

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Lymphangiomas are congenital lymphatic malformations that may involve the skin and subcutaneous tissues12. They are rare, accounting for 4% of all vascular tumors and about 25% of children's benign vascular tumors1. More than 90% of cases occur before two years of age1. They can be classified into three groups: cutaneous lymphangioma circumscriptum (CLC), cavernous, and cystic. CLC is the most common type34. Herein, we report a case of CLC that occurred seven years after surgery for soft tissue cystic lymphangioma.
CASE REPORT
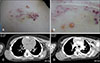
A 9-year-old girl presented with an asymptomatic vesicular lesion on her back, which was noticed a month ago. Physical examination showed a localized plaque composed of yellowish or red-colored vesicles and slightly warty papules (Fig. 1A, B). There was a linear surgical scar about 7 cm long around the lesion. She visited the department of general surgery with a palpable mass seven years ago. Chest computed tomography (CT) was taken at that time. On the chest CT, a mass of about 5.2×2.7 cm was observed on the right posterior chest wall (Fig. 1C). A benign soft tissue tumor was suspected because the boundary was clear and there was no fat attenuation (Fig. 1D). It was finally diagnosed as a 5×3 cm cystic lymphangioma. Seven years later, she revisited with a skin lesion and ultrasound was performed. No soft tissue mass was observed on ultrasound (Fig. 2A). Dermoscopy showed light brownish lacunae with pale septa and dark-reddish areas in some lacunae (Fig. 2B). Therefore, punch biopsy was performed under suspicious diagnosis of cutaneous lymphangioma. Histologic examination revealed a large number of irregularly enlarged lymphatic vessels bordered by very thin lymphatic endothelial cells in the upper dermis. A pale pink lymphatic fluid was observed (Fig. 2C, D). Therefore, the final diagnosis was made of CLC. The patient is undergoing cryotherapy at three-week intervals, and carbon dioxide (CO2) laser ablation therapy once for the remaining lesions. We received the patient's consent form about publishing all photographic materials.
DISCUSSION
CLC is characterized by a clustering of translucent vesicles accompanied by pink, red, or black discoloration as a byproduct of bleeding1. In dermoscopy, it is described as light brown lacunae with presence of clear fluid surrounded by pale septa. When blood infiltrates, dark-red to bluish lacunae are observed leading to hypopyon-like features due to the effect of color transition from dark to bright color5678. This feature is useful for differentiating from haemangioma8. Surgical resection is the choice for primary treatment of lymphangiomas. There were reports that cryotherapy, sclerotherapy, cauterization, and carbon dioxide lasers have been used with good results19.
It was not difficult to diagnose our case because of typical clinical, dermoscopic, and histological findings. However, it occurred around the surgical scar site. The surgery was performed on a soft tissue mass seven years ago. It was very interesting that the mass was a soft tissue cystic lymphangioma. It is known that the recurrence rate is not high in lymphangiomas of 7 cm size or less, if the local excision is performed appropriately10. However, close follow- up is recommended because of the relatively high recurrence rate in children1. In the retrospective study by Alqahtani et al.11, a recurrence rate of 29% was found in 196 lesions of 186 patients during an average follow-up period of 3 years. Sixty percent of patients with relapse, recurred within one year, and eighty percent recurred within three years. It was not uncommon to have lymphangioma circumscirptum associated with cystic lymphangioma121314. In one series of case studies15, 11 of 61 cases of deep lymphangioma, including cavernous lymphangioma and cystic hygroma, were associated with lymphangioma circumscriptum. This probably implies a general developmental disease of the lymphatic system1. In the recurrent form of cystic lymphangioma, there is still no exact epidemiologic data of the ratio to CLC. However, cases were not uncommon where cystic lymphagioma and CLC were displayed together, which suggests that the two types are within the spectrum of lymphatic system malformation16. Therefore, in situations where cystic lymphangioma was incompletely resected, it seems that lymphatic malformation might appear in the superficial form, CLC.
Our patient had remained well without recurrence for seven years after surgery. Suddenly, seven years later, a CLC occurred, confined to the skin. In our case, CLC recurred from cystic lymphangioma, and there was a long interval between occurrences. Prolonged monitoring is needed in lymphangioma patients because relapse is not uncommon. Therefore, we report this case to inform the necessity of prolonged monitoring in lymphangioma patients.

 XML Download
XML Download