

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
1. Background
Social intelligence is a concept beyond the empathy. It is the ability to accurately interpret the behavior of others in social situations, and absolutely necessary for social success [1]. Social intelligence can be linked to communication, management of resources, collaboration, teamwork, and leadership, which require communicating with people, resolving problems in interpersonal relationships effectively, and determining their own emotional ability [2]. Therefore, this concept should involve core competencies of nursing such as therapeutic communication skill [3], but social intelligence did not get much attention in nursing research.
Social intelligence reflects social understanding and interest as well as the ability to interpret social information, and leads to accurate social inferences [4]. According to the manipulative ability to understand and manage other people by perceiving one's own and others' internal states, a previous study reported emotional intelligence is recognized as a sub-concept of social intelligence among many disciplines [5]. While emotional intelligence is recognized as an important concept that nurses should have [6], it is suggested that the use of social intelligence, which is a more extended concept may be an effective concept in nursing practice.
Social intelligence can be improved by interventions, because it is cultivated rather than inherently innate and it is a psychological variable that can measure social behavior efficiently [7]. Thus, social intelligence scales have been developed for adolescents or general college students in other disciplines [158]. In Korea, the core competencies of nursing education include therapeutic communication and leadership, but it is also necessary to develop measurements that can quantify these concepts with objective scores and apply them to the education system [9]. Therefore the development of a social intelligence scale will be helpful for nursing research, practice and education.
Some researchers have developed scales to measure social intelligence. However, these scales have difficulties in the measurement method. First, the underlying construct of social intelligence was too abstract to understand. Second, many measurement methods were pointed out as a problem because they have several methods such as observation and behavioral assessment [810]. As the Tromsø Social Intelligence Scale (TSIS) was developed to correct these problems [11], the TSIS was translated into many languages and its psychometric properties were evaluated as acceptable [10121314]. The TSIS was used to examine the correlation with school adjustment and empathy in students [515]. It was also applied to the elderly, suggesting recently that social intelligence is a positive concept [16] that can be applied to various ages as well.
Although the TSIS was translated into Korean and its psychometric property was examined in college students of a nursing study [10], there is no further study recently done as a psychometric further study. In the recent research on social intelligence in nursing, an other social intelligence scale was applied after modification for adolescents [17]. Therefore, this study aimed to develop a Korean version of the TSIS for nursing students, which was developed by Silvera and the colleagues [11]. The TSIS improved the measurements of existing social intelligence scales, contained a self-report questionnaire format, and was developed for researchers to use easily. It was also developed to measure social cognition ability through behavioral factors. The purpose of this study was to examine the reliability and validity of a Korean version of the TSIS.
METHODS
1. Design
This study was a methodological study to examine the validity and reliability of the Korean version of the Tromsø Social Intelligence Scale.
2. Participants
Recruitment was conducted at three universities in three provinces of South Korea. The participants were nursing students who were enrolled in those universities. The participants were recruited through collaboration with the nursing departments, and were randomly selected students who agreed on the purpose and the procedure of the study without any plan to oversample male nursing students. The researchers distributed the questionnaires at the time appointed by the nursing departments and collected them immediately.
The construct validity was confirmed by applying exploratory factor analysis, in which the number of participants required is at least seven times per the number of items [18]. The original scale of the TSIS consists of 21 items. The appropriate sample size was considered as five to ten subjects per an item for scale development studies [19]. Given the 21 items, a total of 290 questionnaires were distributed and 21 samples were excluded due to incomplete qustionnaires (e.g., multiple answers for individual items). The final 269 valid questionnaires were included in the analysis.
3. Ethical Consideration
This study was approved by the affiliated university's Institutional Review Board (WKIRB-201511-SB-046). All participants received the notice that if they did not want to participate at any point during the study, they could withdraw from participation without any disadvantages. Each written informed consent was obtained from all the participants.
4. Measurement
1) Tromsø Social Intelligence Scale
The TSIS was developed by Silvera and colleagues [11] to measure social intelligence. We obtained permission to use the TSIS from the original developer, Dr. Silvera. This scale consists of 21 items and three sub-factors: (a) social information processing, (b) social skill, and (c) social awareness. Social information processing measures the ability to understand verbal or nonverbal messages regarding human relations, that is, both implicit and explicit messages. Social skill stresses the behavioral aspects of the construct by assessing the ability to enter into a new social situation. Social awareness measures the ability to behave in accordance with situation, place, and time. The Cronbach's α of the 21 items was .72 and .79 for social information processing, .85 for social skills, and .72 for social awareness in Silvera et al.'[11] study. In this study, the Cronbach's α was .81 for social information processing, .86 for social skills, and .79 for social awareness, respectively.
2) Global Interpersonal Communication Competence Scale (GICC)
To assess criterion-related validity, this study used a Korean version of the Global Interpersonal Communication Competence Scale (GICC-K), which was revised by Hur [20]; the GICC was developed by Rubin et al. [21]. GICC was developed to measure social competence, social performance skills, and empathic ability [20], which are variables related to social intelligence. Therefore, GICC was selected to confirm the criterion-related validity of the TSIS.
We obtained permission to use GICC from Hur. This scale had a total of 15 items using a 5-point Likert type, with scores thus ranging from 15 to 75 points. The higher score means the higher levels of communication competence. Cronbach's α was .80 in Hur's study [20] and .71 in this study.
5. Procedure
First, the scale was translated into Korean by an English professor who is fluent in both English and Korean. The preliminary Korean version was back-translated to English by native English speakers. The translators and three professors compared the back-translated version with the original. They discussed the cultural differences, grammar, and interpretation. Second, in order to assess the face validity, it was administered to a pilot group of two students per grade and a total of eight nursing students. They found difficulties in understanding statements and words in the Korean version of TSIS (TSIS-K) and any latent problems in translation and solved them. Finally, the final version of TSIS-K was completed and evaluated. The data collection period was from November 2016 to April 2017.
6. Data Collection and Analysis
Data were analyzed using IBM SPSS Statistics for Windows (IBM Corporation, Armonk, NY, USA). The procedure of the analyses was as follows: (1) the general characteristics of the participants were calculated as real numbers and percentages; (2) the validity of the TSIS-K was specified, using content, construct, and criterion-related validity; (3) internal consistency reliability was tested using Cronbach's α; (4) the construct validity of the scale was investigated by exploratory factor analysis (EFA); (5) to examine convergent and discriminant validity of items, multitrait-multimethod (MT-MM) matrix analysis was done; and (6) Pearson's correlation coefficients were used to examine criterion-related validity with GICC.
RESULTS
1. General Characteristics
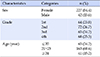
Surveys from 42 male students (15.6%) and 227 female students (84.4%) were analyzed. The grades were represented by 64 freshmen (23.8%), 72 sophomores (26.7%), 65 juniors (24.2%), and 68 seniors (25.3%). The mean age was 21.2 years. Further details about the general characteristics are presented in Table 1.
2. Content Validity
Content validity was assessed by experts' judgement based on the wording, grammar, and item allocation of the scale. After its translation and reverse translation, this scale was assessed by five nursing professors. To calculate the Content Validity Index (CVI), the five experts rated each item based on a 5-point Likert scale. Items' CVI scores larger than 0.79 were considered as appropriate [22]; this scale's CVI score was 0.87, hence none of the items needed to be modified in this study.
3. Construct Validity
The corrected inter-item correlations of the 21 items ranged from .17 to .50. Four items with Pearson's correlation coefficients was below .30 (items No. 4, 12, 16, and 18). Although the correlation coefficient of item No. 21 was over .30, if this item (No. 21) was deleted, Cronbach's α would increase to .77. Therefore, these five items were deleted. After the inter-item correlation coefficients were used to remove the five items, we did an exploratory factor analysis of the remaining 16 items to assess construct validity.
The value of the Kaiser-Meyer-Olkin (KMO) coefficient was .80, and the Bartlett's sphericity test chi-squared value was 1229.95 (p<.001). The obtained result indicates that the sample size was sufficient and adequate for factor analysis. Inspection of the eigenvalues suggested a 4-factor solution, with values of 4.24, 3.32, 1.65, and 1.02. However, the eigenvalue of the fourth factor was significantly less than the third-factor eigenvalue, and the score plot showed only three factors to be clearly on the slope. In addition, the 4-factor solution was uninterpretable. Therefore, using exploratory factor analysis, principal component analysis, and varimax rotation, we found out a 3-factor model in which all eigenvalues were higher than 1.0, with a total explained variance 61.3%. The factors accounted for 23.4%, 21.2%, and 16.7% of variance.
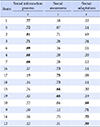
According to the observed factor loading and labels of the original TSIS, factor 1 was labelled as social information process (seven items), factor 2 was labelled as social awareness (five items), and factor 3 was labelled as social adaption (four items). Further details about the EFA analysis are presented in Table 2.
4. Convergent Validity and Discriminant Validity
The convergent validity and discriminant validity of this scale were analyzed by a multitrait-multimethod (MT-MM) matrix approach. As inter-items, each subscale correlation was greater than .40, scaling success rate of convertgent validity. Correlation of inter-items of different sub-factors was also greater than .40, scaling success rate of discriminant validity (Table 3).
DISCUSSION
This study investigated to develop a valid and reliable instrument of social intelligence. TSIS-K scale comprised 16 items with 3 sub-factors tested in nursing students. It has acceptable validity and reliability to measure social intelligence in Korean nursing students.
The multitrait-multimethod matrix analysis was constructed for the convergent and discriminant validity. In this study, the correlation coefficients between the sub-factor inter-items were at least .40 and the convergent validity of the item was established. The correlation between the sub-factor inter-items was .30 in Silvera et al.'s study [11], and was also at least .30 in Doğan and Çetin's study [12]. Inter-items of different sub-factors correlation were satisfied, thus the discriminant validity was established. Therefore, the convergent and discriminant validity achieved scaling success rates in this study [23]. A successful evaluation of the convergent validity means the scale was considered to be adequate in terms of distinguishing between the traits to be measured [1224]. In addition, establishing the validity of discrimination provide evidence that the measure is reflecting a conceptually distinct construct [25]. Thus, TSIS-K showed that all items continuously measure the concept of configuration and maintain independence between subscales.
After the EFA, 16 items remained among 21 items. Park [10] who targeted general college students in Korea, derived 19 items and two items were deleted. However, there was no deletion of the item in the study developed as Turkish and Italian versions of the study [1213]. In the Austrailia's study [14], one item (No. 20) was deleted to address low reliability. Despite removing five items from this study, the total explanatory power is 61.3 percent, which is higher than the 51% of the total explanatory power of the original instrument [11]. The three factors accounted for 23.4%, 21.2%, and 16.7% of variance, respectively. In addition, the previous studies reported three factors and explained the total variance from 40.6% to 44.8% lower than this study [10121314]. This means that the deletion of the items through various processes is stable to construct validity in this study. In general, the lower the number of items relates to the lower the reliability. However, the reliability of Cronbach's α .80 was stable after the items were deleted. Most of the previous studies showed that the Cronbach's α was .75 to .83 [1011121314], similar to or slightly lower than that in this study. Thus, the internal consistency of the scale was sound in this study.
In this study, five items were deleted. Without deleting the items, the first factor was similar to previous studies [10121314] without deleting the items. Two items were deleted from the second factor, the removed items were No. 16 (‘I often hurt others without realizing it’), and No. 21 (‘I am surprised by the reactions of others’). Social intelligence influences inter-cultural communication and is considered to be a function of a particular culture [8]. Because only nursing students were included in this study, it is necessary to replicating studies whether a unique culture is reflected or whether cultural differences between countries have affected the research when compared to other studies in which general college students or adolescents are subjects. In the third factor, three items were deleted. As in this study, Park's study [10] also removed item 4 (‘I often feel uncertain around new people who I don't know’) of this factor. Two more items were removed from the third factor: No 12 (‘I have a hard time getting along with other people’), and No. 18 (‘I'm good at getting along with new people’). However, there was no deletion of this factor in the Turkey and Italy studies [1213]. Social intelligence for the Chinese intends to create harmony and maintain equilibrium by conforming to other's expectations, whereas social intelligence for Germans intends to obtain one's goals and influence others [726]. Based on this, it can be seen that there is cultural differences between the Eastern and Western countries. Therefore, it is meaningful to work a comparative analysis of social intelligence of Eastern and Western societies in future research.
The first factor included seven items, which mainly were ones about understanding the emotions of others and predicting their behavior, thus the factor's name is the ‘social information process’ in the original version. Social information is the ability to understand the feelings, thoughts, and behaviors of others in a social context and to decipher the verbal or nonverbal passwords communicated as social information [2728]. Social intelligence reflects the ability to interpret social information [4], which is a representative characteristic of social intelligence. In a nursing field, it can be similar in meaning to a therapeutic communication, which is interpreted as a higher level of ability than empathy. In addition, it is regarded as a factor reflecting the ability to properly interpret the nonverbal message of the subject as well.
The second factor consists of five items for response to someone else's behavior, that means personal response to one's behavior. The negative reaction to recognize oneself according to social situation is similar to the ‘social awareness’ in the original scale. Awareness provides a context for understanding and interpreting one's own experiences, action, and social interactions [27]. Social intelligence includes a perceptual, cognitive-analytical feature that can control negative emotions and behaviors [16]. Therefore, it can be seen that this factor consists of items that fully reflect the content of social awareness. In nursing, emotional awareness plays an important role as a key component of self-awareness and self-motivation assumes an intervention to goals. Therefore, it should be assumed that this scale is suitable for nursing students.
The third factor was named social adaptation including questions such as “I am good at entering new situations and meeting people for the first time” and “I am easily adapted to social situations.” A person with high social intelligence responds to new situations realistically and solves interpersonal problems [7]. For this reason, the items of this factor reflect their behaviors for social adaptation. The original version centered on a social skill, but after the three items were removed, the rest of the items were determined to include higher social adaptation than social skill. Social intelligence is related to how people can effectively control their behavior [7], and social adaptation is one of the components of social intelligence [11]. In addition, it is adaptation to others and to the social situations [28]. Especially, social adaptation ability can be applied to evaluate the turnover rate of nurses and the clinical practice of nursing college students because it has an influence on the turnover rate of nurses and the clinical practice of nursing students. In the criterion validity, TSIS-K and GICC showed a high correlation of .68. This means that the correlation coefficients are between .60 and .80, which are interpreted as very valid [1819]. This scale can be considered to reflect the concept of social intelligence.
In particular, nursing students often meet unfamiliar persons during clinical practice. Because the subjects of this study were evenly distributed in similar numbers in all grades, the interpretation of the items is distributed across all grades in the results of this study. There may be differences in attitudes and anxiety about interpersonal relationships between juniors and seniors who participate in clinical practice, and freshmen and second graders who have not yet experienced hospital practice. Therefore, it is meaningful to conduct social intelligence surveys of each university year in future research. The study suggests that it will help to identify problems with social response methods and to understand the level of interpersonal and communication skills in terms of academic experience.
CONCLUSION
The study confirmed the validity and reliability of the TSIS-Korean version and showed that the results are suitable for the psychometric scale. The results of this study can be used as basic data for future social information research and can be used as an evaluation measure in nursing student intervention studies. Social intelligence is still an unfamiliar concept in nursing research, but it can be used as an indirect index to measure the social ability of nursing research as psychological variables.

 XML Download
XML Download