

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Langerhans cell histiocytosis (LCH) is a rare disorder characterized by the proliferation of dendritic cells, thereby resulting in local or systemic symptoms. The most recent classification for LCH is based on a treatment protocol recommendation made by the Histiocyte Society1. Unifocal disease (eosinophilic granuloma) is a single-system (SS) disease involving a single site. The Hand–Schüller–Christian disease is a multifocal SS disease that presents with multiple sites of involvement in a single organ system, while Letterer–Siwe disease is a multifocal multisystem (MS) disease that presents as multiple involved sites in more than one organ system. MS LCH is further subdivided into RO+/RO− depending on whether or not a risk organ (RO) (e.g., hematopoietic system, liver, and/or spleen) is included. Central nervous system (CNS)-risk areas include the sphenoid, orbital, ethmoid, and temporal bones, and this represents an increased risk to the central nervous system2.
The clinical symptoms of patients with LCH depend on the site and the degree of involvement. Posterior mandible involvement is seen in 10% to 20% of LCH patients with intraoral lesions3. Oral manifestations include gingival pain, ulceration, enlargement, inflammation, or recession, and mobility of the teeth due to expansion of alveolar bone4. Dental radiographs may show discrete destructive bone lesions that can cause the teeth to appear as if they are “floating on air”5. Periosteal new bone formation and slight root resorption may also be present6.
This article describes two case histories of unifocal bony LCH with mandibular involvement and further discusses the appropriate management of such cases with via a review of the literature.
II. Cases Report
1. Case 1
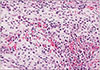
A 5-year-old female patient visited our clinic with complaining of swelling in the right mandibular region.(Fig. 1) The patient was initially evaluated in the local pediatric clinic, and her symptoms were alleviated after a course of antibiotics. However, her symptoms returned, and the patient was admitted to a nearby university dental hospital. The patient underwent numerous tests, including computed tomography (CT), and she finally visited our hospital because of suspected malignancy. The patient had no medical history or prior systemic symptoms (e.g., fever, weight loss, skin rash, or polyuria). Clinical examination revealed swelling of the right mandible and pain in the affected area. On panoramic examination, specific findings were difficult to locate, but osteolytic findings were observed on CT, including a well-defined, buccolingual, expansile lesion. A profuse periosteal reaction was also observed around the lesion. The following laboratory tests were performed: complete blood count with differential, chemistries with liver and renal function and electrolytes, total protein, albumin, quantitative immunoglobulins, erythrocyte sedimentation rate, lactate dehydrogenase, ferritin, uric acid, and urinalysis. An incisional biopsy was performed and revealed LCH (CD1a/S-100 positive) on immunohistological staining.(Fig. 2) The patient was transferred to the pediatric department to clarify the extent of her disease and to determine the appropriate treatment method. Systemic examinations (e.g., magnetic resonance imaging [MRI] and bone scan) were performed, and the patient was diagnosed with unifocal disease. After corticosteroid therapy (prednisolone 5 mg×2.5 Tab. three times a day for 1 month), the patient is in complete remission; the bone scans reveal no abnormal uptake in the right mandible, and the MRI shows no definite findings suggestive of active LCH.(Fig. 3)
2. Case 2
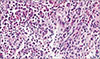
A 9-year-old male patient was referred to our clinic from the Department of Pediatric Dentistry due to a history of unhealed mandible swelling, mobility of a deciduous molar tooth, and gingival swelling.(Fig. 4) One month prior to presentation, the patient experienced pain while touching his gingiva, and he visited a local dental clinic because the symptoms did not subside. The patient underwent endodontic treatment on #84, which was performed 2 years ago. Antibiotics were repeatedly prescribed by the local dental clinic. After a CT image revealed an abnormality, the patient was transferred to our clinic. Clinical examination revealed swelling of the right mandible, pain in the affected area, mobility of #85, and gingival swelling and bleeding. Panoramic examination revealed no specific findings, but osteolytic findings were observed on CT, including a well-defined, buccolingual, expansile lesion. A profuse periosteal reaction was also observed around the lesion. The following laboratory tests were performed: complete blood count with differential, chemistries with liver and renal function and electrolytes, total protein, albumin, quantitative immunoglobulins, erythrocyte sedimentation rate, lactate dehydrogenase, ferritin, uric acid, and urinalysis. An incisional biopsy with the patient under general anesthesia confirmed the presence of LCH (CD1a/S-100 positive).(Fig. 5) The patient was transferred to the pediatric department in order to determine the extent of the disease and the appropriate treatment protocol. Systemic examinations (e.g., MRI and bone scan) were performed, and the patient was diagnosed with unifocal disease. Corticosteroid therapy (prednisolone 5 mg×2.5 Tab. three times a day for 1 month) was administered. After 6 months, several suspicious enlarged bilateral lymph nodes in the neck, mediastinum, and both lung hilar areas were noted, and the patient was considered to be in partial remission. No significant findings were discovered during the patient's follow-up period.(Fig. 6)
III. Discussion
LCH is a rare disease, and the true incidence is unknown. According to a nationwide retrospective survey conducted in Korea, LCH has been reported to occur in about 24 cases per year (603 patients between 1986 and 2010). The incidence was greater in male patients than in female patients (ratio of 1.4:1), and the median age at diagnosis was 65 months. The bone was the most frequently affected organ (80%)7.
The pathogenesis of LCH is unclear, and recent studies suggested that LCH is a monoclonal neoplasm because a V600E mutation is repeatedly found in the rapidly accelerated fibrosarcoma isoform B (BRAF), which regulates cell survival, proliferation, motility, and cell differentiation in cell signals8.
Oral symptoms are common in LCH, and they are the usual chief complaints of patients upon their initial visit to the clinic. Patients usually present with pain and swelling. Radiographic images may reveal “floating teeth” in advanced disease, while destructive, ill-defined, osteolytic lesions are commonly found in a panoramic radiological view. However, it is difficult to discern buccolingual periosteal reactions on x-rays. Periosteal reaction and “punch-out” radiolucency without a corticated border are clearly observed on CT images. Due to the destructive nature of LCH, it is commonly confused with osteomyelitis or malignancy. Therefore, a differential diagnosis based on patient age and radiologic features is useful. Squamous cell carcinoma commonly shows a solitary ill-defined radiolucency, and it may be associated with a soft tissue mass. Sequestrum is a “hallmark” manifestation of osteomyelitis. In particular, LCH must be differentiated from other histological and dendritic cell diseases by histopathologic and immunophenotypic findings (CD1a, S-100) on biopsy. In our cases, each patient presented with a destructive, ill-defined osteolytic lesion, periosteal reaction on CT images, and a positive immunophenotype (CD1a, S-100) reaction on the incisional biopsy samples. Hence, a diagnosis of LCH could be confirmed.
SS LCH has a good prognosis, with 5-year overall survival rates in SS, MS-RO−, and MS-RO+ groups being 99.8%, 98.4%, and 77.0%, respectively, and the 5-year recurrence rates are 17.9%, 33.5%, and 34.3%, respectively7. Treatment is dependent on the degree of organ involvement, solitary or multiple lesions, and higher risk lesions. There is no universally accepted protocol for the treatment of solitary LCH lesions without CNS involvement (orbits, mastoids, or temporal bones) due to its good prognosis9. Numerous treatment options include observation only, surgical curettage, radiation therapy, steroid injections, and chemotherapy. Solitary lesions are often treated with curettage after biopsy, and they have shown low rates of recurrence. However, a minimally aggressive approach has often been suggested as of late910. Hence, after systemic involvement evaluation in both of the present cases, the primary treatment consisted of steroid medication (prednisolone). Higher risk patients with MS disease and those with CNS-risk bone involvement require systemic therapy with vinblastine and prednisone rather than surgery, radiotherapy, or single-agent chemotherapy11.
Due to the low incidence of LCH, multicenter studies are essential for establishing appropriate treatment protocols. Although there are several retrospective LCH epidemiological studies in Korea, research in the dental field is rare, and there are no detailed dental guidelines. However, several guidelines have been published, and they recommend monitoring tooth development and jaw growth in the management of jaw involvement and confirmed LCH12. Studies on LCH diagnosed through oral symptoms, as well as those describing episodes that patients experience before the diagnosis of LCH, will be particularly significant.
Early screening and a differential diagnosis including LCH are essential for young or pediatric patients with osteolytic lesions. We recommend a pediatric transfer for patients diagnosed with LCH for a thorough systemic evaluation of possible multiple organ involvement. In addition, our hospital recommends systemic steroid medication as a treatment protocol.




 XML Download
XML Download