

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The mandibular division of the trigeminal nerve (cranial nerve V) is a mixed nerve containing somatic afferent and special visceral efferent fibers that run downward through the foramen ovale. The lingual nerve (LN) is one of the terminal branches of the mandibular division and supplies afferent fibers to the mucosa of the floor of the mouth, lingual gingiva of the mandible, and mucosa of the anterior two-thirds of the tongue [12]. In the pterygomandibular space, the LN receives the chorda tympani branch of the facial nerve (CN VII) posteriorly, runs along the LN, and innervates the sense of taste from the anterior two-thirds of the tongue. The LN has communicating branches (anterior, middle, and posterior parts of the tongue) with the hypoglossal nerve [3]. The LN passes through and under the attachment on the mandible of the superior pharyngeal constrictor and pterygomandibular raphe and travels close to the lingual plate and lingual crest near the lower third molar [4]. There are studies describing the relationship of the LN and the mandible in formalin fixed cadavers [56789]. Reliability of the measurements in the location of the LN in the fixed cadavers is doubtful as the position of the LN could change before and after tissue fixation. Interestingly, Iwanaga [10] demonstrated that the LN moved based on tongue position in fresh frozen cadavers. LN injury is one of the major complications of wisdom tooth extraction [11]. Therefore, an improved anatomical knowledge of the LN in the lower third molar area is critical to avoiding unnecessary complications for dentists and oral surgeons. Therefore, this study aims to observe the diameter of the LN at the level of the third lower molar using fresh frozen cadavers.
Go to : 
Materials and Methods
Twenty sides (right, 10; left, 10) from 10 fresh frozen adult cadaveric Caucasian heads were used for the present study. The specimens were derived from three males and seven females with age at death ranging from 57 to 93 years (average age, 71.5±12.7 years). The number of the dentulous and edentulous mandibles were both five. The mucosa of the oral floor at the level of the lower third molar was incised anteroposteriorly and the loose connective tissue was bluntly dissected to expose the LN. Then, the diameter of the LN at the level of the third lower molar was measured. The relationship between the LN, mucosa, and submandibular gland was noted. All dissection and measurements were performed by one oral surgeon. A microcaliper (Mitutoyo, Kanagawa, Japan) was used for all measurements. This study was not required to be approved by our ethical committee as this was a cadaveric study. No previous scar was observed in the floor of the oral cavity or tongue.
All quantitative measurements were documented as the mean±standard deviation. To compare data, one-way analysis of variance was used with Scheffé's post hoc test and Fisher exact test. Statistical significance was set at P<0.05.
Go to :
Results
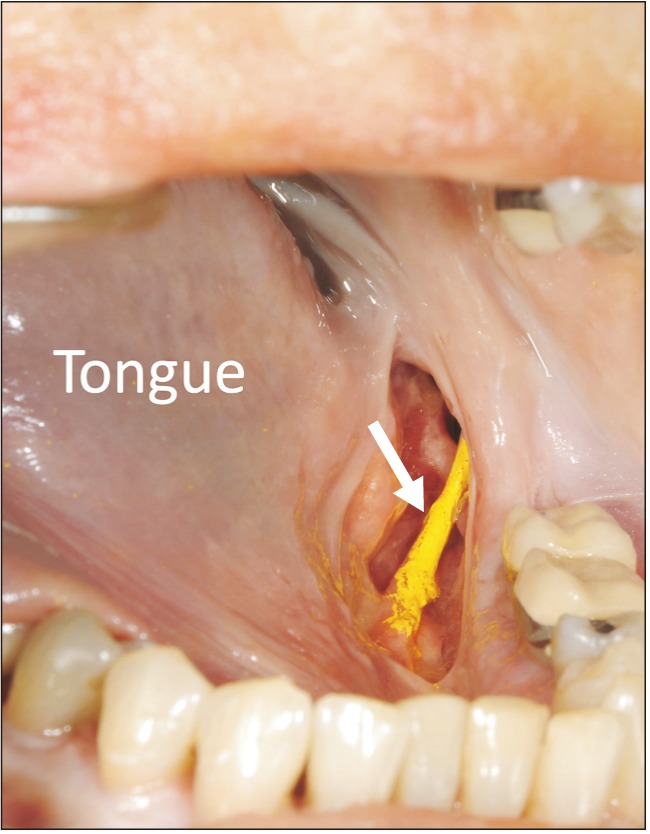
On all sides, the main trunk of the LN was identified at the level of the lower third molar just below the mucosa and above the submandibular gland (Fig. 1). The diameter of the LN ranged from 1.61 to 2.95 mm (mean, 2.20±0.37 mm). No statistically significant differences in the measurements were observed between males (n=3) and females (n=7) (P>0.05). The mean diameter of the LN was 2.18±0.34 mm (range, 1.62–2.60 mm) on right sides and 2.22±0.40 (range, 1.79–2.95 mm) on left sides. There was no statistically significant difference (P>0.05) between right and left sides. The mean diameters of the LN in the dentulous and edentulous mandibles were 2.17±0.43 mm (n=10; range, 1.62–2.95 mm) and 2.23±0.30 (n=10; range, 1.89–2.88 mm), and there was no statistically significant difference (P>0.05). There were no major anatomical variations of the LN during dissections.
Go to :
Discussion
The LN arises from the posterior division of the mandibular nerve under the foramen oval and into the infratemporal fossa [12]. It then travels under the mandibular attachment of the superior pharyngeal constrictor and pterygomandibular raphe and approaches the lower third molar. Kiesselbach and Chamberlain [5], in a study of 34 adult cadaveric heads, described that the LN contacted the lingual plate in 62% and existed at or above the alveolar crest in 17.6% at the region of the third lower molar. Miloro et al. [13], using high-resolution magnetic resonance imaging (HR-MRI), reported that the LN contacted the lingual plate in 25% and existed at or above the alveolar crest in 10% of patients at the region of the third lower molar. Behnia et al. [4], in 430 fresh cadaveric heads, also reported that the LN contacted the lingual plate in 22.3% of patients and existed above and below the lingual crest in 14.5% and 85.8% at the region of the third lower molar, respectively. There are several pieces of literature that described the diameter of the LN at the third lower molar [571314]. Kiesselbach and Chamberlain [5] showed that the diameter of the nerve was 1.86 mm in 34 adult cadaveric heads. Miloro et al. [13] studied using HR-MRI that the diameter was 2.54 mm (range, 1.58–3.13 mm) in 10 volunteers (mean age, 24.7 years; range, 21–35 mm). Hölzle and Wolff [14] reported that the diameter was 2.7±0.3 mm (range, 1.9–3.6) in 68 specimens (34 formalin-fixed cadaveric heads). Kim et al. [7] also clarified that the diameter was 3.3±0.6 mm (range, 2.2–4.4) in 32 specimens (hemi-sectioned formalin-fixed cadaveric heads). In our study, the diameter of the LN in the fresh frozen cadavers was 2.20±0.37 mm (range, 1.61–2.95). However, several authors reported that the mean diameter of the LN at the retromolar area was 3.62±1.0 mm (range, 2.5–4.5) [6], 2.3±0.4 mm (range, 1.5–3.5) [7], and 2.04±0.4 mm (range, 1.42–2.96) [8] in formalin-fixed cadavers. At the horizontal plane of needle placement, the mean diameter of the LN in formalin-fixed cadavers was 3.42±0.38 mm (range, 2.55–4.15) [15]. At the pterygomandibular space, the mean diameter of the LN was 2.57±0.44 mm in fresh frozen cadavers and 2.97±0.48 mm in formalin fixed cadavers [16]. There is a discrepancy in the mean diameter of the LN in the literature (Table 1). However, Hölzle and Wolff [14] concluded that the influence of formalin fixation on the shape of the LN was minimal by comparing its shape between formalin fixed and fresh cadavers. By contrast, Iwanaga et al. [16] reported that the mean diameter of the LN had a statistically significant difference between fresh-frozen and formalin-fixed cadavers. Despite some discrepancy between these studies, there is no doubt that the LN is a risk factor during oral surgery.
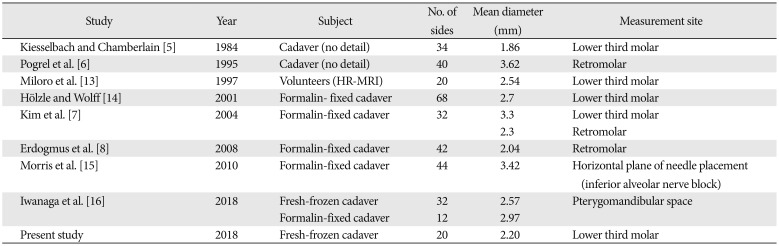
Table 1
The diameter of the lingual nerve in each measurement site
| Study | Year | Subject | No. of sides | Mean diameter (mm) | Measurement site |
|---|---|---|---|---|---|
| Kiesselbach and Chamberlain [5] | 1984 | Cadaver (no detail) | 34 | 1.86 | Lower third molar |
| Pogrel et al. [6] | 1995 | Cadaver (no detail) | 40 | 3.62 | Retromolar |
| Miloro et al. [13] | 1997 | Volunteers (HR-MRI) | 20 | 2.54 | Lower third molar |
| Hölzle and Wolff [14] | 2001 | Formalin-fixed cadaver | 68 | 2.7 | Lower third molar |
| Kim et al. [7] | 2004 | Formalin-fixed cadaver | 32 | 3.3 | Lower third molar |
| 2.3 | Retromolar | ||||
| Erdogmus et al. [8] | 2008 | Formalin-fixed cadaver | 42 | 2.04 | Retromolar |
| Morris et al. [15] | 2010 | Formalin-fixed cadaver | 44 | 3.42 | Horizontal plane of needle placement (inferior alveolar nerve block) |
| Iwanaga et al. [16] | 2018 | Fresh-frozen cadaver | 32 | 2.57 | Pterygomandibular space |
| Formalin-fixed cadaver | 12 | 2.97 | |||
| Present study | 2018 | Fresh-frozen cadaver | 20 | 2.20 | Lower third molar |
![]()
In conclusion, this study observed the detailed diameter of the LN using fresh frozen cadavers. A better anatomical understanding of the LN may help minimize LN injury, which is a severe complication of oral procedures.
Go to :
 XML Download
XML Download