

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Percutaneous liver biopsy (PLB) is the definitive procedure for the diagnosis of a variety of hepatobiliary disorders providing high diagnostic yield and generally low complication rates in children [12]. Increasingly, the procedure is performed with ultrasound guidance in an outpatient setting with local anesthesia and moderate sedation [34567]. Post-procedural monitoring includes assurance of anesthetic recovery, adequate pain control, and observation for known procedural related complications [8910]. The incidence of PLB-related complications varies by definition and has been reported between 0% to 15.2% [12311121314151617181920]. Complications range in severity from minor problems such as abdominal pain and transient hypotension to severe complications including hemorrhage requiring transfusion, pneumothorax, hemothorax, intestinal perforation, biliary leak, or hemobilia.
There is a growing body of literature suggesting lower complication rates using ultrasonography in biopsies performed in children [123131415161718]. Although the greatest risk of bleeding occurs within the first few hours after biopsy, the optimal length of observation to mitigate delayed complications after PLB has not been established [12391221]. The American Association for the Study of Liver Diseases provided guidelines recommending a 2- to 4-hour observation period after PLB for adults undergoing outpatient biopsy [22122]. However, current guidelines permit significant variability regarding recovery duration after biopsy for children [811]. For children undergoing PLB, the absence of contemporaneous cohort comparative data to define ideal monitoring periods has led to variability in recovery practice largely dictated by provider comfort or institutional preference [23].
In our center, the choice of post-PLB monitoring duration is determined prior to procedure and varies by operator preference. We aim to determine if differences exist in the frequency of procedural complications, unplanned admission rate, and total cost for children undergoing ultrasound-guided, outpatient PLB selected for either same-day (≤8 hours) or overnight observation. We hypothesize the complication and unplanned admission rates will be similarly low for both cohorts, but encounter costs will be greater in those with extended observation.
MATERIALS AND METHODS
Study design and setting
We performed a retrospective cohort study in children aged 1-month to 17-years undergoing ultrasound-guided PLB at Johns Hopkins All Children's Hospital from January 2009 to August 2017. Johns Hopkins All Children's Hospital is a 259-bed, free-standing, tertiary care, pediatric referral center with an outpatient surgical day center located on premises. We included only outpatient PLB performed by pediatric gastroenterologists in our surgical day center and excluded those children already hospitalized or PLB performed by interventional radiologists. This research was reviewed and approved by our Institutional Review Board (Johns Hopkins Medicine IRB #00124026).
Case identification, definitions, and study outcomes
Subjects were identified for study by review of the electronic health record using the Johns Hopkins All Children's Hospital Health Informatics Core. Cohorts were defined by the duration of operator pre-selected recovery period: same-day (≤8 hours) vs. overnight. Primary outcomes were surgical complications (surgical site hemorrhage necessitating blood product transfusion, hypotension or hypoperfusion requiring isotonic fluid bolus administration, peak postoperative Wong-Baker pain rating [24], and frequency of bolus narcotic analgesia), unscheduled hospitalization within 7 days post-PLB, and total encounter costs. Aggregate hospital cost data were acquired from an independent hospital billing database and directly obtained via cost-accounted methodology [25]. Demographics, anthropometrics, comorbidities, indication for PLB, general patient outcomes, and diagnostic PLB pathologic reports were obtained for additional sample characterization.
Procedural technique, standard anesthetic, and post-procedural recovery
During the study period, PLB were performed by three pediatric gastroenterologists in our institution. Biopsies were completed using ultrasonographic guidance using a right-sided intercostal or subcostal approach. All biopsies at our institution are completed with the Bard® Manopty® 18-gauge 20 cm disposable core biopsy instrument (Bard Medical, Covington, GA, USA). No more than two needle passes are performed per institution practice, and post-biopsy ultrasound obtained to evaluate for immediate surgical site bleeding. Pressure dressings are then applied, and patients instructed to lie in the right lateral decubitus position for 2 to 4 hours.
Children undergoing PLB in our institution receive deep sedation using total intravenous anesthetic (TIVA) with propofol [2627]. Total intravenous anesthesia using propofol for PLB takes into account potentially impaired hepatic synthetic function or altered drug metabolism associated with liver disease. Goals include maintenance of spontaneous respiration with supplemental oxygen therapy throughout procedure. Where appropriate, additional sedatives and analgesics are administered with opioid and non-opioid agents including remifentanil, dexmedetomidine, ketamine, and/or benzodiazepines. Acetaminophen and non-steroidal anti-inflammatory agents are typically avoided if there is concurrent hepatic insufficiency or renal insufficiency, respectively. It is uncommon in our institution for children undergoing outpatient PLB to require volatile anesthetic agents, neuromuscular blockade, or invasive ventilation unless TIVA is contraindicated, a higher degree of airway control is desired, or intraoperative events dictate more aggressive anesthetic plan.
Following the procedure, children are admitted for either same-day (≤8 hours) or overnight monitoring at the discretion of the operator. Immediately following PLB, patients are transferred to our post anesthesia care unit (PACU) where standard care includes cardiopulmonary monitoring, nursing to patient ratios of 1:1, and vital sign monitoring every 15 minutes. After recovery of cardiopulmonary and neurologic function, patients are transferred to a surgical extended care unit where nursing ratios are reduced to 1:4 and vital signs monitoring extended to 1-hour intervals. If selected for overnight observation, vital sign documentation is further extended to 4-hour intervals. Discharge orders are placed at the discretion of the operative provider but generally are predicated by a return to preoperative baseline cardiopulmonary-neurologic function, tolerance of oral nutrition, adequate pain control, stable hemoglobin (drawn 4-hours post procedure), and provision of anticipatory guidance.
Statistical plan
Descriptive data are reported throughout this manuscript as proportions, percentages, means±standard deviation, or medians (interquartile range [IQR]) depending on data variance and type. Comparative analyses including Student's t-test, Wilcoxon rank-sum test, or Fisher's exact test where appropriate. Type I error was set as 0.05. All statistical analyses were completed using Stata© ver. 15.1 software (StataCorp, College Station, TX, USA).
RESULTS
During the study period, a total of 112 children met inclusion criteria and underwent ultrasound-guided PLB. Within this sample, 18 (16.1%) children were assigned to ≤8-hour post-procedural observation and 94 (83.9%) overnight observation. Mean age was 10.5±6.3 years, weight 46.4±29.7 kg, and ratio of male to female was 1.6:1. The most common indications for biopsy were abnormal hepatic function tests (50%), infectious disease (16%), metabolic disease (15%), and autoimmune disease (9%). Children observed overnight were monitored for a mean of 23.1±5.2 hours and those in the same day cohort for 5.2±1.8 hours.
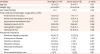
Demographics, anthropometrics, hematologic/coagulation profiles, and procedure indications are shown in Table 1 and divided by observation duration cohorts. Subjects in both cohorts did not differ with regards to age, weight, gender, or preoperative comorbidities including hematologic and coagulation parameters. The indications for PLB were observed with comparable frequency in both cohorts.
Table 1
Sample characteristics including demographics, anthropometrics, hematologic profile, and procedure indication for children with same-day vs. overnight observation
![]()
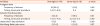
General patient outcomes and procedural outcomes data can be found in Table 2. Groups did not differ with respect to frequency of analgesia administration, isotonic fluid boluses, blood product transfusions, unplanned hospital readmissions, or peak Wong-Baker pain ratings. No child was unexpectedly admitted within 7 days following PLB for any indication or required blood product transfusion during or after procedure. Two children received prophylactic fresh frozen plasma immediately prior to procedure. While 23% of the sample received an analgesic bolus during post-PLB monitoring, all doses were administered within 8 hours of biopsy. Similarly, only 5% of subjects required bolus isotonic fluids that were all administered within 5 hours of procedure. No children experienced severe PLB-related complications including intestinal perforation, blood product transfusion, hemobilia, mortality, pneumothorax, hemothorax, or surgical site infection.
Table 2
Postprocedural outcomes following percutaneous liver biopsy for children with same-day vs. overnight observation
![]()
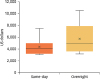
Compared to children in the overnight monitoring cohort, the same-day cohort accrued less total encounter costs (median of US $4,224 [IQR, 3,611–5,068] vs. US $5,216 [IQR, 4,541–6,274], p<0.05, Fig. 1). The median absolute cost difference was US $992 per subject and if applied to the entire study sample, nearly US $100,000 of potential savings was noted.
DISCUSSION
In this single-center, retrospective cohort study comparing same-day vs. overnight extended monitoring after PLB, we observed no major complications or post-operative blood product transfusions during either recovery period. Rates of analgesia administration, isotonic volume boluses, unplanned hospital readmissions, and pain severity scores did not differ for either group. There was, however, an attributable median cost of US $992 per patient for children monitored overnight compared to same-day observation. Our data add to existing adult [22] and a growing body of pediatric literature [13] that reinforces the relative safety of ultrasound-guided PLB and a potential to yield a substantial economic impact by embracing same-day monitoring as standard practice for children without major comorbidities. Taken in sum, these data may assist in the development of pediatric guidelines for post PLB management including identification of ideal recovery durations and setting.
The selection of a particular degree and duration of post-procedural monitoring is multifactorial but certainly includes a thoughtful consideration of patient context, comorbidities, known incidence and severity of procedure-related complications, satisfactory anesthetic-related recovery time, and flexibility for emergent intraoperative factors [910]. In general, complications related to PLB in relatively healthy patients are rare and include minor complications such as localized pain, fever, hypotension, or major complications such as bleeding, arteriovenous fistula formation, pneumothorax, hemothorax, organ perforation, biliary leak, and surgical site infection. While the exact frequency of procedure-related complications may vary by operator, technique, and underlying patient comorbidity, existing literature suggests that if complications do occur, they generally present early within the post PLB recovery period. Among 626 children undergoing outpatient PLB, Bolia et al. [3] noted most complications occurred within 8 hours of procedure. Similar findings were noted by Gonzalez-Vallina et al. [4], Scheimann et al. [16], and Almeida et al. [28], where complications were observed within 2 to 8 hours of biopsy. Our findings complement these descriptive series as we observed all interventions and minor complications within 8 hours in our sample of patients.
Many children undergoing PLB have uncertain hepatic function or coexisting coagulopathy. Therefore, specific focus has been placed in understanding the risk and potential mitigating factors relating to clinically important postoperative bleeding. Bleeding after PLB is more commonly observed for cases where surgical indication is biopsy of a hepatic mass lesion or if completed in the presence of concurrent anticoagulant therapy [1229]. In a retrospective review of 228 inpatient pediatric PLBs, no major bleeding complications were noted in children with international normalized ratio (INR) >1.5 or platelet counts <60,000/μL [1]. The same study noted only minor bleeding complications (incidence of 11.8%). Not surprisingly, they found an increasing number of needle passes was an independent risk factor for minor surgical site bleeding. After reducing institutional preoperative platelet and INR goals to ≥50,000/μL and ≤2.0, Kitchin et al. [30] noted no increase in post-procedural bleeding in a pre-post analysis. Not surprisingly, they did note a significant reduction in use of preoperative blood product transfusion. While an individual's bleeding risk does not appear to correlate with coagulation parameters, neither does mitigation of risk by perioperative transfusion of fresh frozen plasma or platelets. Nearly our entire cohort was without preexisting coagulopathy and, therefore, may have been considered “low-risk” for surgical site bleeding. The European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHN) guidelines state correlations between coagulation-parameters and bleeding risk are of low-evidence and require reassessment [11]. ESPGHN still recommends preoperative coagulation testing and preoperative coagulation goals of an INR <1.5 and platelet count >60,000/μL. A majority of our cohort met these criteria without transfusion and only two patients, with comorbid oncologic disease, received prophylactic fresh frozen plasma transfusion prior to biopsy.
Key components to post-procedure monitoring include time for anesthetic recovery and provision of adequate analgesia [10]. The recovery of pediatric patients after anesthesia requires skilled staff that may not be available at every institution or outpatient setting. Goals of PLB anesthetic are minimalistic with selection of the lowest drug dose required to achieve a therapeutic effect to reduce pain and discomfort, control anxiety or psychological trauma, decrease patient movement to ensure safe completion of procedure, and achieve recovery to a preoperative baseline state of consciousness and cardiopulmonary-neurologic function. After receiving a combination of TIVA and analgesics, children with hepatic dysfunction may experience known adverse events that necessitate intervention including apnea, airway obstruction, laryngospasm, allergic reaction, emergence delirium, hypotension, or inadequate perfusion [3132]. In addition, children given propofol are monitored for development of propofol infusion syndrome, a condition classically seen in prolonged drug exposure (>24 hours) or existing renal dysfunction [33]. Children with hepatic dysfunction and associated coagulopathy, encephalopathy, renal dysfunction, systemic complications of autoimmune disease, or morbidity associated with nutritional deficiencies may be at higher risk for developing anesthesia related complications. Therefore, a targeted history and assessment of anesthetic plan could assist in dictating the degree and duration of postoperative monitoring.
Increased monitoring duration may diminish the repercussions of missed late procedural or anesthetic complications. However, prolonged monitoring may result in harm associated with persistent exposure to the healthcare environment. Longer monitoring may increase parental stress, decrease satisfaction [3435], or result in health-care-acquired conditions such as infections, adverse drug events, and risk of medical error [36]. Prior to discharge, families should receive education regarding PLB-related complications and be provided with appropriate anticipatory guidance. The degree to which a family may reliably receive emergency care and office reassessment in the case of an acute complication must be assessed by providers prior to discharge.
We noted a small, but cumulatively large degree of potential savings when comparing total costs of same-day vs. overnight monitoring (nearly US $1,000 per encounter). This is most likely due to direct charges associated with prolonged monitoring period. While cost is an important healthcare outcome, even one missed major complication could easily account for a sizable portion of any potential savings by altering our institutional practice from overnight to same-day observation. It is encouraging that we observed no major complications, unexpected admissions for late or missed complications after discharge, and only early, isolated minor interventions over the entire 9-year period in all children undergoing PLB.
This study has some limitations. This study assessed PLB performed by pediatric gastroenterologists and not those completed by other surgical team members or interventional radiologists. While we cannot assume similar skill levels between providers and differentially-associated complication rates, if PLB are performed in a similar setting and set of indications, it is likely our findings can be generalized. All subjects represented outpatient procedures and we cannot conclude similar findings in children admitted to the hospital who may require longer postprocedural monitoring due to concurrent illness, severity of illness, or other comorbidities. Careful consideration must be given to providers who do not routinely use ultrasonography for PLB. Additionally, we cannot comment on risk associated with varying biopsy needles other than those described in our study. Cost may vary by institution and regional billing practices. Data assessed in our study represent direct costs obtained by cost-accounting methodology. Our financial assessment likely represents a more realistic and precise estimation of healthcare expenditure for payers and families rather than those calculated by cost to charge ratios or charge data alone. Although this study was a single-center experience, it may be generalizable to other stand-alone, tertiary care, pediatric referral centers where PLB are routinely performed. None of our patients represented acute hepatic organ transplantation, therefore we cannot comment on safety in that specific patient population. However, existing data for PLB in children who received hepatic transplant are comparable to our findings [17]. Additionally, hospital resources such as ability to recover in PACU and extended hours impact ability to safely monitor and recover patients in centers without pediatric expertise.
In conclusion, same-day observation after PLB in the outpatient pediatric population without significant comorbidities appears well-tolerated without incidence of major complications. Children who required minor interventions such as fluid bolus or analgesic administration did so well within an 8-hour recovery period regardless of observation duration. These findings from our sample of outpatient PLB performed at our institution over a 9-year period are consistent with other single-center descriptive studies. Our results back the standard of same day observation in otherwise low-risk children undergoing outpatient PLB. We recommend pre-surgical, targeted historical review to identify children at risk for postoperative complications including existing comorbidities, assessment of previous anesthetic complications, existing airway anomalies, known severe coagulopathy, and any baseline cardiopulmonary or neurologic dysfunction.
 XML Download
XML Download