

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Enhanced understanding of the pathogenic mechanism of systemic lupus erythematosus (SLE) has led to more proper and challenging use of corticosteroids and other immunosuppressive agents such as mycophenolate mofetil (MMF), azathioprine, and cyclophosphamide, as well as development of novel targeted biologic therapeutics, including rituximab and belimumab during several decades.12 It is well established that MMF, azathioprine, and cyclophosphamide are effective in the induction and maintenance of lupus nephritis (LN) and other features such as mucocutaneous lesions and neurological involvement. These therapeutic approaches have greatly improved morbidities and mortalities associated with SLE. However, the complexity of pathogenesis and clinical phenotypes of the disease complicates successful management.
MMF is a prodrug of mycophenolic acid that inhibits guanosine nucleotides through reversible suppression of the enzyme inosine 5-monophosphate dehydrogenase.34 The action mechanisms of MMF suppress proliferation and differentiation of activated T-lymphocytes, expression of adhesion molecules, and autoantibody formation by B-lymphocytes. Several randomized controlled trials have investigated whether MMF is a potent immunosuppressant with a crucial role in induction and maintenance management of proliferative LN. Most studies have demonstrated that patients treated with MMF showed superior or equivalent effects on suppression of renal inflammation in LN compared to those treated with cyclophosphamide or azathioprine.567 In addition, there is increasing evidence that MMF has some beneficial effects on non-renal manifestations including hematologic and neuropsychiatric abnormalities refractory to other conventional therapeutics.89101112
However, data for therapeutic effects of MMF on organs or tissues other than kidney remain sparse for SLE. Thus, we investigated the effects of MMF on non-renal manifestations in patients with SLE using the data of an observational registry from 2014 to 2018.
METHODS
Study population
The Korean Lupus Network (KORNET) registry, established in January 2014, is an observational and prospective registry for SLE patients from four university-based medical centers. Enrolled patients fulfilled the 1982 revised and 1997 updated American College of Rheumatology classification criteria for SLE.1314 The registry for clinical information was annually followed up and updated from baseline to the 2nd follow-up. A total of 505 patients with SLE were enrolled in the KORNET registry at baseline. However, this study recruited 439 SLE patients who completed clinical data collection after the 2nd follow-up visit. During the follow-up period, 66 SLE patients were excluded by follow-up loss or withdrawing consent.
Collection of clinical information
At baseline, we assessed age, gender, duration of education (year), smoking status (yes or no), and alcohol intake (yes or no). Clinical manifestations related with SLE including malar rash, discoid rash, photosensitivity, oral ulcer, arthritis, serositis (pleural effusion and pericardial effusion), neurological disorders (seizure and psychosis), and hematologic abnormalities (hemolytic anemia, leukopenia [< 4,000/mm3 on ≥ 2 occasions], lymphopenia [< 1,500/mm3 on ≥ 2 occasions], and thrombocytopenia [< 100,000/mm3]) were identified at all visits. At baseline, LN was confirmed by histology-proven diagnosis. Patients with non-renal manifestations were defined as those without histologically diagnosed LN.
Other laboratory findings such as white blood cell (WBC), hemoglobin, platelet, erythrocyte sedimentation rate (ESR, mm/hr), C-reactive protein (CRP, mg/mL), complement 3 (C3, mg/mL), and complement 4 (C4, mg/mL) were evaluated. Considering immunologic abnormalities, positivity for each anti-dsDNA antibody, anti-Sm antibody, and anti-phospholipid antibodies such as including anti-cardiolipin antibody, lupus anticoagulant, and false positive reaction for syphilis was also identified. Concurrent medications such as hydroxychloroquine, methotrexate, tacrolimus, azathioprine, and corticosteroid were identified at enrollment.
Assessment of disease activity and damage
This registry utilized physician global assessment (PGA), Safety of Estrogen in Lupus Erythematosus National Assessment (SELENA)-SLE disease activity index (SLEDAI), and SELENA-SLEDAI flare index for measurement of disease activity and improvement or worsening of disease activity.1516 The Systemic Lupus International Collaborating Clinics/American College of Rheumatology (SLICC/ACR) damage index was applied for evaluating lupus-related organ damage.17
Determination of LN
LN status was confirmed based on renal biopsy and its findings. Renal biopsy results were determined on the basis of World Health Organization (WHO) criteria or 2003 International Society of Nephrology (ISN)/Renal Pathology Society (RPS) Classification.18 The use of two classification criteria for LN was permitted in this study because not all participating medical centers used the same classification criteria. These criteria were used only to confirm the presence of renal disease and did not consider the extent or severity of inflammation.
Statistical analysis
Data are described as median and interquartile range for quantitative variables and frequency with percent (%) for qualitative variables. Analysis for all variables by group (MMF and non-MMF) effects with time (baseline, 1st follow-up, and 2nd follow-up) were performed using generalized estimation equation (GEE). For qualitative variables, Poisson distribution, gamma distribution, and normal distribution were used as distribution assumption. The log function was used as link function and unstructured covariance matrix was used. For quantitative variables, binomial distribution was used as distribution assumption. The logit function was used as link function and unstructured covariance matrix was used.
To comparison frequencies of clinical manifestations of malar rash, discoid rash, photosensitivity, oral ulcer, arthritis, serositis, neurological disorder, hematologic manifestations, and immunologic abnormalities between groups (MMF and non-MMF) and among times (baseline, 1st follow-up, and 2nd follow-up), the analyses were divided into total patients, patients with LN, and patients without LN. In the analysis for hematologic abnormalities, subgroup analysis for hemolytic anemia, leukopenia, lymphopenia, and thrombocytopenia was also performed. All tests were 2-sided, and a P value less than 0.05 was considered to indicate statistical significance using IBM SPSS ver. 19.0 (IBM Corp., Armonk, NY, USA).
Ethics statement
All patients registered in this study provided informed consent for inclusion in the study. This study was also approved by the Institutional Review Board of Daegu Catholic University Medical Center at the time of enrollment in the registry (CR-14-123-L). This study was performed according to the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
RESULTS
General characteristics of enrolled patients
The baseline characteristics of all enrolled patients are described in Table 1. This study enrolled 439 SLE patients with a median age of 44.0 years (36.0–52.0) and of whom 411 were women (93.6%). The median age of 110 patients with biopsy-proven LN was 44.5 years (37.0–54.3), and 103 of them were women (93.6%). The remaining 329 patients free of LN had a median age of 43.0 years (35.0–49.0) and included 308 women (93.6%). Of total SLE patients, 72 (16.4%) reported MMF treatment at study enrollment, comprising 21 patients with LN (19.1%) and 51 patients (15.5%) patients without LN. Table 1 also showed the generalized characteristics of SLE patients treated with MMF.
Table 1
General characteristics of enrolled SLE patients

Data are described as median with interquartile range or number (%).
SLE = systemic lupus erythematosus, MMF = mycophenolate mofetil, SELENA-SLEDAI = Safety of Estrogen in Lupus Erythematosus National Assessment-systemic lupus erythematosus disease activity index, SLICC/ACR = The Systemic Lupus International Collaborating Clinics/American College of Rheumatology.
The effect of MMF on non-renal manifestations in total SLE patients
We analyzed the changes in relevant disease activity and laboratory variables from baseline to the 2nd follow-up between MMF and non-MMF groups. As shown in Table 2, there were significant differences in PCS of SF-36, physician global assessment, SELENA-SLEDAI, SLICC/ACR damage index, WBC, and prednisolone dosage between MMF and non-MMF group (P < 0.001, P = 0.003, P = 0.007, P < 0.001, P = 0.012, and P < 0.001, respectively). It suggests that MMF treatment improved quality of life, disease activity, and disease damage, and also reduced change in WBC and daily dose of prednisolone, compared to non-MMF treatment. In contrast, no differences of BDI, MCS of SF-36, SLE flare index, hemoglobin, platelet, ESR, CRP, complement 3, complement 4, and hydroxychloroquine dosage were not noted between two groups (P > 0.05 for all).
Table 2
Comparison for disease activity, laboratory markers, and medications between MMF and non-MMF groups in total patients

Data were described as median with interquartile range or number (%).
MMF = mycophenolate mofetil, BDI = Beck depression inventory, PCS = physical component score, SF-36 = Short Form-36 health survey, MCS = mental component score, SELENA-SLEDAI = Safety of Estrogen in Lupus Erythematosus National Assessment-systemic lupus erythematosus disease activity index, SLE = systemic lupus erythematosus, SLICC/ACR = The Systemic Lupus International Collaborating Clinics/American College of Rheumatology, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein.
aMean dosage per day for each medication.
In assessment of the effects of MMF on clinical manifestations, frequencies of patients with malar rash, arthritis, renal disorder, and hematologic disorder were significantly different between MMF and non-MMF groups (P = 0.023, P = 0.047, P < 0.001, and P = 0.009, respectively) (Table 3). It suggests that MMF treatment improved these clinical features during follow-up period. However, there are no differences of discoid rash, photosensitivity, oral ulcer, serositis, neurological disorder, anti-dsDNA antibody, anti-Sm antibody, and anti-phospholipid antibody between two groups.
Table 3
Comparison for frequencies of clinical manifestations between MMF and non-MMF groups in total patients

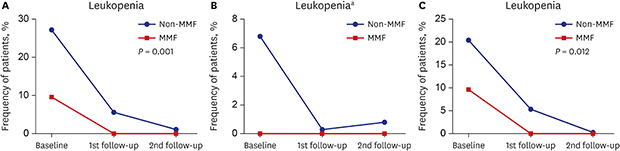
There was significance in frequency of hematologic disorders in total patients (P = 0.009). In subgroup analysis of hematologic abnormalities, the frequency of patients with leukopenia was significantly different between MMF and non-MMF groups (P = 0.001) (Fig. 1A), but there was no difference regarding hemolytic anemia, lymphopenia, and thrombocytopenia (Supplementary Fig. 1A).
Fig. 1
Comparison for changes in frequency for leukopenia between MMF and non-MMF groups. (A) Total lupus patients, (B) patients with lupus nephritis, (C) patients without lupus nephritis. Data was frequency (%) for each variable.
MMF = mycophenolate mofetil.
aIn patients with lupus nephritis, statistical analysis could not be performed because there was no leukopenia in patients treated with MMF.

The effects of MMF on non-renal manifestations in patients with and without LN
Changes in frequencies of clinical manifestations including malar rash, discoid rash, photosensitivity, oral ulcer, arthritis, serositis, neurological disorder, hematologic manifestations, and immunologic abnormalities except for anti-dsDNA antibody were not significantly different considering interaction of time and treatment group in patients with LN (Supplementary Table 1). Subgroup analysis of hematologic abnormalities did not show marked difference in change in frequencies of hemolytic anemia, lymphopenia, and thrombocytopenia (Supplementary Fig. 1B). Considering frequency of leukopenia, there was no patients treated with MMF during follow-up period (Fig. 1B).
In patients without LN, there was significant change in frequency of patients with hematologic disorder considering the interaction of time and group (P = 0.018) (Supplementary Table 2). In subgroup analysis of hematologic abnormalities, there was significant difference in change in frequency of leukopenia (P = 0.012) (Fig. 1C), but not in those of hemolytic anemia, lymphopenia, and thrombocytopenia (Supplementary Fig. 1C).
DISCUSSION
Autoimmune responses mediated by formation of an immune complex; aberrant expression of autoantibodies, autoreactive T lymphocytes, and complements; and production of inflammatory cytokines are peculiar characteristics of SLE, which presents a wide spectrum of clinical manifestations.2122 Diverse immunosuppressive or immunomodulatory medications including hydroxychloroquine, methotrexate, tacrolimus, and azathioprine have been used to control disease activity and prevent flare or organ damage, as has steroid sparing.1 These medications are helpful for cytopenia, arthritis/arthralgia, dermatitis, systemic vasculitis, and neuropsychiatric manifestations. However, there are still clinical manifestations that do not respond to conventional therapy. Over the previous several decades, MMF has been considered a main treatment to manage LN.567 Recently, MMF has been successfully used for management of non-renal manifestations.89101112 Nevertheless, there is not sufficient evidence to demonstrate confidence in the clinical efficacy of MMF for non-renal manifestations in SLE. This is an observational study to determine the therapeutic effects of MMF on non-renal manifestations including musculoskeletal, mucocutaneous, neurological, and hematologic disorders and immunologic abnormalities in Korean SLE patients.
Regarding efficacy of MMF on hematologic manifestations, a systemic review using 20 case series or open-labelled studies has demonstrated that MMF treatment induced good response to autoimmune hemolytic anemia and thrombocytopenia refractory to high-dose prednisolone, intravenous immunoglobulin, or other DMARDs.23 An observational cohort study that enrolled 177 SLE patients showed that 8/13 (61.5%) patients presenting with leukopenia and thrombocytopenia were significantly improved after MMF treatment for 12 months.11 Other studies also have shown good MMF response to autoimmune hemolytic anemia refractory to conventional treatment.824 Ginzler et al.9 demonstrated that 28/47 (60%) patients with LN achieved remission in a hematologic domain based on BILAG score index in a posthoc analysis of the Aspreva Lupus Management Study (ALMS). However, Moder et al.10 reported no statistical improvement of hemoglobin, WBC count, or platelets in 23 SLE patients after 6 months of follow-up. In the present study, there were no differences in hemoglobin and platelet values, but only WBC count was different between two groups (P = 0.012). In addition, the frequency of hematologic disorders in the total study population was significantly different between MMF and non-MMF groups (P = 0.009). Subgroup analysis for hemolytic anemia, leukopenia, lymphopenia, and thrombocytopenia revealed significantly greater improvement in leukopenia in the MMF groups compared to the non-MMF group, but not of any other cytopenia (Fig. 1 and Supplementary Fig. 1). These results suggest that MMF treatment has some efficacy to control and resolve hematologic abnormalities.
Mucocutaneous lesions are frequently treated with conventional treatment modalities such as topical or systemic steroid, hydroxychloroquine, methotrexate, or azathioprine.1 However, MMF can effectively treat lupus-related skin diseases that showed no response to conventional medications. The first report of successful MMF treatment for resistant discoid lupus erythematosus was published in 2001.25 Then, Mok23 reviewed 16 cases with lupus-related cutaneous lesions refractory to diverse therapeutics, in most of whom MMF use induced symptomatic improvement. Another study demonstrated that 73% (5/7) of patients with mild to moderately active non-renal lupus experienced improvement of skin lesions during the study period.10 Yahya et al.8 also reported improvement of more than 20% of skin lesions in two of three patients. Consistent with previous studies, we also found decreased frequency of patients with malar rash in the MMF group compared to the non-MMF group between baseline and follow-up periods. In contrast, poor response to MMF for management of refractory cutaneous lesions has been proposed. In analysis of seven SLE patients with diverse cutaneous lesions, five had no clinical response, one showed partial response, and one had initial response and subsequent relapse while on MMF treatment.26 The discrepancy in these therapeutic effects may be related to the pathological and immunological diversity of lupus-related skin lesions. A more careful consideration of the usefulness of MMF therapy is needed through analysis of the relationship between MMF and cutaneous lesions.
Neuropsychiatric manifestations, including cognitive impairment, seizure, stroke, central and peripheral neuropathy, and psychosis, are a severe feature and contribute to increasing risk of morbidity and mortality in SLE patients.27 High-dose corticosteroids and/or cytotoxic agents such as cyclophosphamide or azathioprine are considered main therapeutics according to severity of these manifestations.27 Some studies have demonstrated favorable effects of MMF on neuropsychiatric features of SLE. In analysis of ALMS, 3 patients with neuropsychiatric features were treated with MMF; two showed partial response and one experienced remission.9 Mok23 reported clinical outcomes of seven neuropsychiatric lupus patients presenting with myelopathy or confusion state/delirium, most of whom showed beneficial efficacy ranging from complete recovery to partial response. In contrast, one observational study with 75 lupus patients treated with MMF for up to 5 years demonstrated that two patients with neurological symptoms improved after administration of MMF, but new neurological features occurred in 6 patients while on MMF treatment.28 In the present study, we found no difference in frequency of patients with neurological disorders between MMF and non-MMF groups. Interpretation of our findings may be limited because the neurological disorders included in this study were only seizure and psychosis.
In our study, we could consider the possibility of MMF treatment in musculoskeletal manifestations. There was a significant difference in arthritis between MMF and non-MMF groups (P = 0.045). Moder et al.10 reported improvement of inflammatory arthritis in 4/7 (57%) patients after MMF treatment. Recently, a more efficient effect of complete clinical response in arthritis was cumulatively noted in 25/30 (83.3%) patients treated with MMF for 12 months.11 However, the effects of MMF on musculoskeletal manifestations have not been determined due to lack of sufficient data.
Some evidence that MMF treatment was found to enhance quality of life in patients with SLE. Wilson et al.29 demonstrated that MMF induced better quality of life, compared to cyclophosphamide in a study using a patient-level stimulation model. In comparison of quality of life in 12 patients with LN, MMF treatment was closely linked with less emotional wellbeing, less energy/fatigue, better physical functioning, and less role limitation due to emotional problems.30 In this study, we also observed more improvement of PCS of SF-36 in patients treated with MMF, compared to those with non-MMF during follow-up period.
There are some limitations in understanding the effects of MMF on non-renal features based on the results of this study. First, this study could not clarify whether the treatment effect of MMF was only the effect of MMF or the effect of other combination medications. Second, the non-renal manifestations analyzed in our study were mainly based on the diagnosis criteria for SLE.1314 This cannot rule out the possibility that assessment for non-renal manifestations might be lacking or underestimated. Third, our study could not determine whether MMF alone has a beneficial effect on leukopenia. There was a limit to revealing the interactions with other anti-rheumatic drugs. Another limitation is that the sample size of MMF-treated group seems to be small. On the other hand, the strength of this study is that using GEE analysis that considers time and group interaction has improved the statistical reliability. In addition, this study enrolled a sufficient patient number compared to previous studies.
In conclusion, this observational study provided relevant evidence that MMF can be an alternative therapeutic option for hematologic abnormalities especially leukopenia refractory to conventional treatment modalities. To strengthen the robustness of our result, further randomized controlled study of additional effects of MMF on diverse non-renal manifestations should be performed in a larger study population.
 XML Download
XML Download