

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
1. Background
With the growth of the older population and increased life expectancy, social attention is being focused on older adults' health problems such as frailty and disability. Frailty is a condition in which the overall ability to maintain daily life independently is reduced due to functional decline in cognitive, psychological and social domains as well as the physical domain in older adults [1]. Frailty causes problems in medical, functional, social, and psychological areas, and problems arising from frailty again become factors exacerbating frailty. The assessment of frailty levels of older adults aged 60 or over in Korea according to physical frailty criteria proposed by Fried et al. [2] revealed that 11.40% of older adults aged 60 or over were frail and 46.04% were pre-frail, showing that 58% of all the older adults were shown to need frailty prevention and management [2]. Since frailty is closely associated with disability, institutionalization, and mortality [3], frailty prevention is taking on increasingly greater importance.
Because frailty is caused and exacerbated by various factors which affect each other, multifactorial interventions are more effective than single-component interventions to prevent frailty. So far, various frailty prevention programs for older adults have been developed and evaluated in foreign and domestic studies. However, in Korea, single-component program such as exercise, cognitive training, psychosocial activities has been provided to prevent frailty for older adults [45]. Even when some interventions are structured to provide a combination of multiple components, multifactorial programs are provided to older adults focused on education or lectures [67], so these interventions have limitations. The most common single-component program offered to the participants is exercise [38910]. Previous studies reported that exercise programs resulted in positive improvement in physical function such as grip strength and complex movement ability [38910]. They were also effective for depression reduction [7] and frailty prevention [89]. A 12-week intervention including cognitive training and group therapy activities was reported to be effective for improvement of cognitive function [11]. Cognitive training was found to be effective for improvement of gait and balance as well as cognitive function [12]. It was reported that participation in psychosocial activities decreased the level of depression in older adults [5]. In Korea, there have been few studies to evaluate the effects of multifactorial interventions, but some foreign studies have reported that multifactorial interventions comprised of multiple components such as exercise, cognitive training, psychosocial program, and nutrition were effective in preventing frailty [1314]. Therefore, it is needed to develop a multifactorial intervention including muscle strengthening exercise, cognitive training, and group therapy activities and to evaluate its effects.
Most studies on community-based programs provided short-term programs and evaluated their effects. In a previous study, after muscle strengthening exercise for older adults was provided twice a week for 12 weeks, it was found that although physical function was improved immediately after the program, functional levels returned to the baseline levels at 24-week and 36-week [10]. It was suggesting that intervention effects did not last long [10]. In fact, it is difficult for older adults living in urban-rural complex areas to continuously participate in a program because of seasonal and farming activities. In addition, public health centers and other welfare agencies operate temporary programs to provide programs throughout the community. Thus, there are many constraints on older adults' continuous participation in a program to prevent frailty.
According to the definition of the World Health Organization, capacity building is the development of knowledge, skills, commitment, structures, systems and leadership to enable effective health promotion [14]. In other words, capacity building is said to mean strengthening capacity at three levels: enhancement of knowledge and skills among practitioners, expansion of support and infrastructure for health promotion in organizations, and formation of partnerships and development of cohesiveness for health in communities [14]. Although it is emphasized that capacity building is important for health promotion, only a small number of previous studies used capacity building in actual interventions. Wurzer et al. [16] reported that the attendance rate of participants who were induced to participate in a long-term yoga program by peer leaders was higher than in other programs and fewer falls occurred among those participants. In addition, Waters et al. [17] reported that a muscle strength and balance enhancement program for older adults operated by a peer leader had a better effect on improvement of physical function than a seated exercise program and led the participants to continue to practice exercises through other programs even after 12 months. However, Ubert et al. [15] reported that a systematic review of the studies which applied capacity building strategies for older adults revealed inconsistent results regarding the effects of exercise interventions. In short, there have been few studies on application of capacity building strategies in Korea, and prior studies reported inconsistent results about the effects of application of capacity building strategies. Therefore, this study aimed to investigate the effect of a multifactorial program on older adults' heath status in urban-rural complex areas by conducting a follow-up program applying capacity building strategies of health leader training, partnership formation and organizing.
The specific objectives of this study are as follows:
To examine the effects of a multifactorial program for frailty prevention on the physical, cognitive, psychological functions and self-rated health in older adults;
To compare the degrees of changes in functional levels and self-rated health in older adults between the follow-up group provided with a follow-up program applying capacity building strategies and the non-follow up group after the end of the program.
METHODS
1. Study design
This study was a quasi-experimental study with nonequivalent control group pretest-posttest design to implement a multifactorial program for frailty prevention and a follow-up program for older adults using senior centers in K city, an urban-rural complex area, and to investigate the effects of the intervention on physical, cognitive, psychological functions, and self-rated health in older adults.
After applying the multifactorial program to both the follow-up and non-follow-up groups for 3 months, we made a comparison of changes in functional levels and self-rated health measured before application of the multifactorial program (pre-intervention) and after the end of the program (post-intervention 1). Then, we also made a comparison of changes in functional levels and self-rated health of older adults between the experimental group which participated in the 3-month follow-up program after the end of the multifactorial program (the follow-up group) and the control group without the follow-up program (the non-follow-up group) after the intervention program (post-intervention 1) and after the period of the follow-up program (post-intervention 2).
2. Participants
The participants of this study were older adults using senior centers located in K City, and they were selected according to the following criteria.
In this study, primary end points were set as the improvement of physical function and maintenance of cognitive function, and secondary end points were set as the improvement of psychological function and self-rated health. The effect size of this study was determined based on the effect sizes in similar studies [1213]. A randomized experimental study of a 6-month multifactorial intervention including resistance exercise, nutrition, and psychosocial intervention reported that the score of the Timed Up and Go (TUG) test was decreased by 0.25 seconds and the score for depression was decreased by 0.92 points. In addition, it has been reported that when a multifactorial program including exercise, nutritional supplements, and cognitive training was provided for older people for six months, muscular strength of knee joint increased by 2.65 kg and 6-m walking speed became 0.16 seconds faster compared with the control group [12]. Although the intervention group was compared with the non-intervention group in the two studies described above, in the present study, interventions were provided to both the experimental group and the control group. So, considering the comparison of intervention effects in terms of the presence and absence of the follow-up program, the medium effect size of 0.5 was assumed. In this study, using G*Power 3.1.9.2, the sample size was calculated through the comparison of the averages of two groups (t-test) by assuming follows: the medium effect size of .05, significance level of 0.05, power of 80%, and an allocation ratio of 1:1 for the follow-up and non-follow-up groups. As a result, 64 participants were required in each group. Assuming a dropout rate of about 25% during the 6-month intervention period, at least 80 people need to be enrolled in each group. A total of 16 senior centers participated in the program and the program was implemented from January 2017 to September 20, 2017. 16 senior centers which participated in this study were allowed to make a decision on whether to participate in the follow-up program voluntarily, and 9 senior centers chose to participate in the follow-up program but 7 senior centers did not. A total of 170 older adults (90 persons in the follow-up group and 80 persons in the non-follow-up group) participated in the study. However, excluding 27 persons (15 persons in the follow-up group and 12 persons in the non-follow-up group) who participated in neither of the two post-intervention assessments, a total of 143 persons (75 persons in the follow-up group and 68 persons in the non-follow-up group) were included in the final analysis.
3. Multifactorial Program
The multifactorial program of this study consisted of exercise, cognitive training, and group therapy activities. The program was performed once a week for 2 hours per session, was composed of cognitive training (workbook) (30 minutes), muscle strengthening exercise (30 minutes), and group therapy activities (40 minutes). The program consisted of a total of 12 sessions (Table 1). The follow-up program consisted of cognitive training (workbook, 30 minutes) and muscle strengthening exercise (30 minutes). The workbooks needed for cognitive training were provided by the public health center and the follow-up program was voluntarily performed with health leaders.
The multifactorial program for older adults was provided at senior centers. After educating participants about cognitive training (workbook) and exercise which they could practice at home for themselves each week, it was checked each week by phone whether the program was continuously performed at home.
The same multifactorial program was provided for both the follow-up group to which capacity building strategies were applied and the non-follow-up group for 12 weeks. The overall operation of the multifactorial program provided to the two groups was carried out by nurses and the continuous operation of the program was checked by phone. Cognitive training and group therapy activities were provided by occupational therapists and nurses, and muscle strengthening exercise was provided by exercise instructors.
For following 12 weeks, the follow-up group was allowed to flexibly adjust the schedule and operation methods of the program according to the situation of the target group by applying three capacity building strategies: 1) formation of partnership between the group and a healthcare agency, 2) organizing, and 3) training health leaders.
Firstly, we recruited the groups of older adults (senior centers) who wanted to participate in the multifactorial program and allowed them to decide whether to apply capacity building strategies. In the group of older adults to which capacity building strategies would be applied, a representative and a health leader were selected and the operation period and methods of the program were determined by collecting opinions through meetings. Through regular meetings (once a month), a partnership between a public health center and the group of older adults was formed. The health leader was directly responsible for operation of cognitive training and muscle strengthening training programs with volunteers for an hour. Withe regard to the operation of the follow-up program, the public health center provided necessary supplies, and nurses and exercise instructors offered guidance to the selected health leader. The health leader took responsibility for the operation of the 12-week follow-up program and nurses monitored the progress of the program.
1) Cognitive training
Cognitive training, which is one of the cognitive interventions proposed by Clare et al. [18], is focused on attention, executive function, cognition, language, and memory, and it is intended to improve, maintain and restore cognitive function by repeatedly performing specific tasks. This cognitive training helps to maintain the cognitive ability of participants by leading them to learn and apply new strategies. In this study, cognitive training was conducted using the workbook titled “Going Together” (spring, summer, autumn, and winter) developed by the Elderly Information Center. The cognitive training in this study included small muscle exercise using finger muscles through various activities, such as tearing and attaching colored paper, coloring work, arithmetic calculation suitable for the level of each participant, word chain, finding wrong pictures, finding hidden pictures, finding a path in a maze, as well as training to improve orientation, concentration, memory, problem solving ability, and executive function through activities such as sharing stories while recalling things about nature related to a season or recalling the past with a theme related to food or events and creating works using various materials. In addition, participants were required to complete the assignments presented among the contents of the workbook and it was checked by phone every week whether the participants completed their assignments.
2) Muscle strengthening exercise
Muscle strengthening exercise consisted of arm exercise using stretching and an elastic band, side exercise, and leg exercise for both legs. Each type of exercise was performed three times. This exercise was performed at the program introduction and finishing stages of each session and conducted for 30 minutes once a week. Posters containing exercise methods were provided to the participants so that they could perform exercise at home 10 times each day. It was checked by phone each week whether participants practiced exercise.
3) Group therapy activities
In a group of older adults, group therapy activities can be used to provide organized rules, promote the sense of stability and adjustment ability, and facilitate pleasant interaction through pleasure and appropriate arousal [5]. In addition, it is stated that through comfortable activities, individuals are accepted as valuable persons who deserve respect, and their abilities can be confirmed through experience of exploration and achievement [5]. In this study, group therapy activities included not only physical activities but also the time for static interaction activities such as self-introduction and sharing hobbies. Each session took a total of 40 minutes. The group therapy activities included various activities, such as a mini-athletic meet, team game of rock paper scissors, foot soccer (beach ball game using feet), napkin art, bowling, category classification, moving table tennis balls, ripping newspaper with feet, balloon volley, guessing food flavors, creating pottery, balloon popping using feet, ‘ojaemi (a small ball-like thing made of cloth)’ throwing, curling and darts.
4. Measures
In order to evaluate the effects of this study, general characteristics and health characteristics, physical, cognitive, and psychological functions and self-rated health were measured.
1) General characteristics and health characteristics
General characteristics, such as gender, age, ability to read and understand Korean, co-residing family, marital status, status of living alone, subjective economic level, and medical expenditure burden were directly investigated through a questionnaire survey. Regarding health characteristics, disease status, medication status, and experience of falling over the past year were examined. In addition, systolic blood pressure, diastolic blood pressure, fasting blood glucose level, height and weight, and waist circumference were measured directly.
2) Physical function
Physical function was measured using energy expenditure (kcal), grip strength (kg), standing on one leg with eyes open, and Timed Up & Go (TUG).
Energy expenditure (kcal) by intensity of physical activity was estimated using metabolic equivalents (1 MET=kcal kg-1 h-1). The intensity of physical activity was calculated according to the type of physical activity, and the total energy expenditure (kcal) was calculated as the product of intensity of physical activity (Mets) × frequency of physical activity × duration of physical activity × 1/60 × body weight (kg) [19].
Grip strength is an effective way to assess the overall strength, nutritional status, and muscle mass of the current state. Grip strength was measured in kilograms using a dynamometer. Participants were asked to hold a dynamometer firmly while holding the arm apart from the body at an angle of 15 degrees and standing with two feet apart naturally. Grip strength was measured by reading the value indicated by the needle. In the present study, the representative value of grip strength was defined as the higher value of the two measures after measuring the grip strength of the dominant hand twice [20]. Standing on one leg with eyes open is a variable to measure static balance. Participants were asked to stand on one leg using the leg they usually use more frequently and lift the other leg about 5 cm from the floor, and the time from starting the position to the moment when the lifted leg touched the floor was measured in seconds using a stopwatch. The TUG test is a useful variable to assess dynamic balance (gait ability). This test was conducted by setting the measurement distance as a 6m round trip by walking to and from a point 3m away from the starting position, and the time taken to get up from a chair, walk 3 m, turn around the target point, return to the chair, and sit back down was measured. This test was shown to have high test-retest reliability in a previous study of frail older adults, and it was verified that it has a high level of validity as a tool to assess the function of mobility [21].
3) Cognitive function
Cognitive function was assessed by a screening instrument for dementia (MMSE-DS) standardized by Kim et al. [22]. The validity and reliability of this instrument were evaluated by Kim et al. [22]. This instrument consists of 19 items to assess time orientation, place orientation, memory registration and recall, attention and concentration, order execution, figure copying, reading and writing, and judgment. The scores were classified into normal and cognitive decline according to the criteria of cognitive decline by gender, age and educational level. Regarding test-retest reliability, Cronbach's α was .83 at the time of development of the instrument [22], and Cronbach's α was .69 in this study.
4) Psychological function
Depression was assessed using the Geriatric Depression Scale (GDS), which was developed by Kee [23] to measure depression objectively. The instrument consists of a total of 15 dichotomous items. The scores range from 0 to 15 points and higher scores indicate higher levels of depression. 0 to 4 points were classified as normal, 5 to 9 points as mild depression, and 10 or more points as severe depression. Cronbach's α was .88 when this instrument was developed [25], and Cronbach's α was .87 in this study.
5. Ethical Considerations for Data Collection and Research
This study was conducted after obtaining the approval of the IRB of the university which the researchers belong to (IRB No.: 1044396-201604-HR-025-02). The principal investigator is currently entrusted with management of the Health Promotion Center of the public health center, and received the approval for this study from the health promotion department of the public health center in K si. We informed senior centers about the study and recruited senior centers which wanted to participate. We explained the study purpose and methods to older adults using senior centers and informed them that confidentiality and anonymity of the data would be guaranteed and they were free to withdraw from the study at any time. We obtained informed consent from people who agreed to participate in the study, and data collection was conducted three times with the participants. Nurses and exercise instructors directly collected data through interviews with participants using a questionnaire. Blood pressure, blood glucose level, height, weight, and physical function were directly measured. Intervention programs were provided for both the follow-up group and the non-follow-up group for 3 months. After the end of the 3-month intervention program, the participants in the follow-up group, which was the experimental group, were provided with a workbook for strengthening cognitive function needed during the follow-up program and the participants in the follow-up group were instructed to perform a cognitive training program and muscle strengthening exercise continuously. But the follow-up program was not provided for the non-follow-up group, the control group. Assessments were made before and after the intervention and at the end of the follow-up program.
6. Data Analysis
Data were analyzed using the SPSS 23.0 program. The general characteristics and health characteristics of the participants were analyzed using frequency, percentage, mean and standard deviation. The test of homogeneity for the general characteristics and health characteristics of the follow-up and non-follow-up groups was performed using χ2 test and t-test. The differences in physical, cognitive, and psychological functions and self-rated health were analyzed by t-test.
RESULTS
1. Comparison of General Characteristics and Health Characteristics between the Follow-up and Non-follow-up Groups
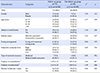
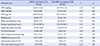
The results of the comparison of pre-intervention scores for general characteristics and health characteristics between the follow-up group and the non-follow-up group are shown in Tables 2, 3. There were no significant differences between the two groups in gender, age, ability to read and understand Korean, marital status, living alone, subjective economic level, medical expenditure burden, the number of diseases, and fall experience over the past year (p<.05). In addition, there were no significant differences in systolic blood pressure, diastolic blood pressure, waist circumference, energy expenditure, standing on one leg with eyes open, grip strength, TUG, cognitive function, depression, and self-rated health (p<.05). However, there were significant differences in the number of medications taken, fasting blood glucose level and BMI between the two groups. The number of medications taken by older adults was 1.61±1.20 in the follow-up group and 2.00±1.12 in the non-follow-up group. The mean fasting blood glucose level was 149.05±46.41 mg/dL in the follow-up group and 168.75±11.26 mg/dL in the non-follow-up group. The mean BMI was 24.00±2.97 kg/m2 in the follow-up group and 25.34±3.38 kg/m2 in the non-follow-up group. In short, the number of medications taken, the fasting blood sugar level, and BMI were higher in the non-follow-up group than in the follow-up group.
2. Comparison of Health Status before and after the Multfactorial Program and before and after the Follow-up Program
1) Evaluation of the effects of the multifactorial program
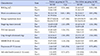
Table 4 shows the changes in health status before and after the 12-week multifactorial program in the follow-up group and the non-follow-up group. In the follow-up group, there were significant changes in waist circumference (t=3.68, p<.001), standing on one leg with eyes open (t=−2.11, p=.039), grip strength (t=−3.06, p=.003), and depression (t=2.60, p=.014). In the non-follow-up group, there was a significant improvement in TUG (t=2.43, p=.016) and grip strength (t=−2.40, p=.045) after the multifactorial program was provided. Although the differences between pre-intervention and post-intervention scores were not statistically significant, there were positive changes in cognitive function, self-rated health, and waist circumference in both groups.
2) Comparison of health status after the follow-up program between the follow-up and non-follow-up groups
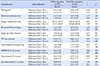
Table 5 shows the changes in the health status between pre-intervention and post-intervention scores and changes in health status between the scores after the intervention and after the follow-up program. The comparison between pre- and post-intervention scores of health status showed that there was no significant difference in BMI, waist circumference, energy expenditure, standing on one leg with eyes open, TUG, grip strength, cognitive function, depression, and self-rated health between the follow-up and non-follow-up groups. On the other hand, the comparison between health status scores after the intervention and after the follow-up program showed that while there was no statistically significant difference between the two groups in BMI, waist circumference, standing on one leg with eyes open, grip strength, cognitive function, depression, and self-rated health (p>.05), there were statistically significant differences in energy expenditure (t=2.00, p=.047) and TUG (t=−5.10, p<.001) between the two groups.
DISCUSSION
After the provision of a multifactorial program, the comparison of differences between two groups in physical function, cognitive function, depression, and self-rated health showed that although there were some differences between the follow-up and non-follow-up groups, there were positive changes in physical function and the decreased depression level in both groups. As a result of comparing the differences in health status according to the provision of the follow-up program after the end of the intervention program, it was found that energy expenditure and TUG were significantly improved in the follow-up group compared with the non-follow-up group.
First of all, the results of this study showed that the multifactorial program composed of muscle strengthening exercise, cognitive training, and group therapy activities as a psychosocial program had a positive effect on physical and psychological functions. These findings of this study are similar to those of previous studies which reported that frailty is a health condition into which not only physical but also mental and social domains are integrated and that a program including the multifactorial attributes of frailty contributes to frailty prevention by acting on physical, cognitive, and psychological functions in a combined way [4111213]. It has been previously reported that a threemonth multifactorial program consisting of resistance exercise, nutrition and a psychosocial program for frail and pre-frail older people living in Japan resulted in an improvement in TUG, the depression score and nutrient intake, showing positive impacts on frailty prevention. In addition, in Korea, muscle strength exercise for older adults provided for 8 weeks was reported to have positive effects on not only grip strength and TUG in physical function but also depression reduction [4]. In Italy, cognitive training offered to pre-frail older people resulted in not only improved cognitive function but also improved gait and balance ability through the improvement in spatial perception operation memory and processing speed and reduction of disability factors. Furthermore, in the UK, a multifactorial program including exercise, nutritional supplements, and cognitive training were provided to healthy and pre-frail older people for three months, and as a result, it was shown to have positive effects on energy expenditure and muscle strength improvement and have greater frailty prevention effects compared single-factor interventions of exercise, nutritional supplements, and cognitive training [12]. In addition, in the present study, no significant changes in cognitive function were observed. This result is in agreement with a previous study which reported that a multifactorial program including cognitive training did not lead to any significant improvement in cognitive function [12]. The findings of this study suggest that the multifactorial program provided in this study has a complex effect on various functions and can be used as a program which can prevent frailty by improving physical and psychological functions.
The results of this study showed that after the follow-up program applying capacity building strategies such as health leader training, participation in decision-making about operation methods, and formation of partnership with public health center was implemented for 12 weeks, the follow-up group showed a significant improvement in energy expenditure and TUG compared to the non-follow-up group. In other words, spontaneous continuation of practice of cognitive training and muscle strengthening exercise for 12 weeks even after the end of the 12-week intervention program resulted in a continuous increase in the exercise practice amount and improvement in TUG compared with the non-follow-up group. Prior studies reporting that application of capacity building strategies to an exercise program increased the tendency to spontaneously participate in and continue exercise even after the completion of interventions [1617] support the results of this study. In addition, the findings of this study are also corroborated by a previous study which reported that physical function improved after the end of the program returned to pre-intervention (baseline) levels after 6 months [10]. In addition, improvement in energy expenditure and TUG as a result of participation in a multifactorial program for 6 or more months means that the multifactorial program contributed to the positive improvement in two items among five frailty assessment criteria of Fried et al. [2], which are unintentional weight loss, low grip strengh, exhaustion (depression), slow walking speed, and low level of physical activity. These result implied that multifactorial programs can be effective in preventing frailty. Therefore, considering the limits of community resources, application of multifactorial programs to older people and the use of capacity-building strategies to induce older people to perform health promotion activities continuously through spontaneous follow-up are expected to contribute positively to frailty prevention in older people.
After the multifactorial program intervention, there were insignificant changes in cognitive function in the non-follow-up group. In the follow-up group, there were positive changes in cognitive function scores even after the follow-up program just as there were differences between pre-intervention and post-intervention scores. However, neither the comparison between pre-intervention and postintervention scores nor the comparison between the non-follow-up and follow-up groups showed any statistically significant changes in cognitive function scores. In this regard, even in previous studies, unlike physical function, cognitive function was not significantly improved after a multifactorial program was performed [12]. In addition, there was also no significant reduction in cognitive function even after the end of a multifactorial program [24]. In previous studies, it was reported that intervention effects were sustained for up to 6 months after cognitive skill training was applied to older adults [25]. Those group provided with cognitive training showed improvement in instrumental activities of daily living compared to the control group in a 5-year follow-up study [25]. Therefore, it is thought that the effects of cognitive training become apparent gradually and last relatively long. The maintenance of the cognitive function improved by the multifactorial program intervention in the non-follow-up group despite discontinuation of cognitive training could be interpreted as a result of the sustained effect of cognitive training. However, considering the results of previous studies that cognitive training contributes to the improvement of gait and balance as well as the improvement of cognitive function [11], it is likely that cognitive training performed continuously for 6 months in this study contributed partially to the improvement of physical function. Thus, it is necessary to reconfirm the results of this study through a longterm follow-up study on the time and duration of cognitive function improvement after cognitive training.
Grip strength, depression, and self-rated health, which were improved after a multifactorial intervention program, showed the tendency to deteriorate in the non-follow up group after the end of the intervention although the changes were not statistically significant. Although it is difficult to make a direct comparison since there are few studies on the residucal effect of the program, positive effects observed in the multifactorial program appear to decrease after the end of the program. The self-rated health of older people is highly related to the functional level and health-promoting behavior [26]. Therefore, it is possible that these results may be due to slightly reduced functional levels and a decrease in health promoting behaviors after the end of the intervention [26]. Even though exercise, cognitive training, and psychosocial programs are all programs which have positive effects on psychological function [713], the effects on psychological function were not maintained after the end of the intervention in this study. However, considering the results of previous studies that exercise contributed positively to psychological function as well as physical function [7]. it is thought that the level of depression in the follow-up group was continuously improved due to the practice of muscle strengthening exercise. Taken together, all these results suggest that it is necessary to continuously provide interventions for depression prevention through exercise or group activities to reduce depression in communities.
According to the Ottawa Charter of the World Health Organization, health promotion is a process which enables people to increase control over and improve their health [14]. Capacity building is highly related to health promotion [14]. Lalonte et al. [27] noted that health promotion is a means of community capacity building and that community capacity building is also a result of health promotion and enables people to maintain the effects of intervention programs actively. In other words, in this study, capacity building strategies applied to older adults gave senior center-based older adults the power of control to manage their health, and continuous practice of cognitive training and muscle strengthening exercise led to positive changes including improvement of physical function. There are many constraints on continuously providing an intervention for older adults in the community. Therefore, it is expected that there will be positive effects of maintenance of cognitive function as well as improvement of physical function if a multifactorial program to which capacity building strategies are applied is provided and continuous practice is encouraged on older adults using senior centers.
This study has some limitations. First, in this study, randomization was not conducted. So, there is a possibility that there were differences in organizational culture between senior centers which chose to receive the follow-up program and those which did not before the intervention was performed. In addition, selection bias cannot be excluded because there is a possibility that senior centers which chose to participate in the follow-up program had been active in frailty prevention activities. Second, caution is needed in interpreting the results of this study for the following reasons. Since the effects of individual studies of single-component interventions could not be compared with those of multifactorial programs, it is not possible to determine whether combined effects were produced. In addition, there is a possibility that the actual effects of the follow-up program were underestimated due to the residual effects of the intervention in the comparison of the effects between the follow-up and non-follow-up groups. Therefore, it is necessary to select the control group with rigorous experimental research design and reevaluate capacity building effects in older adults. Nevertheless, this study has significance in that the findings of this study demonstrated that an intervention applying capacity-building strategies for older adults and applying the follow-up program had the positive effect of the improvement of physical function. The results of this study are expected to serve as a basis for applying capacity building strategies to effectively operate community-based programs for older adults in the future.
CONCLUSION
The results of this study showed that a multifactorial program is an effective program to maintain and promote physical, cognitive, and psychological functions, and that the physical function of older adults can be continuously improved by inducing the participants to continuously do exercise and cognitive training activities using capacity building strategies. Based on the study results, the following implications for future research and practice are proposed. First, it is effective for frailty prevention to provide a multifactorial program consisting of muscle strengthening exercise, cognitive training, and group therapy activities, and if a multifactorial intervention program is continuously offered, it is expected to positively contribute to frailty prevention of older adults. Second, there are many difficulties in continuously providing a program for older adults because of the limits of community resources. Therefore, in order to prevent frailty, it is necessary to provide support so that older adults can perform health promoting behaviors continuously through capacity building of older adult groups. More specifically, we suggest that we should provide the support for the distribution of multifactorial programs for older adult groups using senior centers or senior welfare centers, training older adult leaders, formation of partnership with healthcare agencies, and inducing organizing and participation. Lastly, this study compared the effects of the 12-week follow-up program with those of the control group. However, this study was a quasi-experimental research in which randomization was not conducted and thus a rigorous experimental study is required to reevaluate the effects of a multifactorial program and a follow-up program. In addition, it is expected that there are differences according to attributes such as physical, cognitive, and psychological functions in residual effects and the effect duration period of interventions. Therefore, it is necessary to conduct repeated studies and long-term follow-up research on the duration of intervention effects after the completion of an intervention program.

 XML Download
XML Download