

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Intestinal failure (IF) can be defined as a critical reduction of the gut mass or its function below the minimum needed to absorb nutrients and fluids required for adequate growth in children [1]. Severe IF, results in the need for parenteral nutrition (PN). The short bowel syndrome (SBS) is the leading cause of IF. IF may be reversible or irreversible, depending on a number of factors such as the underlying cause of SBS, the length of the remaining intestine or the treatment used to develop or restore intestinal capacity. Severe and even irreversible IF in children is very challenging. SBS being rare, there is not enough data to provide the scientific foundation needed to form treatment guidelines or for the creation of gold-standards for the care of such very specific patients. However, guidelines for PN may provide basic knowledge for the management of those complex patients [23]. Due to technical refinements and steady advances in the development of highly sophisticated nutrient solutions consisting of optimal combinations of macronutrients and micronutrients, PN plays an important role in patient management [23]. PN has become a safe and efficient feeding technique.
In clinical practice intestinal sufficiency, or insufficiency, may be indirectly measured by the level of PN required for normal or catch up growth [4]. Other indicators such as residual bowel length measured at last surgery and serum citrulline, though helpful, have not proven to be highly reliable prognostic factors in children with SBS [567]. PN dependency index, is the ratio of non-protein-energy intake provided by PN for achieving normal or catch up body weight gain and resting energy expenditure calculated by using the Schofield formula [48].
SBS-IF that requires long-term PN may be associated with various complications PN or IF related, including catheter-related blood infections (CRSBIs), small intestinal bacterial overgrowth (SIBO), growth failure, metabolic disorders, and bone disease [9]. Cholestatic liver disease (CLD) was rapidly identified as one of the limitations in the of long-term management of SBS-IF while CLD related factors are mostly related to IF rather PN supporting the wording “IF Associated Liver Disease” (IFALD) [10111213]. Severe liver disease may lead to the so-called “nutritional failure” which is considered as a major indication for intestinal transplantation (ITx) or combined liver-ITx [9].
DEFINITION AND ETIOLOGY OF THE SBS
SBS is, usually following extensive surgical resection leaving the small bowel (SB) length below a critical value for adequate nutritional supply. Severely reduced mucosal surface results in malabsorption with subsequent diarrhea, water-electrolytes imbalance, and malnutrition [19]. Exact measurement of the remnant intestine remains difficult even with the help of radiographic assessment [14]. At birth, term-neonates have a SB length of approximately 250 cm and their intestines lengthen substantially during the first year of life [15]. Preterm infants have a greater potential for bowel growth since their intestines lengthen substantially during the last trimester of gestation [16].
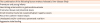
The cut-off length for SBS is related to a number of factors. In general, SBS occurs after a massive resection leaving less than 40 cm of viable SB. A residual bowel length of only 15–40 cm has been associated with bowel adaptation, intestinal autonomy and PN weaning, but, most of the time with few information regarding the long-term growth [171819202122232425]. Numerous factors determine SBS prognosis: the underlying diagnosis, the type of segments preserved, the presence of the ileo-caecal valve (ICV) and the colon, a long-term stoma vs. a primary anastomosis, the number of surgical procedures, as well as the age of the patient at the time of surgery [171819202122232425]. Classification of SBS in 3 type is helpful for the understanding of different outcomes (Fig. 1). Other factors are relevant to the development of SBS such as the functionality of the residual bowel, especially the motility disorders [26].
 | Fig. 1Anatomy of short bowel causing intestinal failure in childhood. Classification of short bowel syndrome according to anatomy of the remnant intestine and different causes of intestinal resection.TIA: total intestinal aganglionosis, NEC: necrotizing enterocolitis.
|
In children the conditions most commonly leading to extensive SB resections are necrotizing enterocolitis (NEC), midgut volvulus, gastroschisis, intestinal atresia, and extensive aganglionosis, the last one leading to SBS without functioning colon (SBS type 1) (Table 1 and Fig. 1).
Table 1
Causes of intestinal failure

![]()
Total/Near Total intestinal aganglionosis (TIA/NTIA) is the most uncommon and life-threatening form of Hirschsprung disease (HD). Most of the time the neonate is left with less than 50 cm normally innervated small intestine or even shorter length below the ligament of Treitz. It may be considered as a SBS type 1 [27].
MANAGEMENT OF SBS-IF
Bowel adaptation after small intestinal resection is a physiological process resulting in bowel lengthening, both in length and diameter, and villous hyperplasia (Fig. 2) [28]. The management of SBS patients aims at promoting this physiological process by using as much as possible the gastrointestinal (GI) tract especially by oral feeding (OF) which is more physiological rather than enteral tube feeding (ETF) [28]. PN itself aims in promoting normal somatic growth during the time bridge for achieving full intestinal autonomy. PN should not be stopped until adequate intake and growth can be achieved with only OF and/or ETF.
 | Fig. 2Consequences of SIBO. Consequences of overfeeding a dilated and poorly motile intestine leading to intestinal stasis, SIBO, mucosal injury, bacterial translocation, portal inflammation, cholestasis and fibrosis.SIBO: small intestinal bacterial overgrowth, ETF: enteral tube feeding.
|
The optimal strategy for enteral feeding, OF vs. ETF and bolus vs. continuous, remains debated [28]. OF allows the maintenance of sucking and swallowing functions along with the psychological interest and enjoyment associated with eating, thus helping to prevent eating disorders (ED). It is important to point that OF promotes the release of epidermal growth factor (EGF) from salivary glands and increases GI secretion of trophic factors [29]. Sialoadenectomy in animals significantly attenuates ileal villus height, total protein and DNA content after SB resection that is reversed by the administration of both systemic and oral EGF [30]. Moreover, the stimulation of hormones released by the GI tract promotes adaptation whereas alternating fasting and feeding periods along with cyclical PN avoid permanent secretion of insulin and excessive fat synthesis and deposition (steatosis and fat body mass).
Enteral, preferentially OF, must be started as soon as possible after surgery. Breast feeding should be encouraged. Human milk (HM) contains a number of factors supporting the developing neonate's intestinal microbiota and immune system including HM oligosaccharides, live bacteria, nucleotides, immunoglobulin A, EGF and leucocytes [31323334]. Polymeric diets containing whole protein, lactose, and long chain triglycerides, are not usually used while extensively hydrolyzed formula (EHF) are preferred. The latter have the advantages of containing short peptides, better absorbed than free amino acids, as well as medium-chain triglycerides (MCT) [28]. Amino acid-based formulas (AABF) are generally used in the treatment of food allergies or in case of milk protein hydrolyzate intolerance [35]. True food allergies have been rarely documented in children with SBS [36]. Andorsky et al. [20] reported less intestinal allergy by using AABF, without clearly defining the criteria for the diagnosis of allergy. Two retrospective studies reported that the use of an AABF was associated with earlier weaning off PN and also a reduced rate of allergies [3738]. However, the very small sample sizes and the lack of control groups in these studies do not support the recommendation of using AABF in SBS patients. Moreover, commercially available AABF contain lower levels of MCT than EHF. In our practice EHF are widely used by OF [28].
Feeds should be increased gradually as tolerated. Tolerance is evaluated by measuring stool number and volume and by the observation of vomiting, irritability and abdominal as well as intestinal distension. Many factors can affect stool volume in SBS, including the length of the residual intestinal segment and the type of segment (the more proximal the resection the larger the fluid and sodium losses), the mucosal and endoluminal variables (residual enzymatic activity and absorptive capacity, bacterial overgrowth). Forced continuous ETF may worsen fluid, minerals and nutrients malabsorption and may result in severe perianal skin lesions. Bile salts malabsorption may be suspected in children without ICV and/or colon, presenting with high stool volume and perianal injury that can be improved by using cholestyramine. Fluid losses in these patients are often accompanied by sodium and zinc losses with subsequent risks of severe depletion; supplements should therefore be provided.
Finally, the use of a MCT rich diet (protein hydrolysate) by OF, as we experienced for the last decades, seems a good option
The colon in SBS-IF
1. The trophic role of the colon
When preserved, the colon, by hosting the largest part of intestinal microbiota plays a predominant role in the physiological adaptation of the intestine after large small intestinal resection. Colon is capable of reducing loss of energy and producing trophic factors [39]. In animal models, supplementation of an elemental diet with pectin, which is fermented to short chain fatty acids (SCFAs) in the colon, improved adaptation of the small intestine and colon in SBS [40]. The supplementation of PN with SCFAs or their intra-caecal infusion reduced mucosal atrophy and intestinal immune dysfunction following massive SB resection [41].
In addition to their local effects, systemic SCFAs, in animal studies, can affect the motility of both the stomach and the ileum through neuroendocrine mechanisms, probably through the expression of enteroglucagon family peptides and peptide YY [42]. Furthermore, both systemic and enteral SCFAs exert a trophic effect on the jejunum by increasing mucosal mass, DNA and villus height [43]. Since SCFAs are the preferred energy source for colonocytes, in patients with SBS the colon becomes an important organ for calories salvage. Unabsorbed carbohydrates are metabolized by the intestinal microbiota to SCFAs [39]. In turn, SCFAs may be considered as trophic factors directly by developing colon mucosa trophicity [44] or by promoting the release of glucagon-like peptide 2 (GLP-2) [42].
Restauration of intestinal continuity, such as anastomosis of the small intestine with the colon, should be done whenever possible as soon as possible. With improved colonic water and electrolyte absorption, PN can then be discontinued or at least decreased. In addition, anastomosis enables colonic fermentation of unabsorbed carbohydrates from the small intestine to occur, being an important source of energy assimilation. In spite of small intestine malabsorption in patients with SBS, both hyperphagia and adaptation of the remaining colon improve patient outcomes. A study evaluated morphology, proliferation status and transporters' expression level in the epithelium of the remaining colon of SBS adult patients compared to controls [45]. It seems that in hyperphagic SBS patients with severe malabsorption, adaptive colonic changes include an increased absorptive surface with an unchanged proliferative/apoptotic ratio and well-preserved absorption Na+/H+ exchangers (NHE) 2, NHE3, and PepT1 transporters messenger RNA levels [45]. As mentioned before, the preservation of the colon and its associated microbiota is essential for energy salvage, in reducing the need for PN and in improving the outcome of SBS patients. Bacteriological analysis based on culture-dependent methods has found that the microbiota of SBS patients is mainly composed of Lactobacilli, but neither qualitative nor quantitative information is available regarding the other main bacterial groups [46]. Few data have been reported in pediatric SBS but have mostly shown low intestinal dysbiosis and reduced microbiota diversity [4748].
2. Colonic hypermetabolism and D-lactic acidosis (D-LA)
Clinical manifestations such as abdominal distension, bloating and nausea—due to colonic microbiological hypermetabolism, may impair daily life and should be monitored. They are the consequences of the intestinal malabsorption leading to huge load of undigested carbohydrates reaching the colon. This condition may be worsened by hyperphagia or aggressive tube-feeding. One rare complication of colonic hypermetabolism, which is clearly different from SIBO, is D-LA.
D-LA, also referred to as D-lactate encephalopathy, is a rare neurologic syndrome that occurs in individuals with SBS or following jejuno-ileal bypass surgery [4950]. Fortunately, this complication is very rare. Symptoms typically present after the ingestion of high-carbohydrate feedings. Neurologic symptoms include altered mental status, slurred speech and ataxia, with patients often appearing drunk. Onset of neurologic symptoms is accompanied by metabolic acidosis and elevation of D-lactate plasma concentration. L-lactate concentration, which is reflected by serum lactate concentration is normal. Thiamine deficiency should be excluded [51]. D-lactate fecal concentration may be assessed routinely [44].
Lactobacilli and other bacteria, including Clostridium perfringens and Streptococcus bovis, when present ferment unabsorbed carbohydrate to D-lactic acid, which cannot be metabolized by D-lactate dehydrogenase. These organisms may proliferate in an acidic environment that may be promoted by the metabolism of unabsorbed carbohydrates to SCFAs. Diagnosis of D-LA is suspected from clinical symptoms and may be confirmed by assessing D-lactic acid in the stools [44]. The mechanism for the neurological symptoms is unknown. They have been attributed to D-lactate, but it is unclear if this is the cause or whether other factors are responsible [44]. Treatments described in case reports have included nothing or only limited reduction of enteral intake with avoidance of “refined” carbohydrates [52] (with spontaneous resolution), oral metronidazole, neomycin, vancomycin (for 10–14 days), . Probiotics, prebiotics and synbiotics have been used but without clear efficacy [5354].
Specific complications of the SBS-IF
1. SIBO
SIBO, characterized by the presence of excessive bacteria in the small intestine, is typically described as a malabsorptive syndrome occurring in the context of gut stasis syndromes. It is generally accepted that continuous tube feeding (CTF) offers the advantages of optimal digestion and absorption rate [31]. However, continuous infusion changes the intestinal motility pattern by missing fasting period [55]. Significant dysmotility—impairing intestinal bacterial clearance—leads to SIBO with subsequent gram-negative sepsis. SIBO and cholestasis are common especially in patients without ICV and those having abnormal motility (e.g., intestinal atresia, gastroschisis, and NEC). Aggressive continuous ETF is often attempted for mimicking “hyperphagia” with the aim of weaning the child off PN, that is thought to be the cause of liver injury. These patients present with dilated loops of bowel containing residual non-absorbed nutrients. This strategy results in increasing SIBO that can cause mucosal inflammation and increased permeability leading to sensitization and allergy as well as bacterial translocation, sepsis and cholestasis [9] (Fig. 2). In addition, aggressive ETF may also result in such an overloaded gut syndrome with abdominal discomfort, intestinal distension and loss of self-regulation of intake leading to ED.
Diagnosis of SIBO remains challenging. There is hope in the application of modern molecular techniques to the study of the small intestinal microbiome, together with some innovative sampling techniques, such as real-time intestinal gas sampling, may soon allow the clinician to truly define the spectrum of SIBO [56].
Treatment of SIBO is very controversial including large spectrum antibiotics and, prebiotics or probiotics [57585960]. Repeated administration of large spectrum antibiotics may improve SIBO but lead the risk of selection of highly resistant bacteria without treating the underlying cause of SIBO. Resuming aggressive ETF and performing non –transplant surgery in reducing small intestine diameter may restore intestinal motility and decrease SIBO (see below).
2. Causes and mechanisms of IFALD in SBS-IF
Many peoples continue to talk about PN-related liver disease suggesting that PN is the cause of liver disease [10]. CLD has been shown to be more frequent in the SBS patients than in any other IF conditions [61]. Out of 175 neonates with abdominal pathology requiring surgery, the patients with SBS (n=40) suffered significantly more morbidity than the group without SBS in all categories of investigation (surgical complications, septic events, and cytokine release syndrome (CRS), PN weaning delay, liver disease, and duration of hospitalization). The case fatality rate was 37.5% in patients with SBS versus 13.3% in patients without SBS (p=0.001). Most of the deaths were caused by liver failure or sepsis and occurred within 1 year from the date of surgery. More recently, the US IF consortium reported a large cohort involving 272 infants [62]. Overall, they have a gestational age of 34 weeks and birth weight of 2.1 kg (range, 1.2–2.7 kg) and were followed up for 25.7 months (range, 11.2–40.9 months). Residual SB length in 144 patients was 41 cm (range, 25.0–65.5 cm). Diagnoses were NEC (26%), gastroschisis (16%), atresia (10%), volvulus (9%), combinations of these diagnoses (17%), aganglionosis (4%), and other single or multiple diagnoses (18%). Prescribed medications included oral antibiotics (76%), H2 blockers (69%), and proton pump inhibitors (57%). Enteral feeding approaches varied among centers; 19% of the cohort received HM. The cohort experienced 8.9 new catheter-related blood stream infections (CRBSIs) per 1,000 catheter days. The cumulative incidences for enteral autonomy, death, and ITx were 47%, 27%, and 26%, respectively. Enteral autonomy continued into the fifth year after study entry. Interestingly, Finnish pediatric surgeons reported a significant correlation between small bowel diameter ratio and the grade of cholestasis in children with short bowel syndrome (r=0.534, p=0.001), providing evidence of a direct relationship between CLD and the underlying intestinal disease [63].
Nowadays IF and SIBO should be considered as the main causes of CLD. The most appropriate wording should be IFALD [91013]. It is probably the most important complication affecting children with SBS-IF on long-term PN. The prevalence of the disorder is unknown because there is no established definition of liver disease in this setting and it is unclear as to whether IFALD should be diagnosed on the basis of clinical, biological or histological criteria. Indeed, there are insufficient data on the degree and type of liver involvement in patients on long-term PN.
The main factors contributing to liver injury in these patients are recurrent CRBSIs, prematurity and low birth weight, lack of enteral feeding, disruption of entero-hepatic biliary acid cycle (proximal stoma and ileal resection), intestinal stasis and SIBO (obstruction, dysmotility, lack of ICV, over-tube feeding, etc). Table 2 reports the IF and PN related factors causing liver injury.
Table 2
Factors causing liver disease

![]()
It should be stressed that the most important factors leading to IFALD are those related to individual patient characteristics and, importantly, the episodes of CRBSIs or SIBO [6465]. Factors that link infection to cholestasis are either cytokines (mainly tumor necrosis factor alpha (TNFα), interleukin (IL)-1β, IL-6) or microbial toll-like receptor (TLR) 2 or TLR4 agonists [66]. Liver targets primarily include hepatocytes, but also extend to Küpfer cells, cholangiocytes, endothelial cells, and stellate cells. There are no direct studies of bile flow in humans given endotoxin, but there is sufficient indirect evidence to link endotoxin and endotoxin-induced cytokines, to cholestasis. During severe sepsis, including septic shock, hyperbilirubinemia is usually a central clinical finding, often out of proportion to typically mild elevations in serum transaminase. Interestingly, TNFα administered in humans has shown significant hyperbilirubinemia, further supporting a link between cytokines and cholestasis [67]. An important role in this process is played by liver inflammation caused by extra-hepatic infections in which microbial products brought to the liver through the blood stream, either directly or through production of cytokines, lead to alterations of bile flow. The inflammation associated with these changes may cause rapid fibrosis and eventually biliary cirrhosis with end-stage liver disease [6869707172].
IFALD develops frequently at very early ages, especially in premature infants in whom liver immaturity, frequent sepsis and NEC facilitate liver inflammation and severe damages. At this young age, PN is most often administered continuously over 24 hours and CRBSI is common. High risk situations for developing liver disease are summarized in Table 3. The combination of those factors makes the onset of CLD likely.
Table 3
High risk situations for developing liver disease
![]()
3. IFALD and intravenous lipid emulsions (ILE)
Frequently cited observational studies suggested a link between ILE and liver disease [7374]. Clayton compared the level of phytosterols in plasma of healthy subjects, patients with mild hepatic dysfunction and those with severe dysfunction who received soybean oil emulsion—rich in sterols, and found a link between liver damage and phytosterols plasma levels [75]. Phytosterols contained in soybean oil have been found to be associated with liver disease progression and their exclusion from ILE may also be beneficial in children on PN [76]. Regarding the presence of tocopherol in lipid emulsions, one should emphasize that there are different preparations of tocopherol: α-tocopherol is the form with far greater antioxidant activity [77]. Polyunsaturated fatty acids (PUFAs), such as the n-3 and n-6 fatty acids (FAs), are particularly susceptible to peroxidation and oxidative damage. Oxidation of PUFAs results in the formation of oxygen free radicals, which can bind to DNA and proteins and result in cell damage and death. α-Tocopherol can scavenge free radicals from peroxidized lipids to prevent propagation of oxidative lipid damage. While soybean oil emulsions contain a high amount of γ-tocopherol (which has 25% of the antioxidant power as compared to α-tocopherol), lipids based on fish oil are rich of the most powerful antioxidant vitamin E, α-tocopherol [77]. To ensure a proper antioxidant power in lipid preparations it is advisable to add 0.5 mg of α-tocopherol per gram of PUFAs. Improvement of cholestasis depends on maintaining an appropriate protein/energy ratio in PN and on achieving cyclic rather than continuous PN infusion [78].
IFALD is a multifactorial disease in which the use of soybean oil-based ILE in PN may represent the major culprit. Several factors should be taken into consideration when choosing an ILE for parenteral use: the content in essential FAs, the ratio of ω-6/ω-3, the PUFAs content, the amount of MCTs, the quantity of α-tocopherol and phytosterols.
The probable detrimental effect (pro-inflammatory) of ω-6 FAs on liver function is provided by studies that showed fat emulsions based on pure fish oil (containing ω-3 FAs) being successful as rescue therapy in pediatric patients with SBS affected by severe liver disease. The infusion of exclusively ω-3 FAs ultimately changed the management of these patients since it allowed the reduction of intake of pro-inflammatory ω-6 and phytosterols while increasing the amounts of α-tocopherol, a powerful antioxidant agent [137778].
The evidence gathered on the beneficial effects of fish-oil in these patients has led to its use in clinical practice. However, 2 different approaches have been developed in North America as compared to Europe. In North America, following the paper by Gura et al. [79] or Cowles et al. [80], a pure fish oil-based lipid emulsion (Omegaven®) has been promoted as the unique emulsion to be available on the US market. In Europe, as in many other countries, it has become early possible to use a composite lipid emulsion containing a mixture of soybean oil (30%), coconut oil (30%), olive oil (25%) and fish oil (15%) (SMOF-lipid®). Both ILEs contain 200 mg/L of α-tocopherol.
Some concerns have been raised on providing fish oil as the sole source of lipids over a long period of time. Pure fish oil provides less essential ω-6 FAs than that currently recommended in infants and young children [23]. Furthermore, Omegaven® (pure fish oil) can only be given at lower infusion rates compared to SMOF-lipid®). Omegaven® as unique source of ILE, may not be able to provide enough calories to sustain growth. Thus, the combination of several types of oil by mixing soybean oil (rich in ω-6 FAs), coconut oil (rich in MCTs), olive oil (rich in monounsaturated FAs) and fish oil (rich in ω-3 FAs) appears to promote better growth while limiting hepatic toxicity [81]. Randomized, double-blind, controlled trials in preterm babies stratified by body weight has analyzed a set of parameters (clinical data, laboratory data, FAs in plasma and red blood cells, plasma levels of α -tocopherol and-phospholipids) after infusion of PN with SMOF-lipid® or soybean oil-based emulsion [828384]. The SMOF-lipid® emulsion increased the content of eicosapentaenoic acid (EPA) and docosahexaenoic acids and reduced the ω-6/ω-3 ratio, improving also liver function tests).
In a study evaluating the long-term effects of the lipid mixture SMOF-lipid® vs. a soybean oil-based preparation in pediatric patients on home PN (HPN), no differences between biochemical and nutritional outcomes were recorded, but there was a clear association between the use of SMOF-lipid® and a significant decrease of bilirubin levels, that conversely increased in the soybean oil-based group [85].
Muhammed reported rapid and marked reductions in serum bilirubin in 17 children with cholestatic jaundice after switching from a soybean oil-based ILE to a multicomponent ILE containing a mixture of 30% soybean oil, 30% MCTs, 25% olive oil, and 15% fish oil (SMOF-lipid®). At 6 months, serum bilirubin declined by 99 μmol/L in children who were switched to SMOF and increased by 79 μmol/L in a historical cohort of children who received a soybean oil-based ILE (p=0.02) [86]
Finally, recent studies have emphasized the “superiority” of pure fish-oil derived lipid emulsions as a major advance for the management of patients on long-term PN. Randomized controlled trials have demonstrated the beneficial effect of SMOF-lipid® vs. soy-based lipid emulsion, no studies have compared SMOF-lipid® to Omegaven® in these patients. Preparations with pure fish oil have been shown to be effective in reversing cholestasis [798081]. However, their long-term use as the sole source of lipids is debated [8788]. Assessments of the plasma FAs profile in children on short term PN receiving 1 g/kg/day of pure fish oil-based LE, have shown a normal triene/tetraene ratio (Holman ratio) [8788]. Authors suggest that the definition of FA essentiality should be revised since pure fish oil LE contain amounts of both arachidonic acid and EPA sufficient to cover the needs [8788]. Those data need to be confirmed by assessing red blood cell FA profile in pediatric patients receiving long-term (>6 months) pure fish oil as the unique source of LE.
The last ESPGHAN/ESPEN guidelines make the following recommendations [89]: as part of measures to reverse IFALD in pediatric patients, a discontinuation of soy-based ILE, a reduction of other ILE dosage and/or the use of composite ILE with FO, should be considered along with the treatment and management of other risk factors (LoE 2þ, RG B, strong recommendation for)
R 4.19 The use of pure FO ILE is not recommended for general use in pediatric patients but may be used for short-term rescue treatment in patients with progression to severe IFALD, based on case reports. (LoE 3e4, GPP, conditional recommendation for, strong consensus).
4. Peri-anastomotic ulcerations (PAU)
PAU is a rare but severe complication after intestinal resection and anastomosis. It is described mostly in children [9091]. The main symptom is bleeding, leading to iron-deficiency anemia, which is life threatening. A survey reported a series of patients with PAU after intestinal resection in infancy, focusing on predictive factors, medical and surgical treatment options, and long-term outcomes [90]. Eleven patients (7 boys) with PAU after an intestinal resection and anastomosis in infancy were reported. The diagnosis of PAU was often delayed for several years. No predictive factor (including the primary disease, the length of the remnant bowel, and the loss of the ileocaecal valve) could be identified. Numerous treatment options, including antibiotics, probiotics (Saccharomyces boulardii) and anti-inflammatory drugs, proved to be ineffective to induce prolonged remission. Even after surgical resection, relapses were observed in 5/7 children. The mechanism leading to PAU remains unknown but it is likely that intestinal microbiota dysbiosis might play an important role. Another recent series reported 14 cases revealed by severe anemia, diarrhea, abdominal pain and growth failure in average 11.5 years after surgery [91]. Ulcerations were most often multiple (n=11), located on the upper part of ileocolonic anastomoses (n=12) and difficult to treat. No granulomas were seen but lymphoid follicules were frequent. In addition, either anti-Saccharomyces cerevisae antibody or anti-neutrophil cytoplasmatic antibody were positive in 4/9 tested patients and 8/11 genotyped patients exhibited a NOD2 mutation (p<0.001 when compared to French healthy controls). Contrary to previous reports with limited follow-up, no medical or surgical treatment could prevent recurrences. Because relapses may occur several years after discontinuation of PN, long-term follow-up is needed. Frequent relapses causing chronic iron-deficiency anemia might benefit in the future from fecal transplantation.
Non-transplant strategies for enhancing intestinal capacity
1. Autologous bowel reconstruction
Surgical approaches aimed at maximising GI digestive and absorptive function are crucial to the management of SBS. These include stoma closure and restoration of bowel continuity together with resection of strictures and closure of fistula. There are situations where surgical interventions aimed at reducing stasis in very dilated bowel, possibly decreasing SIBO (with its negative effects on digestion, absorption, and the liver) in the process and increasing contact time between luminal nutrients and mucosa might improve overall absorption. Indeed, these procedures aim not only to enhance the intestinal length and reduce the diameter of the distended intestinal loop with subsequent reduction of SIBO. The most common procedures are longitudinal intestinal lengthening and tapering (LILT) developed by Bianchi [92] in Manchester, UK and serial transverse enteroplasty (STEP) developed by Kim et al. [93] and mostly used in North America (Fig. 3A and B).
 | Fig. 3Autologous bowel surgery for short bowel syndrome. The LILT procedure and the STEP procedure.LILT: longitudinal tapering and lengthening, STEP: serial transverse enteroplasty.
|
The precise indications and the potential benefits of these procedures remain a matter of debate [9495]. Classical conditions and indications for bowel-lengthening surgery include the presence of a large intestinal diameter (>3–4 cm) for at least 20 cm of SB and a minimum total bowel length of 40 cm.
LILT involves longitudinal splitting of the SB remnant along its mesenteric and anti-mesenteric border, ending up with 2 tubes of bowel of identical length each with their own blood supply which are then joined together [92]. The advantages of the LILT procedure (Fig. 3A) include the conservation of the normal orientation of the muscular fibers allowing more physiological peristaltic contraction, and the possibility to further perform a STEP procedure on the operated segments. The disadvantages are the risk of vascular complications during surgery making LILT more technically demanding as compared to the STEP procedure [92939495]. Moreover, results after STEP and re-STEP procedure are not as performant as expected [96979899].
The STEP procedure involves the use of a surgical stapler applied sequentially from alternating and opposite directions to the dilated loop, in a transverse, partially overlapping fashion creating a zigzag—like channel of approximately 2 to 2.5 cm in diameter (Fig. 3B). This operation has the great advantage of being simple and reproducible [93]; unlike LILT, no anastomosis is needed, and the mesenteric blood supply is not put at risk. If the bowel re-dilates, a further STEP procedure can be undertaken. Unfortunately, there are no surgical techniques that can reliably increase SB surface area, and by so doing rapidly achieve more than the background process of gut adaptation.
Plasma citrulline is a marker of SB enterocyte mass [567]. A 5-year follow-up cohort study after STEP confirms the efficiency of this procedure. Interestingly, both D-xylose - a marker of carbohydrate absorption and mucosal integrity - and plasma citrulline - a marker of SB enterocyte mass - increased significantly postoperatively [100]. This suggests that STEP procedure by reducing SIBO, restores small intestinal mucosa integrity and improves villous size within the first weeks following the procedure. However recent data showed no adaptive mucosal hyperplasia or muscular alterations occurred between first and repeat STEP [101]. This suggest that persistent inflammation and lacking mucosal growth may contribute to continuing bowel dysfunction in SBS children, who require repeat STEP procedure, especially after removal of the ileocecal valve. The overloaded gut syndrome may be defined as the association of dilated intestinal loops, abdominal discomfort, SIBO, cholestasis and failure to thrive in a SBS patient who is partially or totally enterally fed. Surgical bowel-tapering with or without lengthening should be considered in such setting whatever the patient is PN-dependent or not.
The management of TIA/NTIA is challenging. Extended myectomy-myotomy has been proposed as a therapeutic alternative for TIA/NTIA. We have a successful experience in around 15 patients nowadays. However, it does not allow to achieve intestinal autonomy [102], and the role of autologous intestinal reconstructive surgery (AIRS) is controversial [103]. A recent cross-sectional study concludes that AIRS may be performed in carefully selected patients [103]. It may be an effective way to enhance residual bowel absorptive function and to reduce PN requirements. AIRS and ITx are complementary surgical tools in the complex management of TIA/NTIA.
2. Hormonal therapy and other adaptive treatments
Hormonal therapy is promising in the management of infants with SBS. The role of recombinant human growth hormone (rhGH) alone or in combination with glutamine has been investigated. Inconsistent results have been reported in adults receiving rhGH, with reported side effects [104]. A few studies of rhGH alone or in combination with glutamine have been carried out in PN dependent children with SBS [105106107]. Despite some decrease in PN requirements during treatment these trials showed little benefit on body composition and mucosal absorption in the long-term [105106107].
GLP-2 is produced by the L-cells of the terminal ileum in response to luminal nutrients and has a trophic effect on the intestine, promoting absorption and adaptation [108]. GLP-2 has been shown to increase the surface area of the gut mucosa, up-regulate nutrient absorption, improve gut-barrier function, increase intestinal blood flow and decrease bone resorption [108]. Patients with low levels of GLP-2 following the resection of the terminal ileum and/or the ICV improved intestinal absorption and nutritional status after treatment with GLP-2 [109]. A 12-week, open-label study, enrolled SBS PN dependent patients aged 1–17 years [110]. It has been concluded that teduglutide (GLP-2 analogue) was well tolerated at 0.025 or 0.05 mg/kg/day and was associated with trends toward reductions in PN requirements and advancements in enteral feeding. However, study limitations included its short-term, open-label design, small sample size and heterogeneity of both patients and management because of the multicenter study. Monocenter trials are required for addressing recommendations and extend the use of GLP-2 analog (e.g., Teduglutide Revestive®) at a dose of 0.05 mg/kg/day. Results of a more recent 24-week open-label multicenter study should be available. We are currently performing a monocenter open-label study including 25 SBS children aged >3 years receiving a daily dose 0.05 mg/kg for one year. According to the price of the treatment, more data are needed for establishing a consensus for “selecting” the best candidates for whom, permanent intestinal autonomy may be achieved while continuing GLP-2 analog administration.
Oral insulin has been shown to be beneficial in animal models and might be assessed very soon in infants and children [111]. Other relevant treatments associated with a trophic effect on the bowel mucosa such as SCFA may be beneficial in children with SBS [112]. Finally, there is also interest in the use of other trophic factors such as EGF and insulin-like growth factor-1 in children with IF and SBS [113].
Outcome of SBS and long-term growth
Mortality decreased during the last decade especially following the implementation of the so called “intestinal rehabilitation centers” (IRC) [114115116117118119]. Multidisciplinary management, improved prevention of SIBO and sepsis by performing autologous bowel reconstruction [9293949596979899100], by preventing CRBSIs with taurolidine or ethanol lock procedures [120121], by using the last generation of lipid emulsions [13]. As a matter of fact, the rate of ITx decreased in the mean-time [122].
Children with SBS-IF often develop oral aversions (OA) and ED. A long time ago, it was pointed by Moreno Villares et al. [123] that enteral feedings delivered by either gastrostomy or a nasogastric tube, often used in infants to provide adequate caloric and nutrient intake, may induce ED. It is important to consider the critical period involved with OF during the first months, or even the first days of life. According to the complexity of feeding children with SBS, if we are not aware of a rapid introduction of OFs they may develop poor feeding skills. Children in transition for tube to OF may display oral-motor, sensory and developmental feeding problems. There is limited research and information on which to base interventions that will preserve and develop oral motor and feeding skills. A recent review pointed physical, developmental, and social aspects of eating and mealtimes. Interdisciplinary teams are needed to effectively address these complex OF problems [124125126]. Accurate identification the underlying issues will allow healthcare providers to develop interventions to improve feeding outcomes for children with SBS. Future research should focus on evaluating the effectiveness of interventions that address each of the underlying issues. In clinical practice, the role of nurses for supporting the development and the psycho-motor coordination in diseased neonates, should be emphasized in order to prevent ED. Later in life, it is very challenging to develop healthy eating behavior in children with long lasting ED and OA who remain dependent on tube feeding. It may require very challenging tube weaning methods. A recent paper reported messy play therapy (MPT) using sensory activities to provide another meaningful avenue for learning in children by creating a fun way to experience new textures [127]. Better quality of life (QoL) and mealtimes with family were reported at median follow-up of 39 (24–56) months. Further studies are needed to evaluate the effectiveness of MPT and other approachs in a larger scale of patients.
Some studies have been reported, involving the long-term growth and nutrition status of children with neonatal SBS after weaning off PN [22128129130]. Improved care of patients with SBS significantly achieved more optimal weight gain for age compared with decade 1980 [128]. However, the final genetic target size is not always achieved while some deficiencies may be evidenced [129130]. Indeed, children with SBS are still at risk for different nutrient malabsorption even after weaning off PN for a long time. They may develop such an “overloaded gut syndrome” with failure to thrive requiring, for some, PN to be restarted. Therefore, they need long-term, regular monitoring and intensive nutritional care to prevent various nutrient deficiencies. On the other hand, long-term follow-up is mandatory, not only for growth monitoring but for assessment of micro-nutrients deficiency (e.g., zinc status in case of high stool output, liposoluble vitamins and vitamin B12 in case of ileal resection) and search for biliary lithiasis if the gallbladder was not removed.
In patients with TIA/NTIA, appropriate management strategies are not well established for this type 1 SBS. Surgery is performed as a simple jejunostomy below the ligament of Treitz with or without or short-segment longitudinal myomectomy [102103131]. Nutritional management includes cyclic PN (home-PN) associated with OF for reducing the risk of liver disease and promoting oral skills [8124125126]. Continuous attention is needed in the daily long-term management of these unstable infants and children with a permanent risk of dehydration and subsequent complications such as hypercalcemia, renal failure. Growth may be achieved as in other forms of SBS if PN is adapted especially according to the high water-electrolytes losses.
Long-term management of SBS-IF
1. HPN
Long-term PN administration is best achieved at home. HPN, first used in the early 1980s, allows for full nutritional support of children and adults with temporary or permanent IF at home [8132133134135136137138139]. Survival of children receiving prolonged PN depends mainly on the underlying diagnosis and has increased dramatically during the last three decades; Nevertheless, complications such as CRBSIs, IFALD and loss of venous access can seriously challenge the clinical stability of patients with IF [9140].
The expertise required to prescribe PN both at home and in the hospital usually comes from a dedicated hospital-based nutritional team who has a thorough knowledge of energy expenditure, nutrients and trace-elements requirements by age, appropriate central catheter handling, and awareness of the risk and complications of long-term PN. HPN must be tailored to the single patient and its family, always maintaining the goal of counteracting the deleterious aspects of IF. Official guidelines and position statements on central catheter handling and PN prescription have been published [141].
One of the largest cohort ever reported from a single center involves 251 children referred to the Paris-Necker IRC and discharged on HPN between January 1st, 2000 and December 31st, 2013 [8]. In this survey, 217 children (86%) had a primary digestive diseases (PDD). The mean age at HPN onset was 0.7±0.3 year with a mean duration of 1.9±0.4 years. The major indication for HPN was SBS (59%) secondary to midgut volvulus (16.7%), NEC (12.3%), gastroschisis (12%), extensive HD (10%) and intestinal atresia (6.4%). Other PDD were congenital enteropathies (10%), CIPOS (9.1%), and inflammatory bowel diseases (5.1%). At the end of the study period, 56% of children were weaned off HPN, 8% had ITx and 9.6% of children died - most of them had immune deficiency. The major complications of HPN were CRBSI (1.7 per 1,000 days of catheter) and IFALD, 51 children, (20% of the cohort). Children with congenital enteropathies had the highest rates of IFALD (44% of the sub-group). Children on HPN in this cohort have a shorter HPN duration to weaning, lower death rate and longer interval to catheter replacement than other studies. One of the most important advances for long-term PN dependent patients has been the onset of antiseptic catheter locking [120121].
The European data on the long-term management of IF on HPN need to be compared with other continent, especially North America. Several papers from the US, report “IRC” including early management of IF, especially SBS in both neonatalogy and surgical wards, with the aim of the earliest PN weaning [142143144145]. Some patients get severe complications and become candidates for ITx. Some others fail to be weaned off PN and are discharged on home-PN when suitable. The organization and follow-up of HPN is supposed to be shared between pediatric gastroenterology-nutrition teams and home care-giver companies according to the local facilities. Unfortunately, there is almost no report in the literature about the prevalence and results of pediatric HPN programs making a comparison with North-America management almost impossible. One of the reasons is linked to the organization and the management of IF. In France, patients suffering from IF, especially those with SBS, are managed by specialized medico-surgical departments, including pediatric surgeons and pediatric gastroenterologists-nutritionists or neonatalogy units. The decision of discharging the child on HPN and the follow-up are fully dependent on pediatric gastroenterology and nutrition teams. The French network is organized regionally. Patients are referred to the closest of the 7 reference centers for HPN.
2. IRC and multidisciplinary team
Paediatric IF is a multifaceted condition requiring the competent contributions of several medical and allied health professionals both for inpatient and outpatient care. Therefore, the formation of a multidisciplinary team is vital to achieve optimal results [114115116117118119142143144145].
The IF team should ideally include staff specialised in surgery, gastroenterology and nutrition, a paediatric dietician and nurses experienced in central venous catheters handling and PN infusion. Special consideration should be given to the link between the hospital and the home care teams. Fostering coordination of surgical, medical, and nutritional management is vital to provide high quality, integrated care of patients with IF, thus improving remarkably the survival of these patients. The 3 most important issues in the management of children with IF include: 1) a good and early link between primary care givers and IF programs; 2) the presence in the program of both intestinal rehabilitation and ITx expertise; and 3) The participation in the network of the organisations providing HPN solutions. Collaborative strategies must be developed in order to reduce mortality and morbidity in patients with IF, especially for those who are referred for permanent IF or ITx.
ITx for SBS-IF
Although a large percentage of children with SBS-IF can survive with long-term PN, a proportion of patients eventually develop life-threatening complications such as severe septic episodes, fluid and electrolytes imbalance, loss of venous access for PN and end stage liver disease [9140]. In these patients nutrition has failed both in the enteral and the parenteral routes. These patients are considered to have “nutritional failure” and should be referred for ITx as early as possible [9140].
Unfortunately, relatively few advances have been achieved in the field of ITx and multivisceral transplantation in the last 10 years with no significant improvement in the long-term patient and graft survival [146]. According to the intestinal transplant registry, approximately 2,500 ITx have been carried out so far in 79 worldwide transplant centers, of whom half are alive. Among 1351 transplanted children the 5- and 10-year graft survival rate is reported as approximately 50% and 30% respectively; the 5- and 10-year patient survival rate is similar, approximately 50% and 30% respectively. In patients with a functioning graft approximately 60% have a normal function whereas 40% require partial PN or intravenous fluids [146] while QoL may improve [147]. These sobering figures mandate the adoption of all relevant strategies to avoid ITx until new protocols are available to achieve a better outcome.
There is probably a different threshold for ITx on both sides of the Atlantic Ocean. The European approach is more inclined to support long-term HPN, which is cost-effective and provides a better QoL, rather than to refer a child for ITx. Support for this view comes from Pironi et al. [148] who have performed a 3-year prospective study including both adults and children on long-term PN for IF. They compared ‘non-candidates’ for ITx (no indications nor contraindications), with ‘candidates’ who had an indication according to the USA Medicare and Medicaid Services definitions, and a high risk of death or morbidity according to the American Society of Transplantation position paper [149150]. The results showed that only patients with nutritional failure due to IFALD or major catheter complications had an increased risk of death on HPN, thus supporting its use as the primary treatment for IF [150]. Therefore, it was suggested that ITx should be used only as a life-saving procedure [9151]. Although experienced transplantation centers have suggested that the role of ITx should be expanded to a pre-emptive/rehabilitative procedure applicable to all patients with irreversible IF, the recent findings have shown that HPN is the treatment of choice for IF in adults as well as in children. An early referral is essential to prevent or optimize the long-term management of IFALD. Central venous-catheter-related major complications might be indications for a pre-emptive ITx in selected patients. As a matter of fact, “nutritional failure” should be regarded mostly or even only as a clear indication to ITx [9].
Isolated liver transplantation (LTx) has been performed for IFALD in SBS-IF patients. Taha et al. [152] reported a group of children with SBS and IFALD who have the potential for adaptation in the residual bowel underwent isolated LTx. The prognosis remains poor after this procedure, 8 survivors out of 14 [152]. This procedure should be avoided by preventing IFALD. If performed, it should be exercised with extreme caution. These children need careful assessment before isolated LTx and close follow-up with an experienced multidisciplinary team to monitor nutritional outcomes and may need consideration for transplant or non-transplant surgery in the long-term.
In patients with TIA, ITx is undertaken according to the occurrence of complications (water-electrolytes disorders, CRC, and IFALD) and/or the wish of parents for another QoL. In 12 patients with TIA, it was reported an outcome rate of 62.5% in the LITx group and 75% in the ITx group, both with half colon grafting [153]. All the surviving patients were weaned off PN, after a median of 57 days. Pull through of the colon allograft was carried out in all patients. Fecal continence is normal in all but one of the surviving children. When long-term graft tolerance is achieved, growth is normal and QoL improved [154].
CONCLUSION
IF requires specialized and individualized medical therapy that includes surgery, medical equipment, nutritional products, and standard nursing care. Intestinal rehabilitation programs provide such complex care with the goal of achieving enteral autonomy and OF with or without ITx. The treatment of permanent IF has made remarkable strides in the past decades. The establishment of multi-disciplinary intestinal rehabilitation programs at leading centers has improved the survival of children with IF while the morbidity associated with both IF and PN has significantly decreased. These programs almost all include neonatalogists, pediatric surgeons, pediatric gastroenterologists, specialized nurses, and dietitians; many also include a variety of other medical and allied medical specialists, providing integrated interdisciplinary care.
Recent advances in the knowledge of factors implicated with PN and IF complications and improvements in the medical and surgical management of SBS result in better outcomes for these patients. Isolated LTx for SBS-IF patients who have the potential of bowel adaptation should be no longer required. It is interesting to note that the most recent International ITx registry report at the XV SB Transplant Symposium, New York, June 2017 showed early evidence of a world-wide trend of reduction in the number of pediatric ITx. This might be explained by at least the following factors:
• Development of IRC with increasing IF expertise [114115116117118119142143144145]
• Enlarged use of non-transplant surgery [9293949596979899100101102103]
• Better prevention of IFALD, with fish oil-based lipid emulsions playing a role [156]
• Improved prevention of CRBSIs by using taurolidine or ethanol locks [120121]
• Onset of hormonal treatment in SBS-IF by using GLP-2 analogs [108110]
The combined and coordinated talents and skills of multiple types of health care practitioners have the potential to ameliorate the impact of IF and improve health outcomes and QoL.
Major efforts are needed to improve the outcome of ITx that will likely remain part of the armamentarium required to prolong the survival of children with life-threatening complications of IF. Nevertheless, the European experience has led to support a more conservative approach more inclined to HPN, limiting referrals for ITx only to children with nutritional failure [9140151157].
 XML Download
XML Download