

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
1. Background
The number of older adults in South Korea has increased faster than in any other country worldwide. As Korean society ages, the requirements for aging services that meet the specific needs of older adults have increased [1]. The term, age-friendly, has been used to describe some of these initiatives.
An age-friendly city generally refers to a community in which older adults are valued, involved, and supported [2]. Developing age-friendly environments has recently been the focus of social policy in many countries and has also been a recognized and growing movement in South Korea [3]. In 2013, Seoul was designated as the first member of the Global Network of Age-friendly Cities and Communities (GNAFCC) among Asian countries. Other cities in South Korea, including Suwon and Busan, have become involved in the GNAFCC, created age-friendly guidelines tailored to their region, and developed action plans for creating age-friendly cities.
Si-Heung, one of the capital regions, became an aging society in 2013; specifically, the ratio of older adults increased to 7.6% in 2017 from 4.5% in 2003 [4]. Because of the proximity to a centrally-located and densely-populated metropolitan area, Si-Heung is expected to undergo increased aging due to the entry of aging baby boomers and an extremely low birth rate [5]. Thus far, Si-Heung has only conducted a primary survey and inspection regarding the present status of the city for the development of age-friendly guidelines; specific plans have not been formulated. Further, most of the basic investigation has stressed evaluation of the physical environment with respect to age-friendly attributes.
2. Community Support and Health Services, as a Feature of Age-friendliness
The World Health Organization (WHO) addressed eight key domains of age-friendliness, including three aspects of the physical environment (i.e., housing, outdoor space and buildings, and transportation) and five elements of the social environment (i.e., social participation, respect and social inclusion, civic participation and employment, communication and information, and community support and health services), followed by a checklist of the core features included in each part [6]. Among these domains, Community Support and Health Services (CSHS) were shown to be significant features that allow older adults to maintain health and independence in the community.
CSHS encompasses a wide range of initiatives that are designed to respond to the health needs of community members including district nursing, medical and social services, well-aging services, home care, residential facilities for people unable to live at home, a network of community services, volunteer support, and emergency planning and care [7]. The WHO recognizes the importance of CSHS to older adults by stating that an age-friendly city adapts its services to be inclusive of older adults with varying needs and capacities [6]. Besides, aging in place, in which older adults remain active and engage members of the community, depends on older adults having access to relevant service needs in the community [8].
Despite the importance of such services, most of the research and practice in South Korea has emphasized various aspects of urbanization and the physical space of the buildings [3]. While some international studies have addressed age-friendly city features from the perspective of older adults, which underscores CSHS [910], no research has been conducted with a focus on CSHS in South Korea. Moreover, although a few domestic studies have been conducted which have reported older adults' perceptions of the age-friendliness of cities [711], they did not specifically concentrate on older adults' perceptions of CSHS.
3. The Purpose of the Study
The WHO has emphasized that older adults should be engaged in the planning of age-friendly initiatives from inception [12]. Thus, guided by an age-friendly cities checklist, the current study focused on evaluating an index of CSHS from the perspective of older adults residing in Si-Heung. We also comprehensively examined the important characteristics of the participants to better understand the study findings relative to specific demographics. The specific aims of this study are threefold:
To examine the differences between older adults' appraisal and the rated importance on four categories of CSHS (service accessibility, offer of services, voluntary support, and emergency care planning) (Aim 1)
To examine the differences in each category's importance rating with respect to sociodemographic and health characteristics (Aim 2)
To identify the factors related to the rated importance of CSHS (Aim 3)
METHODS
1. Design
This study adopted a descriptive, cross-sectional approach. A convenience sampling strategy was utilized to identify participants.
2. Participants
The inclusion criteria for a participant were: (a) ≥65 years of age and currently residing in Si-Heung; (b) ability to understand the purpose of the study and give informed consent; and (c) no severe vision or hearing impairment. The sample size was determined by a power analysis [13]. With an α level at .05, power of .80, and up to 12 variables, the estimated sample size needed with a medium effect size of 0.15 [14] is 127 to detect a significant regression. We distributed our survey to 231 participants. Forty-eight surveys were deleted due to missing or duplicate data. Further, 17 surveys from participants categorized as having “definite dementia” by the study measure were excluded to ensure that all participants could give informed consent and comply with study procedures, which resulted in a final sample of 166 participants who were deemed eligible for analysis.
3. Measures
1) CSHS criteria
The survey items were adapted from the Korean version of Global Age-friendly Cities: A guideline [6]. The guidelines are available in various languages in addition to the original English version and have been utilized in numerous studies [16]. With the help of expert evaluators, a WHO sub-committee has worked to identify indicators for measuring progress and sustainability of the guideline [11]. The 14 items on CSHS are divided into the following 4 subscale categories: service accessibility; offer of services; voluntary support; and emergency planning care. Service accessibility consists of eight items that emphasize the ease of access to health services and the quality, equity, and efficiency of healthcare resource allocation. Offer of services is comprised of four items regarding the availability of various specific forms of care for members in the community. Voluntary support consists of one item that describes health and social services (e.g., caregiver services, home-care services, and welfare services) that are encouraged and supported by volunteers of all ages in the community. Emergency care planning consists of one item that reflects the community's actions to take account of the needs of people in preparation for and response to emergency situations.
We asked participants to appraise the current performance and rate the importance for each item using an 11-point scale (0~10), which was constructed specifically for the present investigation based on the literature [15]. Each sub-score is an average of the item ratings in a specific category, and the total score is calculated by summing up the average value of individual subscales. Higher scores indicated better appraisal of current status (0=“consistently unsatisfactory” to 10=“consistently superior”) and a higher degree of importance (0=“not important at all” to 10=“extremely important”). The internal consistency of the overall scales and subscales were generally satisfactory: the Cronbach's α ranged between 0.84 and 0.90 for the appraisal scale, and 0.81 to 0.89 for the importance scale.
2) Sociodemographic characteristics
Sociodemographic characteristics included gender (male or female), age (in years; 65~74=“young-old”, 75~84=“old”, ≥85=“old-old”), education level (range: 0~16 years; 0=“no formal education”, <7=“elementary school”, 7~10=“middle school”, >10=“high school or more”), marital status (married/partnered or non-married/unpartnered), financial status (no financial problem or having financial problem), and social network type (diverse, friend, neighbor, family, and restricted) [16].
(1) Social network
The social network was categorized into five network structures suggested by the literature [16]. The diverse network is the most endowed, with a variety of sources of potential support. The friends network is similar to a diverse network, but the members reported having only minimal contact with neighbors. Older adults in the neighbor network report frequent contact with adult children and with neighbors, but not with friends. The members in the family network report having an average of five proximate children who lived nearby and very frequent contact with the children. The restricted network has the most limited extent of social relations. The older adult in the restricted network is most likely not to have a spouse, have the least contact with adult children, and almost no contact with friends or neighbors. In particular, in this study, the answer options on the diverse network and friends network were clumped together because <5% of participants answered “friends network.”
3) Health characteristics
Health characteristics included health indicators (frailty, functional disability, cognitive function, depression) which were identified as significant characteristics of community-dwelling older adults by researchers' previous study [17].
4) Frailty
Frailty was measured by the Korean Frailty Index (KFI) [18], an 8-item questionnaire. The KFI distinguishes between different frailty states, including robust (0~2), prefrail (3~4), and frail (≥5) based on the number of criteria present. The internal consistency as measured by Cronbach's α for the KFI was .65. In the current study, the Cronbach's α was .61,
5) Functional disability
Elderly function and disability were measured using the Korean Instrumental Activities of Daily Living scale (K-IADL) [19]. The K-IADL can be classified as impaired (score<30) or non-impaired (score=30). The activities were categorized into 10 domains (e.g., housework, preparing meals, taking medications, etc.). Possible scores range from 10~30; higher scores indicate a higher capability of instrumental daily living. The K-IADL has satisfactory reliability (Cronbach's α=.94) and validity.
6) Cognitive function
Cognitive function was measured with the Korean version of the Mini-mental State Examination (MMSE-K) [20]. The MMSE-K is designed to measure various cognitive domains, including temporal orientation, registration, recollection, concentration, calculation, language, understanding, and judgment. MMSE-K scores range from 0~30 and is divided into the following 3 categories: definitely normal (>24); definitely dementia (<21); and questionable dementia (between 21 and 24). Higher scores indicate a higher level of cognitive function. In this study, participants categorized as “definite dementia” were excluded from the analyses as explained above.
7) Depression
The Korean version of the Short Geriatric Depression Scale (SGDS) [21] was used as a screening test for depression. The 5-item in SGDS has a sensitivity of .97, specificity of .85, and kappa of .81 for predicting depression in a frail community-dwelling older population. A score ≥2 of the possible 5 was recommended as the cut-off point for diagnosing depression. In the current study, the Cronbach's α was .74.
4. Data Collection
The study was conducted from January 2017 to May 2017. Recruitment of eligible study participants were performed in cooperation with the Si-Heung Public Health Center, after the approval from the Institutional Review Board of * University (IRB FILE No.1704-001-004). The participants were recruited from the social welfare center, senior citizen center, and churches. A home visit was made if the researcher identified a need. Participants were informed that their participation is voluntary and were assured confidentiality. Information was collected from self-reported data via questionnaires. Research assistants, who were public health nurses and community health workers, assisted participants in filling out the questionnaire, thus ensuring that older adults understood the survey instruments and response options. Answers were regularly monitored by the first author to ensure safety and accuracy of the collected data. Respondents required approximately 30~40 minutes to complete the questionnaire.
5. Data Analysis
The participants' characteristics were described using descriptive statistics including percent, frequencies, means, and standard deviations. A paired sample t-test was conducted to test for differences between older adults' appraisal and the rated importance on four categories of CSHS. An independent t-test and one-way ANOVA (Welch's ANOVA was considered in case of heteroscedasticity) were used to examine the differences in each category's importance rating with respect to sociodemographic and health characteristics. Post hoc comparisons were conducted using a Scheffé test. A Games-Howell test was employed for the data with variances that were not equal.
Hierarchical multiple regression analysis using the enter method was conducted to explore the significant factors contributing to the rated importance of CSHS. For regression analysis, health indicators and sociodemographic characteristics were entered as a block of variables in two steps in the model. Health indicators were entered in the first step, as these have been proven to be important characteristics of community-dwelling older adults [17]. The increase in R2 was computed to ensure each set of variables entering the equation made a significant contribution to the model. The F-test of overall significance was used to measure the improvement in model fit when including covariates. Prior to the analysis, multicollinearity among predictors was verified by the variance inflation factor (VIF). The VIF values were 1.10~2.20 indicating that multicollinearity is not a concern. Continuous outcome variables were checked for normal distribution; the distributions of the outcome variables satisfied the criteria for normal distribution with the skewness and kurtosis of the distributions being between −1 and 1. All analyses were carried out using the SPSS, v.20 (SPSS Inc., Chicago, Illinois), and significances were determined at a two-tailed α of .05.
RESULTS
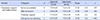
Table 1 shows the differences between older adults' appraisal and the rated importance on four categories of CSHS. The differences were only significant for emergency care planning among four categories (t=7.61, p<.001); emergency care planning was rated as most important (M=7.92, SD=1.90), while its current level of performance was appraised the lowest (M=6.97, SD=1.93).
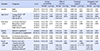
Table 2 and 3 details characteristics of the study participants and the differences in each category's importance rating according to their characteristics. Among 166 participants (22.9% male), an average age was 76.24 years with a range of 65 to 91. About 34.0% were categorized as young-old adults. The highest frequency belonged to elementary school group (42.2%), and approximately 36.0% of older adults claimed to have financial problems. Over one-half of participants were non-married or unpartnered, and 42.2% were classified in the restricted network. The ANOVA analysis showed that the scores on emergency care planning differed by age (W=8.01, p=.004); post hoc tests indicated that the average was significantly higher in old-old adults (M=8.61, SD=1.53) than that of old adults (M=7.98, SD=1.94) and young-old adults (M=7.20, SD=2.13). In addition, differences in scores on voluntary support were noted according to social network type (F=9.84, p<.001); those in restricted network (M=8.75, SD=1.64) rated their importance higher than those in a diverse/friends network (M=6.74, SD=2.01) and family network (M=8.10, SD=2.05).
In terms of health characteristics, the overall prevalence of robust, pre-frail, and frail participants were 51.8%, 33.1 %, and 15.1%, respectively. Of the participants, 25.3% had impaired functional disabilities. Besides, 51.2% were reported to have depression, and 25.1% were classified as questionable dementia. The ANOVA analysis demonstrated that the scores on offer of services differed with respect to functional disability (t=5.20, p=.011), as the average was significantly higher for the impaired group. Differences in scores for voluntary support were noted according to depression (t=2.48, p=.019), and the scores were higher for the people with depression. Further, there were differences in scores for emergency care planning with respect to frailty (W=4.77, p=.009); the scores were higher for the frail group than in the robust group.
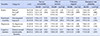
Table 4 shows the factors associated with the rated importance of CSHS criteria. Using the enter method described above, primary variable and established covariates were entered into the hierarchical multiple regression model. It was noted that depression (β=.29, p=.039) was a significant predictor influencing their rated importance in the null model (the model without adjusting covariates). Subsequently, after controlling for the covariates of sociodemographic characteristics, depression (β=.32, p=.016) again remain significant. Among sociodemographic characteristics, age (β=.37, p=.012) and being in restricted social network (β=.26, p=.039) had a strong association with the rated importance of the criteria. The χ2 value for all models were significant (p=.011; p=.003), supporting the validity of subsequent models and providing a better prediction than the null model.
DISCUSSION
Guided by the global age-friendly cities checklist, the current study evaluated an index of CSHS from the viewpoint of older adults residing in one city in South Korea. The differences between older adults' appraisal and the rated importance were only significant for emergency care planning among the four categories of CSHS. In addition, the difference in the rated importance of each category of CSHS was contingent upon the older adults' background characteristics. In particular, depression, older age, and restricted network type were significantly associated with placing a greater importance on CSHS.
Emergency care planning was rated as most important, while its current level of performance was lowly appraised, indicating a need to ensure appropriate emergency services for older adults. Successful emergency care tailored to older adults in terms of availability, continuity, and timely provision has been signified as a social imperative in many cities in Korea [22]. Si-Heung has not yet been included in these discussions, which warrants community-level efforts for effective emergency management for this population. Besides, such schemes are regarded as the most urgent issues, particularly for the vulnerable [22]. Indeed, frailer people and the elderly in the present study rated the importance of emergency services as significantly higher than their more robust and younger counterparts. This imparts that services should focus on older adults with frailty who may have compromised ability to respond to emergencies. Further, the much older group should be viewed as a unique risk-group rather than merely a part of the older population as the oldest of the old require different emergency plans and present different emergency utilization patterns [23].
Compared to older adults without functional disability, people with impaired functional ability scored high on the importance for offer of services. In addition, nearly over one-third of the participants were reported to have impaired IADL functions. These clearly emphasized an importance to assist older adults to live independently in their homes by providing an array of home care services, such as home nursing, house cleaning, home maintenance, shopping, transport, day care, social outings, and home visits [24]. Especially for continuity of primary care, continuous assessment by a visiting nurse service should be facilitated to screen individuals at risk of current and lifetime health issues [25].
People with depression or who live in a restricted social network were more likely to emphasize the importance of receiving health and social services from volunteers within the community. These findings stress the key roles of community-based volunteering services in serving the health and socialization needs of older adults. For instance, clinical support services by trained volunteers exerted a positive influence on psychological health among older adults [26]; socialization services with older adults support active social interactions and promote networks of reciprocal social relations [27]. Although no study on the given topic exists in Si-Heung, the number of volunteers or community volunteer organizations in Si-Heung is reportedly lower than in other cities in Gyeonggi province [28]. This supports that the city needs to foster active discussion on improving volunteer resources while simultaneously making it segmented to meet the needs of specific individuals and situations.
Regression analyses show that those with depression were more likely to rate the importance of CSHS as higher than those without depression. Throughout the literature, mental health services as part of community-based services have proven valuable in that they offer opportunities for the recognition and intervention in depression and associated needs among older adults [26]: in fact, a broad array of effective depression management systems such as primary care provision, assertive outreach services, and routine counseling have been introduced. However, there is no clear consensus on what treatments or services are beneficial to depressed older adults in Si-Heung. Given that nearly half of the current study's participants had depression, the findings call for a more critical examination and development of interventions that are available to older adults in need.
Besides, being older was a sociodemographic characteristic significantly related to a higher degree of importance of CSHS. The oldest group was known to have substantial health needs, demanding an increase of formal or informal services. Indeed, how well society is equipped to advocate and understand the needs of the elderly has long been an indicator of social injustice [29]. However, researchers may easily undervalue their health needs because the oldest group is reluctant to express them to avoid the stigma associated with being ill [13]. In this regard, although the present study collected a small sample of the oldest group, the results were meaningful as they provide evidence of the health needs for the oldest age groups.
Lastly, older adults being in restricted social networks expressed a greater importance of CSHS, underscoring the need for community services that target people with the most limited extent of social relations. These specifically highlight the concept of social connectedness, a key aspect of age-friendly communities, which signifies sustainable and meaningful connections to the community through social services [30]. Several services that promote active and continual engagement in the community for older adults have been identified throughout the literature [2]; these include social, recreational, and educational activities that involve the engagement of family, friends, and neighbors, or economically valuable activity such as senior employment programs, all of which are great suggestions for future practice in Si-Heung.
This study has several limitations. First, the participants were not randomly selected, and the findings may not be generalizable to the larger community. Therefore, these findings will need to be verified in geographically-diverse populations of older adults residing in Si-Heung. Second, the measurements were too inclusive without respecting diversity, which may have undermined engagement by older adults in community development. For example, from whom and from where the health services that older adults want to receive were missing from the WHO checklist. Thus, specifying and designing a checklist that is tailored to older adults and examining the best route by which to provide health services is warranted; this can ultimately determine what interventions will work best. Lastly, a pilot study might have been helpful to better validate the reliability of survey items and enable respondents to have a better understanding of the survey.
CONCLUSION
This study provided a preliminary analysis on the development of age-friendly cities by identifying key features of community support and health services will meet the preferences of older adults. Based on the findings, this paper concludes with the following implications.
First, the emergency system should be improved to effectively provide services to older adults while paying attention to the unique needs of the frail and elderly. Second, it is essential to provide practical services to groups with functional disabilities who need the most assistance and are the most dependent on others. Third, the mental health needs of older adults also need to be properly addressed with continuous health support services. Fourth, it is important to raise awareness of the special needs of the oldest people in the community. Lastly, improving social connectedness among older adults in restricted networks through socialization services is required to promote wellbeing and inclusion among older adults in communities. Overall, realizing these will require comprehensive and ongoing assessment before implementing action plans for an aging-friendly city such that plans can be designed to incorporate the multi-dimensional problems of older adults with the goal of generating tailored interventions.

 XML Download
XML Download