

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Presentations of patients with unilateral cleft lip/palate range from clefts involving only the vermilion to full-thickness clefts involving all tissue layers. These variations in cleft lip presentation have led to the development of different repair techniques1 that have been employed over the years to repair unilateral cleft of the lip2. These techniques can be grouped into two broad groups: straight line techniques and those based on geometrically designed flaps3.
Straight line techniques have the potential for scar contracture with consequent shortening of the lip, as excess normal tissue along the cleft margins is sacrificed to achieve straight-line closure and the shape of Cupid's bow is blunted3. These shortcomings have led to the use of geometrically designed flaps. Theoretical advantages of geometric techniques include applicability to a wide range of cleft sizes, the ability to symmetrically recreate Cupid's bow, achievement of adequate rotation and lip length, increased fullness of the philtral tubercle, and minimal wasted tissue45.
The two basic techniques that are in use for unilateral cleft lip repair, Tennison–Randall and Millard rotation-advancement techniques, are both variants of geometrically designed flap techniques. Both techniques recognize the importance of repositioning the lip muscle (orbicularis oris) in the correct anatomic orientation to achieve aesthetic as well as functional improvement6. These two techniques are the two most frequently employed techniques in Nigeria, where this study was conducted.
The ideal operation for repair of a unilateral cleft lip should result in a symmetrical upper lip with equal philtral column length on either side7. The scar should mirror the opposite side and should not transgress the philtral column7. There should also be no peaking at Cupid's bow at the cleft side or notching of the vermillion. In addition, Cupid's bow should be of adequate proportions7. Christofides and others opined that these criteria should be obtainable in a single operation without multiple minor revisional procedures8.
Because of variations in the sequence and timing of techniques, as well as the skills and experience of individual surgeons, the range of outcomes of treatment of cleft lip and palate can be considerable8; thus, evaluation of treatment outcomes is essential for identification and implementation of the highest possible standards of care79. In this regard, nasolabial appearance is, arguably, one of the most important measures of the success of treatment for unilateral cleft lip10, as it allows aesthetic correction of the deformity and progressive, balanced, development of the mid-face11. Methods to assess nasolabial appearance can be broadly divided into qualitative and quantitative methods. The latter methods aim to analyze the extent of abnormal morphology and the degree of disproportion objectively through facial measurements12. Qualitative methods are more subjective and involve analyses of facial esthetic and appearance impairment using scales, indices, scoring systems, and rankings. Subjective assessment of appearance and aesthetics is fraught with difficulty, but is most likely to reflect the patient's and general public's perception of facial impairment13.
There appear to be no published studies on the evaluation and comparison of these two basic treatment techniques in Nigeria. The purpose of this study was to evaluate and compare the treatment outcomes of surgical repair of unilateral cleft lip using either Tennison–Randall or Millard techniques based on (qualitative) parent/subject and professional assessment.
II. Materials and Methods
This was a prospective, randomized, controlled study of the treatment outcomes of surgical repair of unilateral cleft lip using either the Tennison–Randall or Millard techniques in Lagos University Teaching Hospital (Idi-Araba, Nigeria) between January 2013 and July 2014. A total of 56 subjects with unilateral cleft lip presenting for primary surgery who satisfied the ‘rule of 10’ were recruited for the study. Subjects with bilateral cleft lip and those who had undergone initial cleft surgery were excluded from the study.
The study was approved by the Health Research and Ethics Committee of Lagos University Teaching Hospital (approval No. 34512). Written informed consent was obtained from all subjects who were 16 years or older, and from the parents/guardians of subjects younger than 16 years before enrollment in the study. Subjects were randomly allocated to the two surgical technique repair groups through the use of balloting, namely a box containing sealed envelopes with 56 folded pieces of paper on which either “A” or “B” had been written. There were 28 pieces of paper with “A” and 28 with “B”. Subjects/guardians were asked to pick from the box after it had been thoroughly shaken. Group A were operated on using the Tennison–Randall technique, while group B were operated on using the Millard rotation advancement technique. Preoperatively, age, sex, weight, height, and type of cleft were recorded and cleft lip and palate were classified according to Kernahan and Stark14 as modified by the international confederation for Plastic and Reconstructive Surgery in 197115.
1. Preoperative evaluation
Routine preoperative blood investigations including hemoglobin estimation, electrolyte, urea and creatinine levels, and electrocardiography were done for each subject. Echocardiography was also done when indicated. Subjects were referred to the pediatrician for clinical evaluation to rule out cardiovascular congenital anomalies, upper respiratory tract infection, ear infection, and other congenital anomalies that could be of clinical significance. Subjects were at least 3 months old, 4.5 kg (10 pounds), and had a minimum hemoglobin concentration of 10 g/dL.
2. Operative procedure
In subjects less than 12 years of age, surgical repair was done under general anesthesia with endotracheal intubation, while repairs for subjects above 12 years of age were done under local anesthesia with 2% xylocaine with adrenaline 1:80,000. Surgical repair was carried out by two consultant oral and maxillofacial surgeons experienced in cleft lip and palate surgery. One of the surgeons exclusively used Tennison–Randall's triangular technique16, while the other exclusively used Millard's rotation advancement technique17.
Postoperatively, sufratulle dressing was applied to the wound for the first 24 hours, and this was then followed by gentle daily cleansing with sterile normal saline applied with gauze swabs until the sutures on the skin were removed after 7 days. Closure of the surgical incision was done in layers using a 17.5 mm curved cutting needle. Vicryl (polyglactin) 4/0 was used for mucosa and muscles and nylon 4/0 for skin in both groups of patients.
Subjects were reviewed weekly for two weeks post-surgery, and then once every month for 3 months to evaluate surgical outcome.
3. Evaluation of surgical outcome
Surgical outcome was assessed at 3 months using a qualitative method based on a modified form of the criteria described by Christofides et al.7.(Appendices 1, 2) This evaluation was carried out by both the subjects/guardians (Appendix 1) and independent assessors.(Appendix 2) Scoring indices essentially assessed the appearance of the residual lip scar and nose.
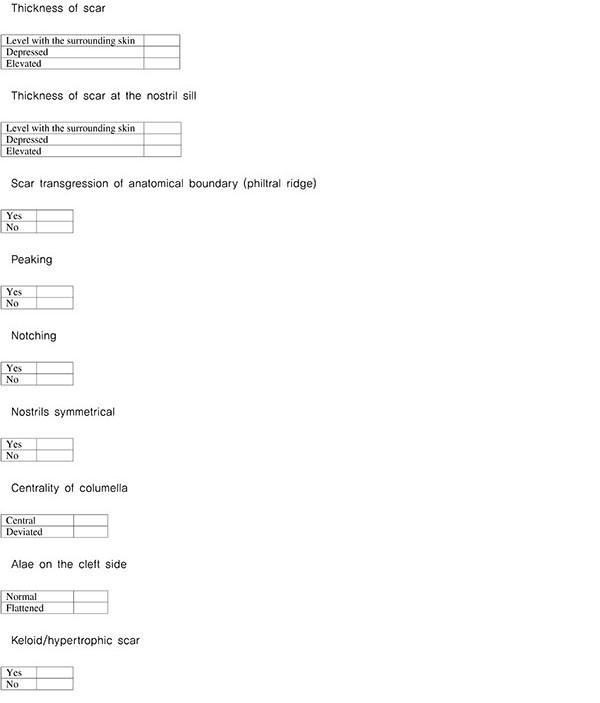
Evaluation was carried out by two experienced surgeons (different from the operating surgeons) and the researcher. The three assessors met before commencement of the project to study the modalities of the scoring index. Initially, assessments were done independently and then together by the three assessors to resolve any differences in their findings. Final assessments were reached by consensus. Clinical evaluation was performed using modified criteria—scar transgression of the philtral ridges, symmetry of nostrils, and centrality of the columella, thickness of the lip scar, thickness of the scar at the nasal sill, peaking, notching—as described by Christofides et al.7 and as shown in the evaluation form. (Appendix 2)
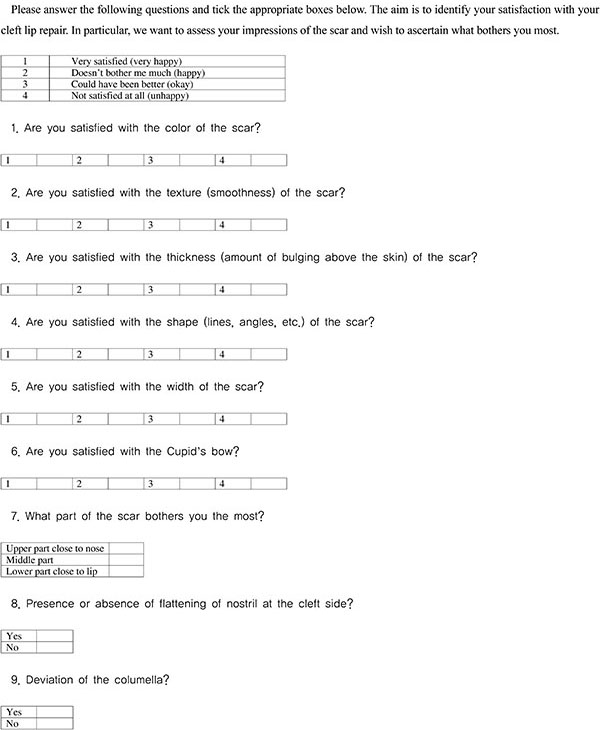
For the second part of the qualitative assessment, the parents/guardians completed a questionnaire to assess satisfaction with treatment of their ward. The questionnaire was interpreted for the patients/guardians if they were not literate. The questionnaire consisted of evaluation of satisfaction with scar and nose appearance. Color, shape, and thickness of the scar were used to assess the patients/guardians opinions of the residual lip scar (Appendix 1), while the presence or absence of flattening of the nose at the cleft side, as well as deviation of the columella were used to assess the nose.(Appendix 1)
4. Data analysis
Data were analyzed using the SPSS for Windows (ver. 17.0; SPSS Inc., Chicago, IL, USA). Proportions and percentages were compared between groups using the chi-square test. Inter-rater reliability analysis using Cohen's kappa statistic was also performed to determine coherence among raters (inter-rater reliability was 0.85, 95% confidence interval). A significance level of P≤0.05 was used.
III. Results
1. Sex distribution of the subject population
A total of 56 subjects requiring repair of unilateral cleft lip were enrolled in this study and analyzed. Twenty-eight subjects each were assigned to the Millard group and Tennison–Randall (TR) group. Of the 56 subjects, 32 subjects (57.1%) were males and the male:female ratio was 1.3:1. There were 15 males (53.6%) and 13 females (46.4%) (ratio of 1.2:1) in the Millard group and 17 males (60.7%) and 11 females (39.3%) (ratio of 1.6:1) in the TR group. There was no significant difference in sex ratio between the Millard and TR groups (P=0.589).
2. Age distribution of subjects
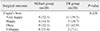
The age of subjects at the time of lip repair ranged from 3 months to 51 years. Highest number of lip repairs was done within 3–6 months in both groups; Millard group, 21 subjects (75.0%) and TR group, 17 subjects (60.7%).(Table 1) There was no significant difference in age distribution between the two groups (P=0.408).
3. Pattern of cleft lip and palate distribution
Unilateral cleft lip, alveolus and palate was the commonest type of cleft deformity in the study (n=23, 41.1%). There were more cleft deformities on the left side (n=35, 62.5%) than on the right side (n=21, 37.5%), corresponding to a ratio of 1.8:1. More males than females presented with cleft lips (32 [57.1%] vs 24 [42.9%]), corresponding to a male:female ratio of 1.33:1.
In the Millard group, unilateral cleft lip, alveolus and palate was the commonest type (n=12, 42.9%). A higher number of cleft lips were seen on the left side than on the right side (19 [67.9%] vs 9 [32.1%]).
In the TR group, 11 patients (39.3%) each had cleft lip only versus cleft lip, alveolus and palate, while cleft lip and alveolus was seen in six subjects (21.4%). More cleft lips (n=16, 57.1%) presented on the left side than on the right side (n=12, 42.9%). There was no difference in the distribution of cleft lip patterns between the two groups.(Table 2).
4. Subject evaluation of surgical outcomes
In the evaluation of the color, texture, thickness, shape, and width of the scar, the vast majority of subjects/guardians (92.9%; 52 of 56) were very happy with the repair regardless of whether Millard or TR repair was used. There was no significant difference in subject/guardian satisfaction between the two groups (P>0.05).(Table 3)
While six of the 28 subjects (21.4%) who had surgical repair in the Millard group were not happy with the Cupid's bow, only two of the 28 subjects (7.1%) in the TR group were unhappy with the Cupid's bow. This difference, however, was not statistically significant (P=0.428).(Table 4)
While 15 of the 28 subjects (53.6%) in the TR group were more bothered about the surgical outcome of the lower part of the scar close to the lip, 12 of the subjects (42.9%) in the Millard group were more bothered about the upper part of the scar close to the nose. This difference was statistically significant (P=0.028).(Table 3)
Twenty-five of the 28 subjects (89.3%) in the Millard group judged the nostrils to be flattened, while 19 out of the 28 subjects (67.9%) in the TR group judged the nostrils to be flattened. This difference between groups was statistically significant (P=0.035).(Table 5)
There were more deviated columella in the Millard group than in the TR group (22 [78.6%] vs 16 [57.1%]), but this difference was not significant (P=0.086).(Table 5)
5. Assessor evaluation of surgical outcomes of the Millard and TR groups
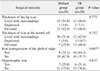
The assessors judged the scar on the lip to be level with the surroundings in 15 subjects (53.6%) in the Millard group and 13 subjects (46.4%) in the TR group. This difference was not statistically significant (P=0.773).(Table 6) Although the number of the patients (n=20, 71.4%) judged to have a levelled scar at the nostril sill in the Millard group was greater than in the TR group (n=12, 42.9%), this difference was not statistically significant (P=0.152).(Table 6)
There was one more hypertrophic scar in the Millard group (n=7, 25.0%) than in the TR group (n=6, 21.4%), a nonsignificant difference.(Table 6)
Assessors observed a striking disparity in scar transgression of the philtral ridge in the two groups. This was present in 32.1% (n=9) of subjects in Millard group but 64.3% (n=18) of subjects in the TR group (P=0.007).(Table 6)
In contrast, more peaking and notching were noticed in Millard repair than TR repair (13 and 10 vs 8 and 6, respectively), but this was not statistically significant (P>0.05). (Table 7)
More nostrils were asymmetrical, more columellas were deviated, and more alae were flattened in the Millard group than in the TR group but without statistical significance (P>0.05).(Table 8)
IV. Discussion
Evaluation of treatment outcomes is essential for identification and implementation of the highest possible standards of care818. Few studies have compared the outcomes of different repair techniques of unilateral cleft lip51920212223242526, and even fewer have compared the two most commonly used techniques2728.
Nasolabial appearance is arguably one of the most important measures of the success of treatment for cleft lip repair10. Thus, we used nasolabial appearance to assess treatment outcomes in this study, consistent with previous studies526. Similarly, a residual scar in the nasolabial region as a result of cleft surgery has been used by various authors7232728 to assess the success of cleft lip repair. Most studies9293031 have concluded that increasing the number of assessors improves reliability and minimizes inter-examiner bias. Therefore, in our study, assessment was performed by three raters to reduce inter-rater bias.
Patient perception of the repair are a major consideration when evaluating outcomes of cleft repair731. Most respondents in our study were very happy with the appearance of the scar and therefore the repair in both Millard and TR groups (92.9%). This means that surgical repair of unilateral cleft lip is important and can provide hope to distressed parents and patients. This is in agreement with prior studies72332 where the majority of repairs with either technique were judged to be good by the parents/patients.(Fig. 1) A plausible explanation for this is that the parents/patients see the repair as a considerable improvement of the deformity. Other reasons for this are that parents/patients trust caregivers, and that they are concerned that complaints from them would be perceived as not appreciating the caregivers33. Respect for caregivers is another potential reason for the high satisfaction rates reported for parents/patients32.
Twenty-one percent of the respondents in the Millard group and 7% in the TR group were not satisfied with the Cupid's bow. Millard repair has been criticized by various authors192334 as producing a wider than normal Cupid's bow. In contrast, TR repair produces a near normal Cupid's bow192234. We did not find one technique superior to the other with respect to Cupid's bow. This may be related to the ability of the Millard's surgeon in this study to produce a normal-looking Cupid's bow.
Differences in the responders' perceptions of what part of the scar bothered them most revealed significant differences between the two techniques. Previous studies reported that both techniques produce a scar that bothers the patients/guardians7233435. In this study, 43% of repairs in the Millard group produced a scar on the upper part of the lip that bothered the patient, while 53% of repairs in the TR group produced a scar on the lower part of the lip that bothered the patient.(Fig. 2) The scar on the upper part of the lip after Millard correction has been reported to be due to the rotation incision in the upper part of the lip, while the scar on the lower part of the lip after Tennison–Randall repair is generally agreed to be due to the triangular flap made in the lower part of the lip722.
There is consensus that Millard cleft lip repair produces better nasal symmetry than TR repair1925. However, we found significantly more symmetrical noses in TR than in Millard repair subjects. This might be due to other factors not explored like width of the cleft and the skill of the surgeon19. The outcome of nasal repair becomes worse as the width of the cleft deformity increases, but an experienced and skillful surgeon is able to achieve a good nasal appearance even in wide cleft deformities. However, various authors3637 have proposed the use of a presurgical orthopedic technique for wide cleft deformity.
Columella deviation was higher in the Millard group than in TR group, but, unlike nasal symmetry, this was not significant. This, however, is in agreement with an earlier study by Abdurrazaq et al.32; these authors also reported poor nasal symmetry in the Millard group. Although primary rhinoplasty was not done after Millard repair1 in this study, the problem of an asymmetric nose even after primary nasal repair is well documented838.
With regard to the assessor evaluations, only scar transgression of the philtral ridge was judged to differ between the two techniques. This coincided with ‘the part of the scar that bothers me the most’ in the guardian/patient evaluation. This is in agreement with prior studies7233435 that also reported a high percentage of scar transgression of the anatomical boundary with TR repair. In contrast, Holtmann and Wray27 and Chowdri et al.28, while working on 35 and 108 randomly selected patients, respectively, concluded that there was no significant difference between the two techniques in terms of transgression of the residual scar. Both techniques have been reported to produce a scar that transgresses a known anatomical boundary. Millard's technique transgresses the philtrum at the upper part due to the rotation incision, while TR transgresses it at the lower part due to the triangular flap that inserts in the medial element22.
There was a higher incidence of peaking and notching in the Millard group than the TR group, but this was not significant. High incidence of peaking, and notching in particular, has been noted in Millard repair by various studies7233439. The most obvious reason for this notching is straight line closure of the vermilion. However, unequal width of the lateral and medial cleft segments might also play a role depending upon the disparity in thickness on both sides of the cleft40. Bilwatsch et al.22 and Cheema et al.39 reported inadequate rotation of the medial element and turning in of the sutured edges as other causes of notching. Another factor may be an incision in the lateral lip segment that is made too far medially, thus going beyond the maximum vermilion thickness where all three segments (vermilion, skin, and muscle) are underdeveloped. Measures to prevent lip notching suggested in the literature include the use of the Noordhoff triangular flap to compensate for deficiency of the vermillion on the non-cleft side, adequate rotation of the medial element with a back cut that does not violate the vermilion, and adequate undermining of the skin and mucosa limited to a few millimeters from the edges40.
Nasal symmetry, columella centrality, and ala symmetry were all rated higher in the TR group than the Millard group, but without statistical significance. This is similar to what was reported by Holtmann and Wray27, Chowdri et al.28, and Fudalej et al.35, in other words no difference between these two techniques in nose appearance assessments.
Hypertrophic scars, of which more occurred in the Millard group than in the TR group, have also been reported in prior studies727283435. Hypertrophic scar is defined as the accumulation of excessive collagen leading to raised scar that does not exceed the boundaries of the wound41. Although no definite relationship between the type of suture material used and formation of a hypertrophic scar has been established in the literature, some suture types such as silk and catgut have been reported to elicit a strong inflammatory reaction when used on the skin2. This might result in excessive formation of fibrous tissue, probably leading to hypertrophic scar formation42. However, we used nylon sutures for repair in this study, which have been noted to elicit very little or no inflammatory reaction2. There is speculation that hypertrophic scarring might be technique biased42. However, verification of this will require a highly controlled study.
Essentially, we found no major differences in the overall results between Millard rotation-advancement repair and Tennison–Randall repair. Tennison–Randall lip repair is one of the most widespread primary reconstruction methods. The most important contributions of this technique to cleft surgery are recognition and preservation of Cupid's bow by lowering the peak in the margin of the cleft22. In contrast, the Millard rotation-advancement technique17, introduced in 1957, has been reported to be the most widely used procedure for cleft lip repair because it places most of the scar along the natural philtral border and is more flexible than geometric closure techniques. Moreover, the Millard technique allows for complete muscular repair and minimizes the discarding of normal tissue.
Most cleft lip repairs were judged to be satisfactory by the guardians/subjects regardless of repair technique used. The main differences in outcomes between the two techniques were the location of the scar that the subject or guardian felt was the most bothersome, and the presence of nasal flattening at the cleft side. The upper part of the scar close to the nose was considered abnormal after Millard repair, while the lower part of the scar close to the lip was considered abnormal after Tennison–Randall repair. Coincidentally, assessors noted a difference in lip scar transgression of the philtral ridge between the two techniques. This suggests that both the Millard and Tennison–Randall techniques require significant improvements to improve the appearance of the scar on the upper and lower parts of the lip, respectively.








 XML Download
XML Download