

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Depression and anxiety are a leading cause of disability, posing a significant challenge to stable employment, productivity, progression, and success among employees.1 These disorders also have the highest costs associated with loss of productivity among all chronic illnesses.2 People with mental disorders such as depression and anxiety experience an average of 15%–30% lower employment rates compared to the general population with double the long-term unemployment rate as compared to the same reference group.3 For those who succeed in gaining employment, there is an increased risk of exposure to inequalities at work, such as lower salaries and discrimination.3 In addition, depression and anxiety have been shown to impair the quality of life, work performance, and social functioning of employees in the workplace.2
Resilience refers to the capability of successfully adapting to stressors and maintaining psychological well-being in the face of difficulties.4 Resilience to stress is dynamic and multidimensional. When facing stress or trauma, people may develop post-traumatic psychopathology or recover relatively rapidly, showing negligible psychological aftereffects. The extent to which responses occur depends on interconnected and synergistic factors, including the individual's neurobiological and psychological characteristics, the history of personal trauma, and the accessibility of social support systems.45 Psychological, neurobiological, social, and mental approaches to improving resilience have been proposed to reduce the likelihood of developing stress-induced depression and anxiety and to treat stress-induced psychopathology. Psychosocial features related to depression and/or resilience include positive emotions (optimism and humor), active coping styles, facing fears, cognitive flexibility (explanatory style, cognitive reappraisal, and acceptance), moral compass (altruism), physical exercise, social support, and so forth.5
Numerous studies have been conducted on resilience as a protective factor for depression in the general elderly population as well as for the burnout syndrome and posttraumatic stress disorder (PTSD) among special occupational groups. In a meta-analysis, people without depression showed higher scores on a resilience scale than people with depression.6 In addition, previous studies reported resilience as a protective factor for PTSD symptoms in paramedics,7 paramedic trainees,8 ICU nurses,9 police officers,10 first responders and military personnel,11 and interpreters for refugees.12
As previous research has shown, resilience may be an important factor counteracting the negative consequences of high levels of job stress, such as depression and/or anxiety. A better understanding of the relationships between these variables can also be used to examine how resilience can buffer or improve the worst effects of stress on employees, and can serve as a basis for future studies of interventions designed to improve employee resilience. We assumed that the resilience of employees is related to low levels of depressed mood and anxiety. In addition, we hypothesized that resilience mediates the negative consequences of high levels of occupational stress, such as depression and anxiety.
METHODS
Participants
This study was conducted as a part of the Kangbuk Samsung Workplace Mental Health Study. This is a cross-sectional survey of Korean workers aged between 19 and 65 years who attended a workplace mental health check-up program at the Workplace Mental Health Institute, Kangbuk Samsung Hospital, Seoul, Korea. Participants were urban white collar workers employed by eight private companies and local governmental organizations in Korea. All workers were invited to voluntarily participate in the mental health examination. The present study was performed from June 2015 to February 2016 (n = 1,479). Questionnaire responses were collected from 1,079 persons, with 1,076 valid responses (men/women, 686/390; active response rate, 99.7%).
Measures
Dependent variables
The severity of depression was assessed with the Korean version of the Center for Epidemiologic Studies rating scale for Depression (CES-D).1314 CES-D is a self-report questionnaire, consisting of 20 items scored on a 4-point Likert scale from 0 to 3. The Beck Anxiety Inventory (BAI),15 a 21-item self-report questionnaire scored on a 4-point Likert scale from 0 to 3, was used to assess the level of anxiety. Previous studies have established the high internal consistency and validity of both the CES-D and BAI tools.131415
Independent variables
The socio-demographic factors collected as independent variables were age, gender, level of education (higher educational level means years of education ≥ 16), and marital status (married or unmarried). In addition, job-related demographic factors were also collected, such as job grade (lower job grade means staff or assistant manager; higher job grade means manager, deputy general manager, or general manager) and duration of work at the current workplace (years).
Job stress was assessed using the Short Form of the Korean Occupational Stress Scale (KOSS-SF),16 a 24-item self-report questionnaire scored on a 4-point Likert scale from 1 to 4. It comprises the following seven subscales of work-related stress factors: job demands, absence of job control, interpersonal conflict, job instability, organizational system, insufficient compensation, and occupational environment. The KOSS-SF previously showed high internal consistency and validity.16 In this study, we used the total score on KOSS-SF.
Resilience was measured by the Korean version of the Connor-Davidson Resilience Scale (K-CD-RISC).17 The K-CD-RISC, a self-report questionnaire consisting of 25 items scored on a 5-point Likert scale from 0 to 4, measures five aspects of psychological resilience; these are Factor 1: “hardiness” (personal competence, high standards, and tenacity of purpose; subtotal score of the 9 Items 18, 19, 15, 16, 17, 23, 14, 4, and 1); Factor 2: “persistence” (tolerance to negative affect, the strengthening effects of stress and circumspect thinking, and decision-making when coping with stress; subtotal score of the 8 Items 11, 21, 24, 25, 22, 5, 10, and 12); Factor 3: “optimism” (feeling hopeful about the future or about the chances of success of a particular event; subtotal score of the 4 Items 9, 8, 7, and 6); Factor 4: “support” (ability to receive help from another; subtotal score of the 2 Items 13 and 2); and Factor 5: “spirituality” (being spiritual in nature, spirituality correlated with closeness to God, and feelings of interconnectedness in the world and between living things; subtotal score of the 2 Items 20 and 3).17 A previous study showed that the K-CD-RISC had good reliability and validity for the assessment of resilience in the Korean population.17
Statistical analysis
Before conducting the regression analysis, Pearson's correlation and multicollinearity diagnostics were performed. We used the variance inflation factor (VIF) as an indicator of multicollinearity. Although there are many differences in the literature regarding the VIF values to be used as thresholds for collinearity, commonly recommended values are 10 and 5.1819 All continuous variables included in the regression analysis in this study yielded values less than 5, so there was no multicollinearity. To determine the influence of resilience on depression and anxiety of employees, we performed hierarchical linear regression analyses using the CES-D and BAI scores as the dependent variables, respectively. In Model 1, associations of socio-demographic factors with depressive mood (measured by CES-D) and anxiety (measured by BAI) were tested. Job-related demographic factors were added in Model 2 to test the associations of job-related demographic factors beyond the effects of socio-demographic factors. Job stress (measured by KOSS-SF) was added in Model 3 to test the associations of job stress beyond the effects of socio-demographic and job-related demographic factors. Last, resilience was added in Model 4a to test the associations of resilience (measured by K-CD-RISC) beyond the effects of socio-demographic factors, job-related demographic factors, and job stress. All these analyses were repeated with the subtotal scores of the five factors of the K-CD-RISC instead of the K-CD-RISC total score as independent variables in Model 4b. Statistical significance was set a priori at α = 0.05 (two-sided) to limit Type-I error. All analyses were conducted using the Complex Samples module of the PASW statistics software package, version 19 (SPSS Inc., Chicago, IL, USA).
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board (IRB) of Kangbuk Samsung Hospital (IRB No. KBSMC 2013-01-217). The IRB waived the informed consent requirement because this study used only de-identified data routinely collected from workplace mental health screenings.
RESULTS
Participant characteristics
Table 1 summarizes the descriptive information on socio-demographic factors, job-related demographic factors, job stress, depressive mood, anxiety, and resilience. The mean age of the participants was 38.86 ± 10.32 years and 36.2% of the participants were women.
Table 1
Socio-demographic and psychological characteristics of the study population
Hierarchical linear regression analyses with the CES-D score as the dependent variable
Results of the hierarchical linear regression analysis of the association of the level of depressive mood with socio-demographic factors, job-related demographic factors, job stress, and resilience are summarized in Table 2.
Table 2
Hierarchical linear regression analyses with the CES-D score as the dependent variable (n = 1,076)
Socio-demographic factors
Socio-demographic factors, tested in Model 1, explained 10.8% of the variance in the level of depressive mood. Being women (P < 0.001) and being unmarried (P < 0.05) were associated with greater CES-D scores. On the other hand, age was negatively associated with CES-D scores (P < 0.001).
Job-related demographic factors
Job-related demographic factors, tested in Model 2, explained an additional 0.2% of the variance in the level of depressive mood beyond the effects of socio-demographic factors. None of the job-related demographic factors was associated with the CES-D score beyond the effects of socio-demographic factors. Age was statistically non-significant in Model 2.
Job stress
Job stress, tested in Model 3, explained an additional 18.2% of the variance in the level of depressive mood beyond the effects of socio-demographic and job-related demographic factors. The KOSS-SF score was positively associated with the CES-D score (P < 0.001). The variable marital status was statistically non-significant in Model 3.
Resilience
Resilience, tested in Model 4a, explained an additional 3.3% of the variance in the level of depressive mood beyond the effects of socio-demographic factors, job-related demographic factors, and job stress. The K-CD-RISC score was negatively associated with the CES-D score (P < 0.001). Additionally, in this final model, being women remained independently related to a higher CES-D score (P < 0.05) and the KOSS-SF score independently continued to show a positive relationship with the CES-D score (P < 0.001). This final model explained 32.5% of the variance in the level of depressive mood. Further, in Model 4a, the relative influence of the significant variables was defined as the magnitude of the absolute value of the standardized coefficient β. Comparison showed that variables influenced the CES-D score in the following order: women gender (β = 1.129), the KOSS-SF score (β = 0.257), and the K-CD-RISC score (β = −0.119).
Hierarchical linear regression analyses with the CES-D score as the dependent variable and the five factors of K-CD-RISC as independent variables
Results of the hierarchical linear regression analysis that tested the association of the level of depressive mood with socio-demographic factors, job-related demographic factors, job stress, and the five factors of resilience are summarized in Table 3. The results from Model 1 to Model 3 were the same as in Table 2.
Table 3
Hierarchical linear regression analyses with the CES-D score as the dependent variable and the five factors of K-CD-RISC as independent variables (n = 1,076)

The five factors of resilience
The five factors of resilience tested in Model 4b explained an additional 4.9% of the variance in the level of depressive mood beyond the effects of socio-demographic factors, job-related demographic factors, and job stress. The scores for “Factor 1: hardiness” (P < 0.01) and “Factor 4: support” (P < 0.001) of the K-CD-RISC were negatively associated with the CES-D score. Additionally, in this final model, being women (P < 0.05) and being unmarried (P < 0.05) remained independently related to higher CES-D scores and the KOSS-SF score independently continued to show a positive relationship with the CES-D score (P < 0.001). This final model explained 34.1% of the variance in the level of depressive mood. Comparison showed that variables influenced the CES-D score in the following order: unmarried status (β = 1.261), women gender (β = 1.252), Factor 4: “support” (β = −0.892), the KOSS−SF score (β = 0.241), and Factor 1: “hardiness” (β = −0.212).
Hierarchical linear regression analyses with the BAI score as the dependent variable
Results of the hierarchical linear regression analysis that tested the association of the level of anxiety with socio-demographic factors, job-related demographic factors, job stress, and resilience are summarized in Table 4.
Table 4
Hierarchical linear regression analyses with the BAI score as the dependent variable (n = 1,076)
Socio-demographic factors
Socio-demographic factors, tested in Model 1, explained 8.1% of the variance in the level of anxiety. Being women was associated with greater BAI scores (P < 0.001), whereas age was negatively associated with the BAI scores (P < 0.01).
Job-related demographic factors
Job-related demographic factors, tested in Model 2, explained an additional 0.3% of the variance in the level of anxiety beyond the effects of socio-demographic factors. None of the job-related demographic factors were associated with the BAI score beyond the effects of socio-demographic factors. Age was statistically non-significant in Model 2.
Job stress
Job stress, tested in Model 3, explained an additional 11.7% of the variance in the level of anxiety beyond the effects of socio-demographic factors and job-related demographic factors. The KOSS-SF score was positively associated with the BAI score (P < 0.001).
Resilience
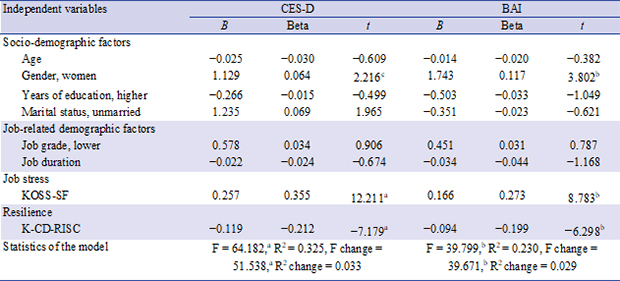
Resilience, tested in Model 4a, explained an additional 2.9% of the variance in the level of anxiety beyond the effects of socio-demographic factors, job-related demographic factors, and job stress. The K-CD-RISC score was negatively associated with the BAI score (P < 0.001). Additionally, in this final model, being women remained independently related to higher BAI scores (P < 0.001) and the KOSS-SF score independently continued to show a positive relationship with the BAI score (P < 0.001). This final model explained 23% of the variance in the level of anxiety. Comparison showed that variables influenced the BAI score in the following order: women gender (β = 1.743), the KOSS-SF score (β = 0.166), and the K-CD-RISC score (β = −0.094).
Hierarchical linear regression analyses with the BAI score as the dependent variable and the five factors of K-CD-RISC as independent variables
Results of the hierarchical linear regression analysis that tested the association of the level of anxiety with socio-demographic factors, job-related demographic factors, job stress, and the five factors of resilience are summarized in Table 5. The results from Model 1 to Model 3 were the same as in Table 4.
Table 5
Hierarchical linear regression analyses with the BAI score as the dependent variable and the factors of K-CD-RISC as independent variables (n = 1,076)

The five factors of resilience
The five factors of resilience, tested in Model 4b, explained an additional 4.2% of the variance in the level of anxiety beyond the effects of socio-demographic factors, job-related demographic factors, and job stress. The scores on “Factor 1: hardiness” (P < 0.01) and “Factor 4: support” (P < 0.01) of the K-CD-RISC were negatively associated with the BAI score. Additionally, in this final model, being women remained independently related to higher BAI scores (P < 0.001), and the KOSS-SF score independently continued to show a positive relationship with the CES-D score (P < 0.001). This final model explained 24.3% of the variance in the level of anxiety. Comparison showed that the variables influenced the BAI score in the following order: women gender (β = 1.738), Factor 4: “support” (β = −0.536), Factor 1: “hardiness” (β = −0.188), and the KOSS-SF score (β = 0.156).
DISCUSSION
This study aimed to identify the mechanisms underlying the interactions among risk and protective factors related to depressive mood and anxiety among Korean employees. In this study, being women and high levels of job stress were associated with greater depressive mood and anxiety. In contrast, resilience was negatively related to depressive mood and anxiety after adjusting for demographic variables and the level of job stress. Among the five factors of resilience, “support” and “hardiness” were protective factors for depressive mood and anxiety after adjusting for demographic variables and the level of job stress.
This study found that women employees have a higher level of depression compared to men employees. No clear explanation has been found for gender differences in the level of depression experienced in the workplace so far. One explanation is that women may experience conflict between their work and their families. Higher stress among women and levels of depression appear to be related to the multiple roles that they are expected to play.20 In a previous systematic review of prospective studies on the consequences of occupational burnout, psychological influences included sleep disturbance, depressed mood, use of antidepressants and other psychotropic medications, hospitalization for psychiatric disorders, and other psychiatric symptoms.21
In this study, a high level of job stress was associated with greater depressive mood and anxiety. The cause of depression and anxiety is multifactorial, including the interaction of biological, psychological, and social factors such as genetic susceptibility, personality vulnerability to stressors, socio-economic difficulties, and severe undesirable life events.22 It has been suggested that work-related risk factors contribute to the development of depression and anxiety, with increasing evidence from systematic reviews, including meta-analysis studies. The majority of these studies reported that occupational stress characterized by a combination of high job demands and low job control is associated with an increased risk of depression.2324
This study suggested that the association between job stress and depression and anxiety symptoms might be mediated by an individual's resilience. The results of multivariate logistic regression analysis showed that a low level of self-resilience was significantly related to the development of depressive mood and anxiety among employees after adjusting for demographic variables and the level of job stress. Previous research has reported a negative association between resilience and the subsequent development of psychiatric symptoms.49 However, in this study, resilience could only explain of 3%–5% of depression and anxiety. A meta-analysis of the association between resilience and depression in the general elderly population showed that resilience had a moderate effect on depression (r = −0.35).6 Although no meta-analysis for the workplace has yet been performed, resilience has been shown to have a small to moderate effect on the development of depression and anxiety in a study conducted on a variety of occupations.6 The reason for the differences in the effect size of resilience on mental disorder among workers is considered to be the different characteristics and intensity of stress to which they are exposed according to occupation. In this study also, the degree of occupational stress had a great effect on depression and anxiety. However, occupational stress is often difficult to adjust and modify. Therefore, the results of this study may be valuable in spite of the small effect, if they can be used to prevent depression and anxiety by promoting resilience in people exposed to uncontrollable occupational stress. One definition of resilience is the process of returning to functioning at pre-stress levels without experiencing serious dysfunction or psychopathology.25 Resilience is considered to be a capacity to search for and use health care resources in the context of hardship, in addition to utilizing resources from supportive families and communities to promote one's welfare.26 Therefore, resilience can reduce the risk of mental illness, including depression and anxiety disorders, through effective emotional control and active pursuit of support or nurturing relationships.27
It has been suggested that people with psychopathology may also show some features of resilience and that the level of resilience can influence the treatment response. In a study using the Connor-Davidson Resilience Scale (CD-RISC) to evaluate the resilience of patients with PTSD, patients who reported greater resilience showed significantly better treatment effects than those who reported lesser resilience.28 The high spontaneous remission rates from mental illnesses suggest that many individuals can overcome psychological difficulties without formal treatment and thereafter show some long-term features of resilience. A study of spontaneous remission from major depressive disorders reported that 23% of patients experienced remission from untreated depression within 3 months, 32% within 6 months, and 53% within 12 months.29
In this study, “support” and “hardiness” were protective factors for depressive mood and anxiety among the five factors for resilience (hardiness, persistence, optimism, support, and spirituality).
It is not surprising that “support,” which means the ability to receive help from another, is a protective factor for depressive mood and anxiety. This factor includes items such as, “There is at least one person who is close and able to help me when I am stressed,” and “I know who to ask for help in a stressful/crisis situation.” A previous study conducted with radiologists reported social support to be a protective factor against depressive mood and anxiety.30 In a previous study of character strengths, “judgement” and “kindness” in women and “teamwork” and “creativity” in men were protective factors against depression and suicidality among employees.31 In addition, strengths related to social support, including “kindness,” “teamwork,” and “humor,” were associated with decreased negative coping among employees in various types of jobs.32 According to another workplace survey, “teamwork” is the most important predictor of job performance and general well-being in the workplace.33 In a meta-analysis of the impact of workplace environments on burnout, high-levels of workplace justice, work control, and high levels of social support from colleagues were shown to be protective factors against the burnout syndrome.34
“Hardiness” means personal competence, high standards, and tenacity of purpose. This factor includes items such as, “I can make a difficult decision that others do not like,” “I can adapt when change occurs,” “Rather than letting others make all the decisions, I like to lead the problem-solving process,” and “I can handle unpleasant or painful emotions such as sadness, fear, and anger.” Therefore, “hardiness” reflects the individuals' abilities of decision-making, problem-solving, and emotional control.
An adaptive coping strategy helps individuals to effectively deal with the causes of stress and thus to devote greater energy to achieving their intended purpose.35 A problem-focused approach involves analyzing the problem in detail and adjusting or eliminating problems that cause stress. In a previous study, “judgement” was reported to be a protective character strength against suicidality in women workers.31 “Judgment,” representing intellectual ability, plays an important role in selecting adaptive coping skills and avoiding maladaptive coping skills in the workplace.32 This ability brings individuals self-efficacy and a sense of control when doing new things and lessens stress.36 This is especially useful when individuals can identify the cause of the problem and change the situation. In the workplace, this includes adjusting working conditions so that the worker feels less stressed or unproductive.37 Such adjustments can be more useful if changes in working conditions positively affect many other fellow workers.
In previous studies, emotional intelligence has been frequently reported as one of the protective factors against occupational stress and burnout, as well as negative health outcomes.38 Emotional intelligence refers to a psychological resource regarding one's ability to process information about one's own and other's feelings, to understand and manage emotion-related information, and to use this information to solve problems.38 It is related to positive attitudes and behaviors regarding one's occupation and job satisfaction.39 In addition, the positive influence of emotional intelligence on emotional and physical health is mediated by work engagement as well as the reduced use of unhealthy coping strategies.39
Resilience can be learned because it is not a stable trait, but rather a characteristic.25 The objective of resilience-training intervention is to increase an individual's ability to deal with stressors, lower stress sensitivity, and increase stress adaptability, yet few studies of interventions to increase resilience have been conducted in the past. Studies have reported that resilience interventions were effective in decreasing depressive symptoms in individuals with childhood trauma.40 Resilience can be molded and strengthened in people with psychopathology. In previous studies investigating resilience in PTSD patients, it was found that participants' resilience scale scores significantly improved after treatment.28 Certainly, there is evidence that learning resilience is more appropriate for those who have difficulty adapting to situations than those who are adaptable.
Psychological features that can be developed to increase resilience have been reported, such as optimism, altruism, cognitive flexibility, active coping strategies, supportive social networks, a sense of humor, exercising, finding a resilient mentor, learning to be proficient in fear, and developing a personal moral compass or belief.9 In addition, key elements to enhance resilience have been suggested, including emotional regulatory training to identify and control responsiveness and impulsivity; cognitive approaches to reconstruct thought processes and enhance positive emotions; supportive social network within families, colleagues, and mentors to enhance the support system; health-related information on food, exercise, and sleep to promote protective behavioral habits; and neurobiological approaches to enhance the capability to manage stress, such as mindfulness-based stress reduction.5 Future experimental research is needed to evaluate whether resilience interventions for employees can reduce their occupational stress, depressive mood, and anxiety.
This study had several limitations. First, the current study did not collect data on various psycho-socio-demographic factors and job-related factors, such as severe life events outside work, family history of psychiatric disease, history of medical or psychiatric disease, personality traits, socio-economic status, working hours, and work environment, that potentially influence occupational stress, mood, and anxiety. Second, this was a cross-sectional study. Although resilience is more trait-like than state-like and has been considered a causal factor in the literature, this may be a limitation in causality. Third, readers need to consider reporting biases, because a self-report survey was used during the data collection. Fourth, readers should consider the possibility of non-response bias, because we did not include data from those who failed to respond to the questionnaires. We had tried to increase the response rate by sending reminders, but only 1,079 of 1,479 participants answered the questionnaires. Therefore, future longitudinal studies with a larger number of study participants using objective evaluation tools and controlling for potentially confounding factors are needed to confirm and generalize the results of this study.
Based on the results of the current study, we suggest that focusing on the resilience of employees, especially on the factors of “support” and “hardiness,” as well as developing and engaging in interventions that increase resilience in the workplace, can serve to protect against depressive mood and anxiety, especially in those with high levels of job stress. Future research needs to focus on developing interventions to promote such resilience among employees in the workplace.
 XML Download
XML Download