

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Fungal infections are emerging as a major cause of healthcare-associated infection, and invasive fungal infections (IFI) are associated with high mortality in burn patients. The (1,3)-β-D-glucan (BG) assay has been increasingly used for the diagnosis of IFI, but its effectiveness remains uncertain. As such, we evaluated the BG test in patients with severe burn injuries.
Methods
From July to December 2018, a total of 86 patients with major burn injuries were prospectively tested using a Fungitell assay (Cape Code, East Falmouth, MA). BG levels were measured within the first week of intensive care unit admission and compared with clinical symptoms of patients and results of a fungal culture.
Results
A total of 11 patients were identified as proven or possible IFI. Thirty seven patients (43.0%) were positive, 5 (5.8%) were intermediate, and 44 (51.2%) were negative based on a 60–80 pg/mL cutoff. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were 81.8%, 56.0%, 24.3%, and 95.5%, respectively. A receiver operating characteristic (ROC) analysis showed an area under the curve of 0.725, an optimal cut-off of 124.2 pg/mL, a sensitivity of 81.8%, and a specificity of 74.7%.
Figures and Tables

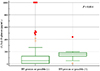 | Fig. 2Comparison of (1,3)-β-D-glucan levels in patients with and without proven or possible invasive fungal infections (IFI). Patients with proven or possible invasive fungal infection (IFI) (N=11) showed statistically significantly higher (1,3)-β-D-glucan levels (157.2 pg/mL, 95% CI: 124.7–185.2 pg/mL) compared to patients without proven or possible IFI (51.3 pg/mL, 95% CI: 10.0–125.0 pg/mL, N=75).
|
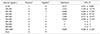
 | Fig. 3Sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) of (1,3)-β-D-glucan for (A) invasive fungal infection (IFI) proven (B) IFI proven or possible.
|
 | Fig. 4Receiver operator characteristic (ROC) curve of (1,3)-β-D-glucan cutoff values to define invasive fungal infection (IFI).
|

Acknowledgements
This study was supported by Korean Society for Healthcare-associated Infection Control and Prevention.
References
1. Garcia-Vidal C, Upton A, Kirby KA, Marr KA. Epidemiology of invasive mold infections in allogeneic stem cell transplant recipients: biological risk factors for infection according to time after transplantation. Clin Infect Dis. 2008; 47:1041–1050.

2. Alexander BD, Smith PB, Davis RD, Perfect JR, Reller LB. The (1,3){beta}-D-glucan test as an aid to early diagnosis of invasive fungal infections following lung transplantation. J Clin Microbiol. 2010; 48:4083–4088.
3. Racil Z, Kocmanova I, Lengerova M, Weinbergerova B, Buresova L, Toskova M, et al. Difficulties in using 1,3-{beta}-D-glucan as the screening test for the early diagnosis of invasive fungal infections in patients with haematological malignancies--high frequency of falsepositive results and their analysis. J Med Microbiol. 2010; 59(Pt 9):1016–1022.
4. Garey KW, Rege M, Pai MP, Mingo DE, Suda KJ, Turpin RS, et al. Time to initiation of fluconazole therapy impacts mortality in patients with candidemia: a multi-institutional study. Clin Infect Dis. 2006; 43:25–31.
5. Voss A, le Noble JL, Verduyn Lunel FM, Foudraine NA, Meis JF. Candidemia in intensive care unit patients: risk factors for mortality. Infection. 1997; 25:8–11.
6. Pappas PG, Alexander BD, Andes DR, Hadley S, Kauffman CA, Freifeld A, et al. Invasive fungal infections among organ transplant recipients: results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Clin Infect Dis. 2010; 50:1101–1111.
7. Singh N, Avery RK, Munoz P, Pruett TL, Alexander B, Jacobs R, et al. Trends in risk profiles for and mortality associated with invasive aspergillosis among liver transplant recipients. Clin Infect Dis. 2003; 36:46–52.
8. Albert O, Toubas D, Strady C, Cousson J, Delmas C, Vernet V, et al. Reactivity of (1→3)-β-d-glucan assay in bacterial bloodstream infections. Eur J Clin Microbiol Infect Dis. 2011; 30:1453–1460.
9. Bellanger AP, Grenouillet F, Henon T, Skana F, Legrand F, Deconinck E, et al. Retrospective assessment of β-D-(1,3)-glucan for presumptive diagnosis of fungal infections. APMIS. 2011; 119:280–286.
10. De Vlieger G, Lagrou K, Maertens J, Verbeken E, Meersseman W, Van Wijngaerden E. Beta-D-glucan detection as a diagnostic test for invasive aspergillosis in immunocompromised critically ill patients with symptoms of respiratory infection: an autopsy-based study. J Clin Microbiol. 2011; 49:3783–3787.
11. Karageorgopoulos DE, Vouloumanou EK, Ntziora F, Michalopoulos A, Rafailidis PI, Falagas ME. β-D-glucan assay for the diagnosis of invasive fungal infections: a meta-analysis. Clin Infect Dis. 2011; 52:750–770.
12. Theel ES, Doern CD. β-D-glucan testing is important for diagnosis of invasive fungal infections. J Clin Microbiol. 2013; 51:3478–3483.
13. Fesel PH, Zuccaro A. β-glucan: crucial component of the fungal cell wall and elusive MAMP in plants. Fungal Genet Biol. 2016; 90:53–60.
14. Onishi A, Sugiyama D, Kogata Y, Saegusa J, Sugimoto T, Kawano S, et al. Diagnostic accuracy of serum 1,3-β-D-glucan for pneumocystis jiroveci pneumonia, invasive candidiasis, and invasive aspergillosis: systematic review and meta-analysis. J Clin Microbiol. 2012; 50:7–15.
15. De Pauw B, Walsh TJ, Donnelly JP, Stevens DA, Edwards JE, Calandra T, et al. European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group. National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis. 2008; 46:1813–1821.
16. Cuenca-Estrella M, Verweij PE, Arendrup MC, Arikan-Akdagli S, Bille J, Donnelly JP, et al. ESCMID Fungal Infection Study Group. ESCMID* guideline for the diagnosis and management of Candida diseases 2012: diagnostic procedures. Clin Microbiol Infect. 2012; 18:Suppl 7. 9–18.
17. He S, Hang JP, Zhang L, Wang F, Zhang DC, Gong FH. A systematic review and meta-analysis of diagnostic accuracy of serum 1,3-β-D-glucan for invasive fungal infection: focus on cutoff levels. J Microbiol Immunol Infect. 2015; 48:351–361.
18. Santucci SG, Gobara S, Santos CR, Fontana C, Levin AS. Infections in a burn intensive care unit: experience of seven years. J Hosp Infect. 2003; 53:6–13.
19. Blyth DM, Chung KK, Cancio LC, King BT, Murray CK. Clinical utility of fungal screening assays in adults with severe burns. Burns. 2013; 39:413–419.
20. Rafik A, Diouri M, Bahechar N, Chlihi A. Epidemiology of nosocomial fungal infections in the National Center for Burns in Casablanca, Morocco. Ann Burns Fire Disasters. 2016; 29:90–93.
21. Greiner M, Pfeiffer D, Smith RD. Principles and practical application of the receiver-operating characteristic analysis for diagnostic tests. Prev Vet Med. 2000; 45:23–41.
22. Fraser VJ, Jones M, Dunkel J, Storfer S, Medoff G, Dunagan WC. Candidemia in a tertiary care hospital: epidemiology, risk factors, and predictors of mortality. Clin Infect Dis. 1992; 15:414–421.
23. Ekenna O, Sherertz RJ, Bingham H. Natural history of bloodstream infections in a burn patient population: the importance of candidemia. Am J Infect Control. 1993; 21:189–195.
 XML Download
XML Download