

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Extrahepatic portal vein obstruction (EHPVO) and portal cavernoma transformation is not commonly seen in pediatrics [1234567]. High mortality rates are associated with its consequences of portal hypertension and esophageal varices. Multiple risk factors have been linked to such entity consisting mainly of placement of umbilical vein catheterization, sepsis and necrotising enterocolitis during the neonatal period [45]. However, few reports had suggested hepatic abscesses as a predisposing factor especially in the English literature [6]. We present a 12-month-old female infant that had neonatal sepsis with liver micro-abscesses and subsequently was found to develop a delayed-onset portal hypertension with cavernoma transformation. Due to the rarity and delayed presentation of such diagnosis in pediatric age group, our aim is to raise the possibility of delayed-onset portal hypertension as a complication of liver abscess and neonatal sepsis.
CASE REPORT
A 12-month-old Saudi female infant girl presented with history of hematemesis and melena of one day duration. On examination, she was pale, hypotensive and had tachycardia. Her growth parameters were appropriate for age and gender. The spleen was palpable 4 cm below costal margin with neither hepatomegaly nor ascites. The rest of her systemic examination was within normal. Her blood pressure was initially managed by fluid boluses. She was found to be anemic (hemoglobin, 6.6 g/dL) so received blood transfusion. She had no history of bruising or petechia with no family history of liver, rheumatological or hematological diseases.
After the initial stabilization, a limited emergency abdominal Doppler ultrasound was performed but came to be suboptimal with unremarkable findings apart from an enlarged spleen and no evidence of portal hypertension. Investigations showed leukocytosis with bandemia, microcytic hypochromic anemia and thrombocytopenia (hemoglobin, 6.6 g/dL; white blood cell count, 20,800/mm3; platelets count, 129×103/µL, 48% polymorphs, 25% band cells, 20% lymphocytes, 5% monocytes). C-reactive protein was 4.8 mg/L and erythrocyte sedimentation rate 7 mm/hour. Serum albumin was 2.9 g/dL and total protein was 4.9 g/dL with normal bilirubin and liver enzymes. Blood gas, renal function test, serum electrolytes, coagulation profile and lactate were within normal with negative blood culture.
Regarding her perinatal history, she was a product of full term uneventful pregnancy with normal vaginal delivery. Significantly, at the age of six days of life, she presented to the hospital with sepsis-like symptoms in form of fever, lethargy and a decreased oral intake. Investigations confirmed the presence of multiple hepatic micro-abscesses and neonatal sepsis. Her blood culture identified the presence of methicillin-resistant Staphylococcus aureus (MRSA) bacteremia with negative cerebrospinal fluid culture. During her neonatal admission period, no umbilical vein catheter was inserted. Also, she did not undergo any abdominal surgeries nor had a postnatal history of necrotizing enterocolitis. The patient was managed by intravenous antibiotics, and her serial abdominal sonographic studies revealed a full resolution of her hepatic micro-abscesses within forty days.
The patient was admitted to the pediatric intensive care unit and started on somatostatin analogue (octreotide) as (1 µg/kg/hour) and intravenous antibiotics. After stabilizing the patient, an upper gastrointestinal (GI) endoscopy was done that showed two esophageal varices of grade II, first one seen at 10 o'clock position at level of 13 cm extending to the level of 16 cm. Second one was seen at 12 o'clock position extending from the level of 15 cm to the gastroesophageal junction at the level of 21 cm, with no gastric or duodenal varices (Figs. 1 and 2).
 | Fig. 1Endoscopic view of grade II esophageal varices. An endoscopic view of the two esophageal varices, both of grade II, first one at 10 o'clock position, and second one was seen at 12 o'clock position.
|
 | Fig. 2Endoscopic view of grade II esophageal varices. An endoscopic view of the second esophageal varices at 12 o'clock position which extends from the level of 15 cm to the gastroesophageal junction at the level of 21 cm.
|
Both varices underwent injection sclerotherapy using ethanolamine oleate 5% agent. Later on, ultrasound Doppler of liver and portal vein system has been repeated which came to be suggestive of an old portal vein obstruction, however acute portal vein thrombosis couldn't be ruled out. Computed tomography (CT) angiogram of the abdomen was performed and showed a cavernous transformation of the portal vein which was poorly visualized starting from the confluence, instead it was replaced by multiple collaterals in the portohepatic and peripancreatic areas. Multiple collaterals were also noted within pericholecystic and gastrohepatic ligament areas. Splenomegaly and minimal ascites were noted also (Fig. 3).
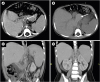 | Fig. 3CT angiogram. (A) Contrast enhanced axial CT scan of the abdomen showing dilated tortious vessels at the porta-hepatis and peripancreatic areas (arrow), in keeping with cavernous transformation of portal vein caused by portal hypertension. (B) Non-enhanced axial CT scan of the abdomen showing hypertrophy of the caudate lobe (arrow). (C) Contrast enhanced coronal CT scan of the abdomen showing splenomegaly and (D) minimal ascites at the sub-hepatic region.CT: computed tomography.
|
The patient was discharged after full resolution of her upper GI bleeding episodes and normalization of her laboratory investigations. Two weeks later, a follow up upper GI endoscopy was performed and showed that the old esophageal varices became smaller in size, grade I to II, with no new active lesions, so an elective injection sclerotherapy was done accordingly. Currently, the patient is asymptomatic and not receiving any medications. It's worth mentioning that the report had been ethically approved by the ethical committee at Imam Abdulrahman Bin Faisal University, Dammam, and an informed consent from the patient's guardian was obtained.
DISCUSSION
Pediatric portal hypertension is a serious emergency with various causes in literature. Its etiologies vary according to the age group. In neonates, umbilical vein catheterization and sepsis are the commonest causes implicated [6]. In our case, there were no history of umbilical vein catheterization, necrotizing enterocolitis, or abdominal surgeries, but the child did have blood culture proven MRSA neonatal sepsis and multiple small liver abscesses during her neonatal period at the 6th day of life. It was unclear whether sepsis caused the hepatic abscesses in our patient or vice versa, although she was having hepatomegaly at her neonatal presentation. The hepatic micro-abscesses were confirmed on ultrasound and the neonate showed complete resolution of her hepatic lesions by the age of 45 days following use of intravenous antibiotics namely; linezolid.
Portal vein thrombosis is rarely reported as an acute complication of neonatal hepatic abscess [346]. However, there were no reported cases of pediatric portal hypertension as a consequence of a chronic complication of neonatal hepatic abscesses in the literature like in our patient. In neonates, hepatic abscess is a rare disorder with less than 100 cases reported worldwide [1234567]. Mortality rate over 50% in neonatal hepatic abscess has been reported [8]. Predisposing factors for development of neonatal hepatic abscess include blood culture proven sepsis, umbilical catheterization, necrotizing enterocolitis, surgery and prematurity [7]. Therefore, we can conclude that umbilical vein catheterization and sepsis would be the commonest causes of liver abscesses leading to portal vein thrombosis. Up to our knowledge, by reviewing the literature our patient is the only reported case with such delayed onset of portal hypertension after a confirmed neonatal sepsis and hepatic abscesses of almost one year prior to her current presentation.
Chronic portal vein thrombosis or classically referred to as EHPVO in children is characterized by the formation of collateral vessels that bridge the obstruction and cause the appearance of the so-called portal cavernoma [9]. In our case, cavernous transformation of the portal vein was noted by CT angiogram of the abdomen, with no acute portal vein thrombosis, and the portal hypertension was manifested by caudate and quadrate hypertrophy, splenomegaly and minimal ascites.
EHPVO can be acute or chronic and is frequently diagnosed after first episode of variceal bleeding representing one of the most frequent causes of portal hypertension in pediatric patients [9]. The acute form usually manifests as a sudden onset of abdominal pain. On physical examination, most patients will exhibit splenomegaly, but ascites is usually absent [10]. Chronic portal vein thrombosis or EHPVO can present with portal hypertension related complications like variceal bleed, splenomegaly, thrombocytopenia and anemia or may be asymptomatic that can be incidentally found following an imaging procedure [11]. The most common presentation in children is a recurrent upper GI bleeding inform of hematemesis, melena or both [12]. Transient ascites is seen in almost one fifth of children following the episode of variceal bleed. Splenomegaly is almost universal and may transiently reduce during episodes of acute variceal bleed because of the partially relieved portal pressure with the active bleeding episodes [1314]. Hypersplenism is seen in up to one third of patients and is usually asymptomatic [13].
Despite that bleeding from ruptured gastroesophageal varices is considered as a serious emergency and the leading cause of death in children with EHPVO, till date, there is a lack of randomized controlled trials in the pediatric age group comparing different modalities of management for bleeding esophageal varices [14]. The current treatment options include medications such as: vasopressin and somatostatin and their analogues, endoscopy, surgery, and transjugular intrahepatic portosystemic shunting. Depends upon their relative efficacy, safety, and cost considerations, the choice of one modality over another is established with none of the existing modalities come close to being ideal for pediatric age group. Intravenous vasopressin reduces portal pressures by directly constricting mesenteric arterioles and decreases portal venous inflow. However, it was found that it enhances mortality due to extrasplanchnic vasoconstrictive properties and resultant myocardial, cerebral, bowel, and limb ischemia [15]. Because of such side effects, vasopressin should be given with caution in children. Somatostatin inhibits the release of vasodilator hormones such as glucagon, indirectly causing splanchnic vasoconstriction and decreased portal inflow [16]. Octreotide is a long-acting analogue of somatostatin. In a meta-analysis comparing somatostatin versus vasopressin by Imperiale et al. [17], somatostatin was found more effective for controlling bleeding than placebo or vasopressin and had fewer side effects, therefore it replaced vasopressin as the pharmacologic treatment of choice for active variceal bleeding. In our case, the patient was started on octreotide with no reported complications noted.
Regarding the non-medical modalities of management, endoscopic variceal ligation (EVL) has become the procedure of choice for managing variceal bleeding in children because it is a safe with lower risk of complications and effective with shorter interval time to varices eradication, requiring lower number of sessions with lower rebleeding incidence [18]. EVL may, however, be technically difficult in infants, and injection sclerotherapy is the recommended alternative approach in such cases [19]. In one pediatric study series of 169 cases of EHPVO, El-Karaksy et al. [14] reported that injection sclerotherapy was effective in eradication of varices in their population of pediatric patients and was completed without being affected by the grade of varices. In the same series, they found that recurrence occurred only in 4 cases within few months suggesting that injection sclerotherapy was more associated with the development of secondary varices than EVL. In our patient, injection sclerotherapy was effective in cessation of visceral bleeding after the first session, but it did not completely eradicate the varices which require another session of injection sclerotherapy with follow up endoscopy.
Studies in adults' population recommend the use of nonselective β-blockers for primary and secondary prophylaxis of variceal bleeding [20]. However, the long-term use of such agents cannot be recommended in children due to the lack of sufficient data as these agents can block the physiological compensatory mechanism for hypervolemia when bleeding occurs [19].
We conclude that pediatric portal hypertension with EHPVO can be of a delayed onset presentation. Thorough history including antenatal, perinatal and neonatal history and physical examination is a cornerstone step in identifying the underling predisposing factors for such pathology. Neonatal sepsis continues to be one of the commonest risk factors for portal vein thrombosis in pediatric age group, along with the proposed entity of neonatal hepatic abscess as a recently recognized under-reported predisposing factor. A high index of suspicion should be raised when portal hypertension is suspected even with a suboptimal Doppler ultrasound imaging. By reviewing the literature, our case represents one of the most delayed onset presentations of pediatric portal hypertension secondary to EHPVO due to hepatic abscess versus neonatal sepsis of almost one-year duration.
 XML Download
XML Download