

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Alcohol is an often misused substance throughout the world. Severe alcohol abuse creates many social and economic problems. Alcoholic ketoacidosis (AKA) is an acute complication in alcoholics who are chronically malnourished. Normal or slightly elevated serum glucose, binge drinking (ending in nausea, vomiting, and decreased intake), elevated anion-gap metabolic acidosis (without alternate explanation), and positive serum ketones (absence of ketones cannot exclude the diagnosis) are known as diagnostic criteria for AKA1).
AKA itself is known to have a good prognosis however, some AKA especially accompanying infection, can produce severe and irreversible cellular dysfunction which can be associated with a very high mortality2). Some institutions in Korea have reported that the mortality of AKA is 22-23%3), which is more than 20 times higher than that of the USA (1%)4). Severe acidosis and combined conditions are reported as poor prognostic factors for AKA2). Although increased C-reactive protein (CRP) levels were reported in postmortem AKA patients5) and chronic alcohol abuse is known to reduce immunity6), there has been no report that this inflammatory marker is a poor prognostic factor for AKA.
In systemic inflammatory status, immature granulocytes (IG), which are one of the inclusion criteria of systemic inflammatory response syndrome (SIRS), are increased78). The delta neutrophil index (DNI) is assessed by an automated blood cell analyzer and is strongly correlated with manual IG counts8). DNI is the immature granulocyte fraction provided by a blood cell analyser; it is determined by subtracting the fraction of mature polymorphonuclear leukocytes from the sum of myeloperoxidase-reactive cells and reflects the number of immature neutrophils as a blood biomarker. In the meta-analysis, DNI was reported as a prognostic marker for mortality in adults with sepsis9). In addition, DNI is regarded as an early marker of sepsis because it predicts septic shock and sepsis better than CRP, which is well known as an inflammatory indicator710). Chronic alcohol consumption and acidosis aggravates inflammatory reaction and frequently combining infection. Therefore, we evaluated potential prognostic factors for AKA patients, including inflammation indices such as DNI, CRP, and white blood cell (WBC) counts, and hypothesized that DNI might be one of the early prognostic markers of mortality in patients with AKA.
Methods
1. Study setting and population
This retrospective and the observational study included 131 male patients, who were diagnosed with AKA at the emergency department of Wonju Severance Christian hospital from September 2009 to May 2014. All patients with the word “alcoholic ketoacidosis”, or “ketoacidosis” in the discharge codes registered in the computerized hospital records were selected. We then confirmed the diagnosed of AKA by several findings, including the history of chronic alcohol abuse and a recent episode of binge drinking with metabolic acidosis on arterial blood gas analysis and increased serum anion gap in serum chemistry1). A total of 13 patients were excluded from analyses due to other diagnoses or the inability to obtain patient history (AKA combined with organophosphate intoxication (n=3), diabetic ketoacidosis (n=1), obstructive nephropathy (n=1), and unable to obtain history due to lack of guardian or unconscious patient (n=8)). Unfortunately, there were only 2 female patients during evaluation periods. One hundred eighteen male patients were finally included in the evaluation. Underlying disease, demographic characteristics, and laboratory results were investigated on the day of hospital arrival. We categorized survival and non-survival groups according to the patient's survival. We defined renal survival patients as those who did not receive renal replacement therapy during hospitalization. Patient informed consent was not required for this retrospective, observational study, and the patient records were anonymized prior to the analysis. This study was approved by the institutional review board of Wonju College of Medicine, Yonsei University (CR318085).
2. Data collection
Data were collected by retrospectively reviewing medical records. Demographic data and clinical variables including, age, sex, hospitalization duration, initial clinical parameters (blood pressure, heart rate, respiratory rate, and 24 hour urine output), presence of gastrointestinal (GI) symptoms (including nausea, vomiting, melena, hematochezia, diarrhea, and abdominal pain), central nervous system(CNS) symptoms (including mental change, dizziness, seizure, and dysarthria), dyspnea, general weakness, past disease history, alcohol intake history (duration, amount, last drinking time, and amount), use of inotropes (norepinephrine, vasopressin, and epinephrine) during hospitalization, need for mechanical ventilation or renal replacement therapy during hospitalization, total sodium bicarbonate (NaHCO3) infused (mEq) during the first 24 hours after admission, complications during hospitalization, and mortality were recorded. Initial Acute physiology and chronic health evaluation (APACHE) II scores were calculated to measure the severity of patients' conditions11).
Blood samples for the analyses of DNI and other laboratory parameters were obtained from arterial or venous puncture within the first 2 hours of hospital admission. The blood samples were immediately transferred to the laboratory department, and the DNI assays were performed within 2 hours of blood sampling. DNI was measured through an automated specific hematology cell analyzer (ADVIA 2120, Hematology System, Siemens Healthcare Diagnostics, Forchheim, Germany). The DNI was calculated in leukocyte differentials using the following formula: DNI=(the neutrophil subfraction and the eosinophil subfraction measured in the myeloperoxidase (MPO) channel by cytochemical MPO reaction)−(the PMN subfraction measured in the nuclear lobularity channel by the reflected light beam)81213).
3. Statistical analysis
Data are expressed according to the properties of the variable. Continuous variables are presented as mean and standard deviation (SD). Categorical variables are presented as frequency and percentage. In order to compare groups, we performed the two-sample t-test, ANOVA, and Chi-square test (Fisher's exact test) as appropriate. Prognostic variables for mortality and renal survival were analyzed by using the univariate Cox proportional hazard model. Considering the Cox proportional hazards model in univariate analysis and collinearity, multivariate Cox regression analysis was performed. The univariate and multivariate Cox regression analysis results are presented as hazard ratios (HR) and 95% confidence intervals (CI). Considering univariate Cox regression results, collinearity, and clinical importance age, history of diabetes, and history of liver cirrhosis were used in multivariate Cox regression of in hospital day renal replacement therapy (Renal Survival) and hospital day mortality (Patient Survival). The discrimination of DNI, pH, and GFR for all-cause mortality and renal survival were evaluated using the area under the receiver operating characteristics (ROC) curve. Decreased pH and GFR values are associated with poor prognosis in AKA patients. Therefore, we used reverse pH(-pH), GFR(-GFR) in ROC curves. The optimal cut off point for ROC curves was selected for maximizing the sensitivity and specificity of the selected values. Kaplan-Meier survival and renal survival curves were then drawn and Log-rank values were calculated to assess their statistical significance. A p-value less than 0.05 was considered statistically significant. All statistical analyses were conducted using the IBM Statistical Package for the Social Science (SPSS) version 23.0 (IBM Corporation, Armonk, NY, USA).
Results
1. Patients characteristics and laboratory findings
The average duration of hospitalization for the total 118 male patients was 10.9 days (range 0–71 days) (Table 1). All-cause mortality was 32.2% (38 patients). The most common cause of death was alcoholic ketoacidosis itself (52.6%) (Table 2). On average, mortality occurred 6.7 days after hospitalization. During the hospital day, 64 (54.2%) patients had infectious complications. The most common pathogen of infection was Methicillin-Resistant Staphylococcus aureus (23.4%) (Table 3). The most common symptoms among patients were GI symptoms (48.3%), such as nausea, vomiting, diarrhea, melena, hematochezia, hematemesis, and abdominal pain. History of diabetes, hypertension, liver cirrhosis and the amount of alcohol ingested were not different between survival and non-survival patients. Clinical characteristics that differed between the survival group and the non-survival group are shown in Table 1. On laboratory results, CRP, creatine kinase (CK), and bicarbonate (HCO3) were not statistically different between survival and non-survival patients. Laboratory results that differed between survival and non-survival patients are shown in Table 1. The DNI level in the survival group (4.8±6.4) was statistically lower than in the non-survival group (11.4±12.5) (p<0.001).
2. Analysis of risk factors affecting renal survival
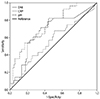
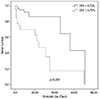
In Cox regression analysis, initial laboratory values (DNI, MAP, pH, hemoglobin, platelet counts, albumin, PT (INR), lactate, and Cr), use of ventilator during hospitalization, use of inotropic during hospitalization, cardiac arrest, and APACHE II score on first hospital day were significantly associated with renal survival. In multivari ate adjustment analysis, initial DNI level and initial pH remained as independent predictors of in-hospital renal replacement therapy (Renal Survival) (Table 4). ROC curves were drawn for initial DNI (AUC 0.671, 95% CI 0.553–0.789), initial pH(AUC 0.738, 95% CI 0.637–840) and CRP (AUC 0.557, 95% CI 0.431–0.683) to determine cut-off values predicting renal survival (Fig. 1). Patients with an initial pH value above 7.044 had higher renal survival days (47.0 days) than other patients (33.9 days) (p=0.006). Mean renal survival days were significantly lower in the high initial DNI group (above 4.75%, 27.8 days) compared with the low initial DNI group (below 4.75%, 53.8 days) (p<0.001) (Fig. 2).
3. Analysis of risk factors affecting patient survival
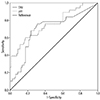
In Cox regression analysis, initial DNI level, initial MAP, initial pH, initial lactate, received renal replacement therapy (RRT) or mechanical ventilation during hospitalization, complications of rhabdomyolysis, arrest during hospitalization, and APACHE II score on first hospital day were significantly associated with mortality. In multivariate Cox regression analysis, DNI and initial pH remained as independent predictors of hospital day mortality (Table 5). ROC curves were drawn for initial DNI (AUC 0.705, 95% CI 0.6–0.811) and, initial pH(AUC 0.761, 95% CI 0.665–0.857) to determine cut-off values predicting mortality (Fig. 3). Mean survival days were significantly lower in the high initial DNI group (above 4.5%, 30.5 days) compared with the low initial DNI group (below 4.5%, 56.3 days) (p<0.001).
Discussion
Chronic excess alcohol intakes and recent binging can lead to AKA with severe metabolic acidosis by a multifactorial process14). Alcohol is metabolized to acetate, which is acidic, by alcohol dehydrogenase and acetaldehyde dehydrogenase2). High serum ethanol concentration inhibits lipolysis, while an alcohol binge makes ethanol concentration decrease, resulting in a significant increase of ketone bodies (particularly β-hydroxybutyrate), which are acidic15). Extracellular volume depletion caused by chronic alcohol ingestion causes peripheral tissue hypoperfusion, resulting in the accumulation of lactic acid.
AKA combined with severe acidosis alters the immunity. Several studies have demonstrated that a moderate amount of alcohol consumption has advantages in the immune system16) however, alcohol abuse is associated with an increased risk of infectious disease. Alcohol abuse increases serum immunoglobulin levels, reduces cell-mediated immunity, reduces lymphocyte numbers, increases macrophage numbers, and alters production of several cytokines617). These immune system changes make the alcohol abuser vulnerable to infection, especially pneumonia18). This change in immunity due to alcohol persists for a considerable period after alcohol withdrawal1920). Several studies have reported postmortem increased CRP levels due to AKA rather than inflammation521). The accumulative oxidative stress of acetoacetate and β-hydroxybutyrate, which are the causative agents in ketoacidosis, is believed to result in inflammatory status and an increase in postmortem CRP22). In addition to alcohol, acidosis caused by alcoholic ketones makes many changes in the body. In vivo and vitro studies showed that in acute metabolic acidosis, the immune response is changed and lymphocyte function is decreased, impairing the immune response2324).
Chronic alcohol consumption causes renal tubular dysfunction and alcoholic ketoacidosis causes renal tubular vacuolization2526). Renal tubular dysfunction limits urinary excretion of ammonium and aggravates the acidosis. In addition, acidosis causes arterial vasodilatation via increased nitric oxide production and decreased cardiac contractility that causes hypotension, aggravating acute kidney injury (AKI)2728). Vomiting and decreased fluid intakes cause volume depletion, and alcohol ingestion causes rhabdomyolysis, resulting in aggravated AKI. AKI in alcoholic ketoacidosis is also associated with poor patient prognosis29). Although there is much controversy about the nephrotoxicity of alcohol and more studies are needed to determine the sequential association of DNI, renal survival, and mortality, our study showed that increased DNI is associated with decreased renal survival and poor prognosis.
Multiple organ dysfunction syndromes (MODS) is known as to occur in about 15% of patients admitted to the intensive care unit (ICU)30) and is responsible for nearly 80% of ICU mortality31). Risk factors for MODS include infection, non-infectious conditions, AKI, and toxic exposure (including alcohol)3031). Although the pathogenesis is unclear, chronic alcohol consumption might act as a toxin, damaging the inflammatory response and resulting in increased vulnerability to MODS. In some reports, a correlation between chronic alcohol consumption and MODS has been found3233). It is noteworthy that the creatinine level is included in the APACHE II, SOFA, and MODS scores which are commonly used as an indicator of MODS. Therefore, AKI in AKA patients represents that they are progressing to MODS.
In our study results, DNI did not show significantly higher sensitivity or specificity or hazard ratios than other tests. However, DNI is a parameter that is reported with other standard hematologic parameters with minimal additional costs and tests for the patients. In contrast, pH, known as a prognostic factor, requires an arterial blood sample. Several scores which reflect MODS, such as SOFA and APACHE II, require multiple tests and calculations. Further studies need to be conducted to determine the exact pathophysiology by which increased DNI is associated with decreased renal survival and poor prognosis, but we suggest that DNI can be used as a quick, economical, and intuitive method to gauge the prognosis of AKA patients without additional testing.
Our study had several limitations. First, this was a single center study with a small number of male patients. Because there were only 12 female patients (after adjusting exclusion criteria there only remains 2) during the 5-year study period, this study included only males. Second, it was a retrospective observational study, and we did not routinely measure beta hydroxyl butyrate and acetoacetate. The emergency department also did not routinely measure procalcitonin (PCT) level, so we could not compare DNI and PCT levels. AKA is known as a benign disease, but it can be fatal if treatment is delayed. We found that DNI may be a simple method to predict renal prognosis and mortality in AKA patients.





 XML Download
XML Download