

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Acne is a chronic inflammatory disease of pilosebaceous unit. It is a common skin disease affecting approximately 85% of the adolescents12. It is characterized by comedones, papules, pustules and/or nodules; finally, these lesions can cause scars13.
Particularly, facial acne has a considerable psychosocial impact in the affected population. It can cause negative effects on self-image, deterioration in social relations and quality of life and also various psychiatric problems such as anxiety and depression14. In a recent research, it was reported that 26.2% of the people with acne had anxiety symptoms. In acne patients; the impairment of quality of life due to acne was found to be associated with severity of the anxiety symptoms5.
Anxiety sensitivity (AS) is a continuous fundamental fear and defined as extreme fear of anxiety sensations and symptoms6. It is considered as a personality trait and high AS can cause tendency to anxiety disorders (especially panic attack) and alcohol or substance abuse7. It is shown that AS: is a distinct entity separate from trait anxiety that can play a role in anxiety and mood disorders and some other psychiatric disorders8910. AS contributes in the maintenance and exacerbation of a wide variety of chronic physical diseases11. Individuals with AS are prone to respond fearfully to anxiety-related sensations. Despite many studies evaluating anxiety frequency in patients with acne, there is lacking literature on AS of the patients with acne. It was reported that patients with psychodermatological diseases like acne or eczema have higher AS than healthy controls12. In addition, a recent study showed that AS moderated the association between stress and skin-related emotional and social functioning in adults with dermatological disease13.
In this paper we aimed to evaluate the AS in patients with acne. Our hypothesis is that patients with acne have higher AS compared to healthy controls. In addition, the AS scores are negatively correlated with quality of life scores in acne patients.
MATERIALS AND METHODS
The study was performed between February 2017 and June 2017. Eskisehir Osmangazi University of Local Ethics Committee (decision no: 2017/02) approved the study protocol before the initiation of the study. Acne patients and healthy controls were informed and informed consent form was signed. Each individual participating in the study was informed of the right to withdraw from the study at any time. Participants were selected subsequently from patients with acne who had applied to our department and met the inclusion criteria. For the healthy control group, snowball technique was used for forming the healthy control group which was mostly consisted of hospital personnel. Patients younger than 16 years and with primary neurological disorders, mental retardation, cognitive mental disorders (i.e., dementia and delirium), and psychotic disorders (i.e., schizophrenia, delusional disorder, bipolar affective disorder) were excluded from the study.
Demographic data of the participants were recorded. Severity of acne was evaluated by Global Acne Grading System (GAGS). All volunteers were asked to fill anxiety sensitivity index-3 (ASI-3), Beck anxiety inventory (BAI) and Turkish version of acne quality of life index (TAQLI).
Accordingly GAGS, scores are calculated by lesion localizations's factor coefficients (forehead: 2, left cheek: 2, right cheek: 2, nose: 1, chin: 1 and neck, chest and back: 3) multiplying with lesion scores (no lesion: 0, comedone: 1, papule: 2, pustule: 3, nodule: 4) and scores of each region are collected. Finally, severity of acne is classified as no (0 point), mild (1~18 points), moderate (19~30 points), severe (31~38 points) and very severe (>39 points)14.
ASI had been defined by Reiss et al.7 in 1986. Later, ASI was revised and a well validated version ASI-3 was developed715. ASI-3 comprised 3 subscales: physical, cognitive and social. Physical subscale assesses fear of physical symptoms, e.g., be afraid of heart beats rapidly. Cognitive subscale assess fear of losing cognitive control, e.g., be afraid of losing mind. Social subscale assess fear of someone will be aware of their anxiety symptoms, e.g., be afraid of redden in front of society. ASI-3 consists of 18 questions. Each question scored between 0 and 4. The total score can range between 0 and 72, the subscale score range between 0 and 24. Higher total scores on this scale suggest higher AS levels and fear of anxiety symptoms. The Turkish form of ASI-3 was shown to be valid and reliable6.
BAI is used to determine the frequency of anxiety symptoms. It includes 21 questions. Each question scored between 0 and 3. Higher total scores on this scale suggest higher anxiety levels. The validity and reliability of the Turkish version of the BAI was conducted16.
TAQLI consists of 11 questions. Each question scored between 0 and 4. The total score can range between 0 and 44. Higher total scores on this scale suggest more impairment in the quality of life17.
IBM SPSS Statistics ver. 21.0 software (IBM Corp., Armonk, NY, USA) was used for the data analyses. Continuous data was presented as mean±standard deviation and median (Q1~Q3). Categorical data was presented in percentage and frequency values. Normality was analyzed by Shapiro–Wilk test. Mann–Whitney U test was used to determine the differences between the BAI and ASI scale scores of the two groups and Kruskal–Wallis H test was used to determine the differences between the BAI, ASI and TAQLI scale scores of the three groups. The Spearman correlation test was used to determine the direction and magnitude of the relationship between the scale scores. p<0.05 value was accepted to be statistically significant.
RESULTS
A total 214 acne patients and 117 healthy controls were enrolled in the study. Mean ages (±standard deviation) in acne and control groups were 21.26±3.73 and 21.95±3.39 respectively. One hundred and ten of the acne patients were male, 104 were female; 60 of the healthy controls were male, 57 were female. No significant differences were observed on the age and sex (p>0.05). Mean disease duration (±standard deviation) was 4.27±3.28 years (min: 1~max: 18).
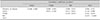
Mean ASI-3 total, social, physical subscale, and BAI scores were significantly higher in acne patients compared with controls (p<0.001, p<0.001, p=0.032, p<0.001, respectively) Mean ASI-3 cognitive subscale score was not significantly different between acne patients and controls (p=0.382) (Table 1).
Mean TAQLI score was 16.71±8.71 (min: 0~max: 40) and mean GAGS score was 14.76±8.17 (min: 2~max: 38) in acne patients. Based on GAGS scores, a total of 150 patients (70.1%) had mild, 54 (25.2%) had moderate and 10 (4.7%) had severe acne. The mean ASI-3 total, BAI, and TAQLI scores were not significantly different according to the severity of acne (p=0.147, p=0.871, p=0.556, respectively) (Table 2).
In Spearman correlation test, there was significant correlation between TAQLI, BAI and ASI-3 total scores in subjects with acne (p=0.014, p=0.019, respectively); but there was no significant correlation between disease duration and BAI and ASI-3 total scores (p=0.935, p=0.951, respectively). Similarly, there was no significant correlation between GAGS scores and BAI and ASI-3 total scores (p=0.872, p=0.080, respectively) (Table 3).
DISCUSSION
These results support our hypothesis that patients with acne have higher AS compared to the healthy controls. Specifically, social and physical aspects of AS was found to be significantly higher. These findings suggest that individuals with high AS are more likely to be aware of the social and physical effects of physiological symptoms associated with stress or skin disease. Psychological stress is thought to be related to many common skin diseases and can trigger onset of these diseases or exacerbate18. Anxiety can trigger onset of acne or aggravate too. Acne most commonly affects adolescents; that is an important period for physical, social and emotional development. Lower self-confidence, deterioration in social relations and quality of life and also various psychiatric problems have been seen in patients with acne14. Moreover, psychosocial impact of acne that started in adolescence period can affect whole life of the individual. It has also been reported that acne severity is associated with low social status1.
Impairment of quality of life in patients with acne is reported to be similar to in patients with other chronic diseases such as asthma, epilepsy, diabetes, back pain and arthritis19. Lukaviciute et al.3 reported that quality of life was impaired in 96.5% of patients with acne. Our results are consistent with these results. Impairment of quality of life is often higher than assessed by the clinician. Severity of acne and its effect on quality of life may not be always correlate. Impairment of quality of life is observed even in patients with mild acne20. Similarly, in our study, there was no significant difference in the mean TAQLI scores of patients with acne according to severity of acne (p=0.556). Various psychiatric problems are common in acne patients. In a previous study, it was reported that 56.1% of the patients with acne had various psychiatric problems. The most common psychiatric problem was anxiety3. Golchai et al.21 reported that 68.3%, Lukaviciute et al.3 38.4% of patients with acne had anxiety. In our study, the mean BAI score was significantly higher in acne patients compared with healthy controls. The mean BAI score was higher in severe acne patients than mild-moderate but there was no significant difference. As being a disease that often affects the face and may cause anxiety due to the cosmetic defect in individuals.
There are numerous studies investigating the anxiety frequency in patients with acne; however, AS has never been investigated. Being as a distinct entity separate from trait anxiety, AS is based on the belief that anxiety symptoms have detrimental physical, cognitive, or social consequences. For example, person with high AS may be afraid of sweating, believing that it can be considered a sign of a serious illness or a sign of weakness by others6812. It is thought that AS may be associated with various psychodermatological conditions and high AS may increase anxiety responses and severity of dermatological symptoms1218. There are only two studies evaluating AS in dermatological diseases in the literature1213. AS was reported to be significantly higher in psychodermatological diseases (psoriasis, rosacea, acne, etc.) than in non-psychodermatological diseases (sunburn, skin cancer, keloid, etc.)12. Similarly, in our study the mean ASI-3 total score was significantly higher in patients with acne and it was higher in patients with severe acne than mild-moderate but there was no significant difference.
TAQLI score was correlated with BAI and ASI-3 total scores in patients with acne but there was no significant correlation between disease duration, GAGS scores, BAI and ASI-3 total scores. These results show that anxiety and AS may be high in patients with acne, regardless of severity and duration of disease and quality of life decreases as anxiety and AS increase. Therefore, even if severity of acne is mild, patients should be evaluated psychologically. A recent study reported that association between stress and skin-related emotional and social functioning in adults with skin disease was moderated by social AS13. Our study reports similar results with the study of Dixon et al.12 specially for acne, the main difference is that not only the social AS but also the physical AS was found to be significantly higher. As there are numerous ways for presentation of skin diseases, there might be several psychological mechanisms underneath and authors should evaluate every skin disease in regards to psychological components one by one specifically.
It is important to define the level of AS; because AS can be reduced by short, low-cost interventions22. Cognitive behavioral treatments may reduce AS23. Initially, cognitive behavioral treatments were developed for individuals with anxiety disorders; however, it has been reported to be effective in the treatment of pain associated with anxiety and irritable bowel syndrome2425. Dixon et al.12 suggested that cognitive behavioral treatments may be beneficial for psychodermatological diseases such as acne. Also, in a previous study, cognitive behavioral therapy is found to be beneficial in patients with acne when added to conventional medical treatments26. Reducing the AS levels of acne patients may decrease their anxiety levels and increase their quality of life however further research is needed to examine the efficacy of cognitive behavioral treatments in acne patients.
In our study, we found that patients with acne had impaired quality of life, higher anxiety and higher AS. According to severity of acne, there was no significant difference in TAQLI, BAI and ASI-3 scores. We also found a negative correlation between quality of life and anxiety, AS in patients with acne. However, there was no correlation between disease duration, severity of acne, anxiety, AS and quality of life.
The main limitations of this study were its cross-sectional design and the usage of the self-rating scales. Besides, the selection of the healthy controls from the hospital personnel with snowball technique might be another limitation.
To our knowledge, our study is the first to report that AS is high in acne patients. Clinically, our results suggest that there might be a relationship between AS and acne. The association between higher AS and acne is not clear. Is AS a cause or a result of acne? isn't exactly known. We conclude that further studies are needed in order to clarify the relationship between acne and AS and to investigate the ef ficacy of cognitive behavioral treatments in acne patients.


 XML Download
XML Download