

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Crohn's disease (CD) is a chronic inflammatory condition that can occur anywhere in the gastrointestinal tract. It has been recognized as an important disease entity mainly in North America and Northern Europe, including the United Kingdom and Norway. Recently, however, the incidence has increased markedly in Asia, including Korea [12]. It is known that 25% to 30% of all cases of CD occur in children <19 years of age. Pediatric CD has a higher association with family history and greater small bowel involvement than in adults; the recurrence rate and number of operations have also been reported to be high [345]. The cumulative incidence of surgery for pediatric CD has been reported to be 20% at 3 years and 34% at 5 years from diagnosis [67]. Therefore, aggressive treatment is needed for pediatric patients with CD because it directly impacts growth, especially height and weight [89].
In 1998, infliximab, a monoclonal antibody to tumor necrosis factor-alpha (TNF-α), was introduced. Thereafter, biological therapy became available for clinical use, leading to the remission and maintenance of CD through intestinal mucosal healing [101112]. Previous studies have reported that biologics are beneficial to growth (i.e., height and weight), especially in adolescent patients with CD [891314]. However, their effect on reducing the rate of surgical intervention remains debatable [151617]. Therefore, this study aimed to analyze the effects of biologics on growth and prognosis related to surgery in children and adolescents with CD.
MATERIALS AND METHODS
Study population
A retrospective cohort study involving patients aged <19 years diagnosed with CD at the Seoul National University Children's Hospital (Seoul, Korea) between January 2006 and October 2017 was performed. Clinical features of patients and the disease course according to the use of biologics were analyzed. CD was diagnosed according to clinical, endoscopic, radiological, and pathological findings, excluding congenital autoimmune diseases and other intestinal diseases involving other organs. The “accelerated step up” strategy was used [18]. To treat patients, steroid therapy was used first, followed by the simultaneous administration of azathioprine. Biologics were used in patients with no initial steroid response or with steroid dependency. Moderate or active CD unresponsive to more than 1 universal treatments, such as corticosteroid and immunomodulator treatment, untreated perianal disease, CD with a pediatric CD activity index (PCDAI) score of >30, or contraindications to such treatments were indications for the use of biologics according to the Health Insurance Review & Assessment Service in our hospital. Infliximab was administered at 0, 2, and 4 weeks and every 8 weeks thereafter at 5 mg/kg/day, and clinical courses were evaluated. Dose intensification with interval shortening was applied at intervals of up to every 4 weeks when patients exhibited unresponsiveness or flaring with infliximab treatment.
The present study was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB No. 1810-129-982).
Description of variables
Clinical features of patients with CD during a 12-year period were investigated and compared among those who were treated with biologics and those who were not. Additionally, the frequency of operation(s), divided into 9 groups according to the surgical site, was also analyzed. Clinical features of patients who underwent procedure(s) were investigated according to the type of surgery. Surgical treatment was limited to operations related to CD throughout the gastrointestinal tract. The association of the use of biologics with growth (i.e., height and weight [body mass index; BMI]) was analyzed. Retrospective comparison according to outcomes was performed. Finally, surgical outcomes were analyzed. The time from diagnosis to operation, time from first operation to second operation, and total number of operations were analyzed to compare the effectiveness of biologics. The types of operations were divided into those involving the perianal area and those not involving the perianal area.
Statistical methods
Z-scores for height and BMI were calculated using the Zanthro package and STATA version 14 (StataCorp, College Station, TX, USA) based on 2006 World Health Organization (WHO) growth standards and 2007 WHO growth chart references [1920]. The Student's t-test was used to compare height and weight z-scores in the biological- and non-biological treatment groups. The cumulative operation and recurrence rates were calculated by retrospective cohort analysis using the Kaplan-Meier method. Differences with p<0.05 were considered statistically significant. Cox hazard regression analysis was used to calculate hazard ratios with stratification based on the initial PCDAI score [21]. Statistical analysis was performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Clinical features of children and adolescents with CD
A total of 173 patients were enrolled, of whom 65 underwent surgical procedures and 108 who did not (Table 1). The number of males was 1.7 times higher than females (110 male and 63 female). The mean (±standard deviation) age at diagnosis was 12.25±3.2 years and mean PCDAI score was 36.7±12.7. biologics were used in 121 (70%) patients. Paris classification was observed with the following distribution: L1 (8.6%), L2 (13.3%), L3 (58.9%), L4 (1.7%), and P (17.3%).
Table 1
Baseline characteristics of the patients

Values are presented as mean±standard deviation or number (%).
M: male, F: female, PCDAI, pediatric Crohn's disease activity index.
![]()
The rates of use of biologics were similar between the operated and non-operated patients: 46 of 65 (70.8%) patients underwent operation and 75 of 108 (69.5%) did not. The sex ratio was 1.7 in the biologics group and 2.8 in the non-biologics group among the operated patients (Table 2). The mean age at diagnosis was 12.58 years for the biologics group and 11.3 years for the non-biologics group, and the PCDAI scores were 38.4 and 36.9 in the biologic and non-biologic groups, respectively, in the operated group. The mean number of operations per patient was 1.89, and most patients underwent more than 1 operation. The mean time from initial diagnosis to surgery was 19.3 months. The sex ratio, mean age at diagnosis, PCDAI score, and mean age at operation of patients in the biologic and non-biologic groups among the non-operated patients were not statistically different.
Table 2
Baseline characteristics of patients according to treatment with biologics

Values are presented as mean±standard deviation or number (%).
OP: operation, M: male, F: female, PCDAI, pediatric Crohn's disease activity index.
![]()
Clinical features according to type of surgery
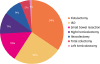
When operation rates according to surgery type were analyzed, the most common operation was fistulectomy (34%), followed by incision and drainage (I&D) (25%), small bowel resection (15%), right hemicolectomy (11%), ileocolectomy (9%), and total colectomy (5%) (Fig. 1). Perianal operation accounted for more than one-half of the cases (59%). Patients were classified according to whether they underwent operation, and their clinical features were analyzed. The mean age at diagnosis was 12.05 years, and most operations were performed at the age of 11–13 years. Mean age at total colectomy was 7.5 years and that at left hemicolectomy was 1.8 years, and these mean ages were relatively lesser than those for other types of operations. The mean number of hospital admissions per patient was the highest for total colectomy (14 admissions), followed by left hemicolectomy (9.7 admissions) and right hemicolectomy (7.3 admissions). Comparing the number of hospitalizations, total colectomy and left hemicolectomy were the most common (14 cases), followed by 9.7 cases of right hemicolectomy, and 9.3 cases of I&D. Preoperative biologics were used in 50% of patients who underwent I&D, 40% of those who underwent small bowel resection, and 27% of those undergoing fistulectomy. However, biologics were not used in patients undergoing total colectomy or left hemicolectomy.
Growth differences according to the use/non-use of biologics
Up to the end of the study in October 2017, there were 143 patients with reliable height and weight data; of these, 50 underwent operation and 93 did not. Among the 50 patients who underwent operation, 23 (mean age, 12.6 years) underwent perianal procedures and 17 (mean age, 12.2 years) underwent non-perianal procedures. The follow-up period was 7.2±4.1 years for patients using biologics and 4.4±2.9 years for those not using these agents (p=0.00). The mean initial erythrocyte sedimentation rate (ESR) was 52.6±32.3 mm/h in the biologics group and 37.3±28.0 mm/h in the non-biologics group (p=0.09). There was no statistical difference in ESR during follow-up between the 2 groups. Initial C-reactive protein (CRP) levels of patients was 4.9±6.5 mg/dL in the biologics group and 3.5±3.9 mg/dL in the non-biologics group, but the difference was not statistically significant. There were also no significant differences in CRP levels between the groups during follow-up.
The use of biologics increased the z-score for height (p=0.002) and BMI (p=0.005) (Fig. 2) in all patients. Additionally, in the operated group, the use of biologics increased the z-score for height (p=0.004) and BMI (p=0.048) during follow-up periods (p=0.04). In perianal lesions of patients who underwent surgery, biologics increased only the height z-scores (p=0.031). In contrast, only BMI was increased in those who underwent non-perianal procedures (p=0.001). In the non-operated group, there was no significant difference in height (p=0.06) or BMI (p=0.07) z-score between biologic- and non-biologic-treated patients. Instead, in non-operated patients, there was significant difference in the PCDAI scores between those undergoing biologic treatment and those who did not (Table 2). Patients undergoing biologic treatment demonstrated higher mean PCDAI scores (37.9) compared with those not treated with biologics (31.6) (p=0.01).
 | Fig. 2Box and Whisker plots of differences in height and BMI z-scores from diagnosis to follow-up according to the use of biologics. Height and BMI z-scores from diagnosis to October 2017 according to the use of biologics in all patients (A); in total operated patients (B); in perianal lesion operated patients (C); in non-perianal lesion operated patients (D); and in non-operated patients (E).BMI: body mass index.
|
Comparison of surgical outcomes according to biologic status
Among 173 patients, 11 who were treated with biologics at the same time as the operation were excluded. The time from diagnosis to the first operation was defined as free from surgery and the biologics-treated group was compared with the untreated group.
In all patients, the free from surgery curve of the non-biologic group decreased considerably compared with that of the biologic group as time passed in the Kaplan-Meier curve analysis (p=0.000). The biologics group exhibited a 0.27-fold greater hazard for duration of free from surgery compared with the non-biologics group among non-operated patients.
Among operated patients, the free from surgery curve according to the use of biologics was not statistically different (p=0.198) (Fig. 3). The time to free from surgery was not affected by the use of biologics in the group that underwent perianal procedures (p=0.078) or those who did not (p=0.294). However, within 2 years in perianal procedure group, free from surgery was significantly prolonged in the biologics group; however, there was no difference thereafter (p=0.013) (Fig. 3, Table 3). The recurrence interval was defined as the period from the first operation to the second operation in patients who underwent ≥2 reoperations. There was no difference in the recurrence interval, the number of the total operations between the groups using/not using biologics. Among non-perianal surgery patients, the use of biologics did not prolong the time from diagnosis to operation, the interval from first surgery to second surgery, or the number of total operations.
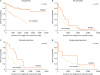 | Fig. 3Cumulative operation rate in the operation group. Kaplan-Meier statistics comparing the duration from diagnosis to operation according to the use of biologics. Cumulative operation rates are shown in all patients (A); in all patients in the operation group (B); in the perianal lesion operated group (C); and in the non-perianal lesion operated group (D).
|
Table 3
Cox hazards regression model for free from surgery according to the use of biologics
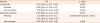
Biologics group showed a 0.27-fold greater hazard of duration of free from surgery compared to non-biologics group in non-operation patients. Biologics showed 0.12-fold greater hazard in non-perianal operated group. In perianal operated patients, p-value was 0.078, but within 2 years p-value was 0.013 and 0.25-fold HR.
HR: hazard ratio, CI: confidence interval.
![]()
DISCUSSION
CD follows a chronic, progressive course in which many patients are complicated and require surgical intervention(s). Since the 1990s, the number of patients with CD has increased in Asia, including in Korea, and the incidence in children has increased worldwide [12]. The prognosis of CD varies depending on the site of the lesion(s), severity, and accompanying complications. Generally, the younger the age at onset, the worse the prognosis and the higher the probability of requiring surgical intervention(s).
The sex ratio of patients with CD was 1.7:1 in this study, similar to the 1.8:1 ratio reported in previous Western studies. Male predominance in CD is common worldwide [22]. In our study, the mean age at diagnosis was 12 years and that at operation was 13.6 years, which were younger than the mean ages reported in the West [22]. In our series, the mean PCDAI score at diagnosis was 36.7, indicating that many of our patients had severe disease at their initial presentation. Among patients who underwent surgery for CD, the mean age at operation was 12 years. The duration from diagnosis to operation was 19 months, which is shorter than that in adult patients in whom the operation rate has been reported to be 28% over the 5 years [23]. There was no difference in the sex ratio, age at diagnosis, and PCDAI scores between the biologics and non-biologics groups. According to the type of procedure, fistulectomy, I&D, and small bowel resection were frequently performed, and perianal procedures were the most common types of surgery. In non-perianal surgeries, small bowel resection was the most frequent operation, which is similar to the findings of previous studies [4]. Left and total hemicolectomy had a relatively younger age at diagnosis and operation compared with other operations; however, in our group, the early use of preoperative biologics was rare.
In addition to general clinical symptoms, such as abdominal pain, diarrhea and weight loss, children with CD exhibit growth retardation and delayed puberty [2425]. Because growth in children during the disease course is an important treatment target, height and weight should be considered important treatment outcomes. Anti-TNF-α antibodies are known to prevent further loss of height during the course of the disease through remission of the inflammatory process [13262728]. During the follow-up period in our study, biologics in the operation group significantly increased height and BMI z-scores compared with the non-biologics group (p=0.04). In the perianal operation group, only the height z-score increased (p=0.031). We found differences in the time from diagnosis to the use of biologics in both groups: 541 days for patients undergoing perianal procedures and 801 days for those undergoing non-perianal procedures (p=0.042). It is likely that patients who underwent perianal procedures tended to use biologics earlier due to overt clinical symptoms, and height and weight may have “recovered” after inflammation was controlled [142729]. In the non-perianal operated group, treatment with biologics could not affect height; however, it is believed that BMI improved because disease was controlled by the operation and nutritional status was restored, even though biologics could not be used earlier. In contrast, in the non-operated group, there was no difference in height and BMI z-scores according to the use of biologics. When we analyzed the PCDAI scores of non-operated patients, those in the biologic group had higher scores than those in the non-biologic group (37.9 and 31.6, respectively) (p=0.01). In the non-operation group, symptoms might be well controlled with immunomodulators alone, including azathioprine, and height and weight could not be significantly different between the biologics and non-biologics groups.
The initial ESR was high and the follow-up period was long in the group using biologics. This implied that patients with severe disease were selected for biological treatment. There were no significant differences in CRP and ESR changes during the follow-up periods between the 2 groups. Nonetheless, because of the significantly higher changes in height and weight z-scores among patients using biologics, biologics are believed to help height and weight growth in patients with high disease severity.
There are many opinions regarding the relationship between biologics and surgical intervention(s). A recent study by Appau et al. [30] found an association between preoperative infliximab therapy for CD and postoperative complications. Additionally, another study reported that infliximab therapy did not supplant the need for surgical intervention in the majority of patients with fistulizing CD [16]. In contrast, yet another study found that infliximab treatment had the potential to extend the time to the first surgery [31]. In this study, biologic therapy could prolong the duration of free from surgery within 2 years in patients with perianal lesions, which accounted for >50%, although the frequency and recurrence of surgery were not prevented. Therefore, the use of biologics at the appropriate time period is important, especially in patients with severe perianal lesions. In our study, the early use of biologics in patients with CD with perianal lesions had the effect of growth in height and prolonging the duration of free from surgery.
These results suggest that the use of biologics based on the PCDAI scores reduces the possibility of surgery. However, the use of biologics based on the PCDAI scores alone would result in poorly treated patients not receiving appropriate treatment, resulting in an increased probability of operation. Guidelines are, therefore, needed to enable the early use of biologics in a timely manner, with clearer standards for high-risk groups. Finally, in the subgroup analysis of patients undergoing surgery, the first 2 years appeared to delay the onset of surgery, which is considered an important time for growth. Therefore, improved screening of high-risk patients and early use of biologics are very important.
There were some limitations to this study. The present investigation was a retrospective cohort study. As such, it is difficult to generalize characteristics of patients with pediatric CD in Korea because due to the small number of patients studied; therefore, a larger-scale national study is needed. In this study, nutritional intervention was not performed; however, nutritional support has a significant effect on the course of CD [32]. As demonstrated in this study, the therapeutic effects of biologics vary according to the severity of disease, and detailed guidelines for treatment should be established according to clinical features and clinical course.
Based on this study, although biologics could not prevent operation rate, biological therapy delayed disease progression within two years after disease onset in pediatric CD patients who underwent surgery. Biologics could bring growth and BMI benefit in this window period. Therefore, it may be helpful for optimal growth to use biologics in pediatric patients with high probability of undergoing future surgery.
 XML Download
XML Download