1992 to December 2012, with each center providing Institutional Review Board approval (approval number: 20160024).
Women who delivered before 20 weeks of gestation or those with the death of one or more of the fetuses before 20 weeks, were excluded from the cohort of triplet pregnancies. Neonates with reduced viability who were born before 23 weeks, those with major congenital anomalies, and those who experienced in utero fetal death were also excluded from the analysis of neonatal morbidity.
The admission, discharge, and outpatient records of pregnant women and neonates were evaluated. All information was reviewed by two of the authors. This 21-year study was divided into two periods: 1992 to 2001 (period I) and 2003 to 2012 (period II). There were no triplet births at either hospital in 2002. We evaluated the temporal trends in the maternal and neonatal outcomes of triplet pregnancies.
We followed the management guidelines presented by the American College of Obstetricians and Gynecologists for all triplets [1819]. Management policies for triplet pregnancies have varied over time, and hospitalization for bed rest, prophylactic cerclage, and prophylactic tocolytics have not been generally proposed. Tocolytics were administered if clinically indicated and included one or more of the following: ritodrine, magnesium sulfate (MgSO4), nifedipine, or atosiban. Betamimetics or MgSO4 were used as first-line agents. A dose of corticosteroids was administered between 23 and 34 weeks of gestation only in expectant mothers in whom preterm birth was highly probable. The delivery was mainly by elective cesarean section after 34 weeks.
We evaluated the maternal age, the gestational age at delivery, chorionicity, pregnancy complications of preterm labor (PTL), preterm premature rupture of membranes (PPROM), preeclampsia, GDM, the use of antenatal corticosteroids and tocolytics, and anemia during pregnancy. PTL was defined as a uterine activity causing progressive cervical changes at <37 weeks of gestation. Preeclampsia was diagnosed when hypertension at ≥140/90 mmHg appeared after 20 weeks of gestation and was accompanied by proteinuria (defined as urinary excretion of ≥300 mg of protein in 24 hours or a urine dipstick value of 1+ or more). Screening for GDM in all triplet pregnancies was carried out between 24 and 28 weeks of gestation by measuring plasma glucose levels with the 50 g oral glucose tolerance test. A 1-hour post screening value of >140 mg/dL was considered positive. A diagnosis of GDM was based on the recommendations of the fourth International Work Shop Conference on Gestational Diabetes, which utilizes the Carpenter-Coustan criteria [20]. Anemia during pregnancy was defined as hemoglobin concentrations from just before delivery: <10.5 g/dL in the second trimester of pregnancy or <11.0 g/dL in the third trimester [21].
The neonatal data included birth weight, length of hospitalization, Apgar scores, and the presence of RDS, bronchopulmonary dysplasia (BPD), retinopathy of prematurity (ROP), neonatal sepsis, severe IVH, and necrotizing enterocolitis (NEC). RDS was diagnosed based on the combination of clinical (tachypnea, grunting respirations, costal retraction, and cyanosis despite 40% oxygen therapy) and radiological (a diffuse reticulogranular pattern with air bronchogram) features [22]. BPD was defined as a condition requiring treatment with oxygen after 28 days or continuous oxygen dependence at a corrected gestational age of 36 weeks [23]. Grade III–IV IVH was considered as severe IVH. Grade III involved IVH occupying more than 50% of the ventricular area, and grade IV involved periventricular hemorrhagic infarction of adjacent white matter [24]. ROP was diagnosed according to the guidelines of the International Committee for the Classification of ROP [25]. NEC was diagnosed based on clinical symptoms and radiographic pneumatosis intestinalis based on Bell's staging criteria [26]. Both suspected sepsis and proven sepsis were included. Suspected sepsis was diagnosed when the blood test findings, such as the total leukocyte count, immature total neutrophils, platelet count, and C-reactive protein were abnormal and accompanied by clinical features of sepsis without identified bacteria. Proven sepsis was diagnosed with identified bacteria. The composite neonatal morbidity was defined as any of the four chronic neonatal morbidities: BPD, severe IVH, NEC, and ROP. Neonatal and infant mortality were excluded from the composite outcomes because all of the mortality cases had more than one morbidity factor.
For the descriptive statistical analysis, categorical variables are presented as numbers (percentages) and were compared using the χ2 test and Fisher's exact test. Continuous variables are expressed as the mean and were compared using the Student's unpaired t-test or the Mann-Whitney U test. Differences between the two period groups (1992 to 2001 and 2003 to 2012) regarding composite neonatal morbidity were assessed with a generalized estimating equation (GEE) logistic regression, which accounts for the cluster effects. Variables with P-values ≤0.2 in the univariate analyses were included in a multivariable GEE logistic regression model. The final model for the composite neonatal morbidity was determined by backward stepwise elimination procedures. A value of P<0.05 was interpreted as statistically significant. SAS software, version 9.1 (SAS Institute Inc., Cary, NC, USA), was used for statistical analyses.
Results
Over the 21-year study period, a total of 65 women delivered triplets (48 women at AMC and 17 women at SMC). Overall, the mean maternal age was 31.7 years, and 51 (78.5%) of the 65 women were nulliparous. Regarding the conception method, 50 (76.9%) triplet pregnancies were conceived through ART. The majority of the triplet pregnancies (95.4%) were delivered by cesarean section. Three vaginal deliveries occurred: one due to delivery at 21 weeks of gestation, one due to the death of one fetus, and one due to precipitous labor. Chorionicity was ascertained for 80% of the triplets. Of the triplets, 56.9% (n=37) were trichorionic triamniotic, 16.9% (n=11) were dichorionic triamniotic, 6.1% (n=4) were monochorionic (3 triamniotic and 1 monoamniotic) and 20% (n=13) were of unknown chorionicity. Additionally, there were no complications resulting from the monochorionic pairs. Six cervical cerclages were performed, and indications of cervical cerclage were: a short cervical length (4 cases), an incompetent cervix (1 case), and a previous history of an incompetent cervix (1 case).
As depicted in Fig. 1, 10 out of 195 fetuses were excluded from the analysis of neonatal morbidity for the following reasons: 3 (1.5%) due to a previable gestational age (at 21 weeks of gestation); 3 (1.5%) due to intrauterine death (at 26, 27, and 28 weeks of gestation); and 4 (2.1%) due to severe congenital anomalies (two with pulmonary atresia and two with severe aortic stenosis).

Period I (1992–2001) and period II (2003–2012) comprised 22 and 43 pregnant women with triplet pregnancies, respectively. Table 1 presents the maternal characteristics of the study population for both periods. Maternal age, gestational age at delivery, chorionicity, the use of tocolytics, and the use of antenatal corticosteroids were not different between periods. Notably, the incidence of preeclampsia was markedly decreased in period II compared with period I (31.8% vs. 2.3%, P=0.002). As shown in Table 1, the incidence of anemia during pregnancy was significantly decreased in period II compared with period I.
Table 1
Maternal characteristics and outcomes of triplet pregnancies within two time periods
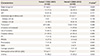
Data presented as the mean±standard deviation or number (percentage).
ART, assisted reproductive technology; PTL, preterm labor; PPROM, preterm premature rupture of membranes; GDM, gestational diabetes mellitus.
a)Categorical variables: the χ2 test or Fisher's exact test; Continuous variables: Student's unpaired t-test or the Mann-Whitney U test; P<0.05: statistically significant; b)We excluded triplets with unknown chorionicity (period I: n=12 and period II: n=1).
![]()
Table 2 summarizes the neonatal outcomes of the study population between periods I and II when analyzed with GEE logistic regression. Gestational age at delivery was not different between periods. When subdivided by gestational age at delivery as presented, there was a significant difference in each proportion between periods. The incidence of delivery under 28 weeks of gestational age was decreased, and the incidence of delivery over 34 weeks of gestational age was increased in period II compared with period I. The mean birth weight of the neonates tended to be higher in period II, but it did not reach statistical significance. Although the frequency of NICU admission did not significantly differ between periods, period II was associated with shorter hospital stays (30 vs. 18 days, P=0.001) and a lower incidence of Apgar scores below 7 at 5 minutes (23.0% vs. 5.6%, P<0.001). Although individual neonatal morbidity was not significantly different between periods, the composite neonatal morbidity was significantly decreased in period II compared with period I (26.2% vs. 8.1%, P=0.033) with neonatal and infant mortality rates of triplet neonates in periods I and II being 0% vs. 0.8% and 0% vs. 2.4%, respectively.
Table 2
Neonatal outcomes of triplet pregnancies within two time periods
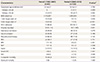
Data are presented as the mean±standard deviation, median (range), or number (percentage).
NICU, neonatal intensive care unit; RDS, respiratory distress syndrome; BPD, bronchopulmonary dysplasia; ROP, retinopathy of prematurity; IVH, intraventricular hemorrhage; NEC, necrotizing enterocolitis.
a)Categorical variables: the χ2 test or Fisher's exact test; Continuous variables: Student's unpaired t-test or the Mann-Whitney U test; P<0.05: statistically significant.
![]()
Table 3 shows maternal and neonatal characteristics of the study population according to the presence of composite neonatal morbidity, using a univariate GEE logistic regression. In this univariate analysis, the gestational age at delivery, PPROM, the neonatal hospital stay, birthweight, a 1-minute Apgar score <4, a 5-minute Apgar score <7, and the period, were found to be significantly related to the composite neonatal morbidity. When we performed multivariable GEE logistic regression with confounding factors and included factors with a P-value of <0.2, the gestational age at delivery and the period showed significant associations with the composite neonatal morbidity (P<0.001 and P=0.0074, respectively). Period II demonstrated significantly decreased risk of composite neonatal morbidity compared with period I (adjusted odds ratio, 0.310; 95% confidence interval, 0.020–0.593).
Table 3
Univariate and multivariable generalized estimating equation logistic regression analysis for composite neonatal morbidity
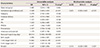
OR, odds ratio; A-OR, Adjusted odds ratio; CI, confidence interval; ART, assisted reproductive technology; PTL, preterm labor; PPROM, preterm premature rupture of membranes.
a)Assessed with a generalized estimating equation logistic regression. P<0.05: statistically significant.
![]()
Discussion
Our study demonstrated that the outcomes of triplet pregnancies significantly improved when period I (1992–2001) and period II (2003–2012) were compared, and these improvements were characterized by decreased composite neonatal morbidity during period II compared with period I. A pregnant woman with a triplet pregnancy has an increased risk of multiple neonatal morbidities. Therefore, we analyzed the characteristics of neonatal morbidities using a GEE logistic regression. Our multivariable analysis showed that independent contributing factors for the improvement of composite neonatal morbidity were attributable to a higher gestational age at delivery and the most recent period.
We have also shown that a higher gestational age at delivery, rather than an increase in the use of antenatal corticosteroids, contributed to the improvement in neonatal outcomes. There was no difference in neonatal gestational age at delivery between the two periods. However, deliveries under 28 and over 34 weeks of gestational age increased significantly in period II. The increase in deliveries under 28 weeks of gestational age can be explained by the lower threshold of viability. Instead of terminating the triplet pregnancies under 28 weeks of gestation, the patient was transferred to a tertiary hospital. In Korea, the rates of delivery prior to the 27th week of gestational age for multiple pregnancies in 1995, 2003 and 2012 have been reported to be 3 (0.03%), 68 (0.69%) and 358 (2.29%), respectively [7]. However, we could not explain the increase in deliveries over 34 weeks of gestational age. Atosiban has been used in Korea since 2006 and was used in this study. However, noting an increased birth rate after 34 weeks of gestation in maternal characteristics (P=0.056) resulting from the use of tocolytics was difficult because betamimetics and MgSO4 are used as first-line drugs [27] and because there was no difference in the use of the various tocolytics between the two periods. When our period II data is compared to U.S. birth data, gestational age at delivery (32.5 vs. 31.97 weeks) and mean birth weight (1,683 vs. 1,660 g) were similar. Our period II data also had a lower rate of delivery under 32 weeks (30.2% vs. 36.8%) and a lower rate of birth weight of under 1,500 g (29.8% vs. 35%) compared to U.S. birth data. We believe that this difference is probably due to an increased incidence of gestational age over 34 weeks.
In a similar study, despite the use of new tocolytics, such as oxytocin receptor antagonists or calcium channel blockers, no prolonged pregnancies or delayed preterm deliveries of triplets occurred. Furthermore, the proportion of newborns with extreme prematurity (<28 weeks) has not changed over the last three decades [14]. Ballabh et al. [15], analyzed the neonatal outcomes of triplets from 1993 to 2000. An increase in the use of antenatal corticosteroids was observed over that study period, but the incidence of RDS remained fairly constant. There was no definitive trend in the frequencies of surfactant use, patent ductus arteriosus, IVH, or ROP [15].
In our study, we found that the use of antenatal corticosteroids was similar between periods. The use of antenatal corticosteroids in singleton pregnancies with a risk of preterm birth lowers the incidence and severity of RDS [28]. Additionally, according to a systemic review, antenatal corticosteroid therapy enhances the circulatory stability of preterm neonates, lowering the risks of IVH, NEC, and systemic infection during the first 48 hours of life [29]. Although some studies have reported that a complete course of antenatal corticosteroid therapy significantly lowers the rates of RDS and IVH in preterm neonates from multiple pregnancies [1130], many studies have not been able to identify the source of the improvement in neonatal outcomes [1415]. Whether the effect of corticosteroid therapy decreases in multiple gestations has not been determined. However, Jobe [31] has hypothesized that the reason why the effect of antenatal corticosteroid therapy is low in twins is not because of the standard dose, but because the effect of corticosteroid therapy varies depending on the reaction of the fetus. Jobe [31] insists that in the PTL of twin pregnancies, there is not enough stress for the fetus to react to antenatal glucocorticoids.
Preeclampsia is related to the patient's socioeconomic status [32]. The decreased incidence of preeclampsia in Korea can be related to large improvements in socioeconomic status and the introduction of the universal voucher scheme [3334]. However, the incidence of preeclampsia during period II was extremely low. A possible explanation for this extremely low incidence may be the influence of the small sample size. During the study period, there was a significant increase in the antepartum hemoglobin level, whereas the frequency of women who developed anemia declined. This is presumably attributed to education regarding the optimal amount of iron supplementation for women with triplet pregnancies in prenatal care and to improved nutrition [35].
SFR in triplet pregnancies has been performed to decrease pregnancy loss, antenatal complications, birth before 36 weeks, and neonatal death [17]. However, a meta-analysis of 893 triplets reported that although SFR decreased the early preterm birth rate, SFR increased the miscarriage rate before 24 weeks from 4.4% to 8.1% [16]. Regardless of the change in the miscarriage rate, the meaning of a miscarriage after SFR differs from that of a spontaneous miscarriage. Moreover, if parents with a history of infertility undergo an abortion, a miscarriage may cause psychological trauma to the parents and is also a burden for the doctor who performs the procedure. Although the neonatal outcome and prognosis of a triplet pregnancy are poorer than those of singleton and twin pregnancies, advances in perinatal and neonatal care have changed the outcomes of triplet pregnancies over the last few decades [14]. However, a recent study reported that neonatal and infant mortality of triplets have not changed in Korea between 2009 and 2015 [36]. Further research regarding improvements in triplet pregnancy outcomes would be useful for providing counseling regarding SFR to women with triplet pregnancies and a history of infertility.
Although this study included two tertiary-care hospitals in Korea, the relatively small sample size of the study population may limit the power of some of the results derived from this study. To overcome this disadvantage, we performed a multivariable analysis to uncover the independent factors associated with improved neonatal outcomes in the most recent period and found that the significant independent predictors for neonatal morbidity were lower gestational age at delivery and the period (early). In addition, another limitation of the study was that the long-term outcomes of the neonates were not included.
In summary, the composite neonatal outcome of triplet pregnancies was significantly improved during the last two decades and was associated with a higher gestational age at delivery in the most recent period. This new data may provide very useful information for physicians and women with high-order multiple gestations, especially when compared with data from earlier time periods.
 XML Download
XML Download