

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Giant-cell arteritis (GCA), also known as temporal arteritis, is an autoimmune vasculitis of moderate-sized and large blood vessels that is considered a medical emergency due to its potential to cause rapidly progressive irreversible blindness.12 The most common pattern of permanent vision loss due to GCA is arteritic anterior ischemic optic neuropathy (AAION).34
GCA is common in the Caucasian population,1 but its prevalence seems to be extremely low in the Asian population.56 The incidence of GCA is unknown in Korea, with only a few case reports having been published.7891011 Physicians and ophthalmologists therefore widely believe that cases of AAION associated with GCA are extremely rare in Asian populations. Unfortunately this belief may occasionally lead to misdiagnosis and consequent permanent vision loss, which sometimes occurs bilaterally.
The aims of this study were to estimate the incidence of AAION associated with GCA among patients with presumed AION in a single medical center in Korea, and to delineate the distinctive clinical features of AAION associated with GCA in Korean patients based on our own case series and cases reported in the literature.
Go to : 
METHODS
Subjects
Consecutive cases of AAION associated with GCA among the patients with presumed AION who visited the neuro-ophthalmology clinic at Pusan National University Yangsan Hospital from January 2013 through August 2018 were analyzed retrospectively. This study was reviewed and approved by the Institutional Review Board of Pusan Nation University Yangsan Hospital, Yangsan, South Korea (approval no. 05-2018-188). All study procedures adhered to the tenets of the Declaration of Helsinki.
Patients were diagnosed with presumed AION [both AAION and non AION (NAION)] if all of the following criteria were present or true: 1) an age at onset of >50 years, 2) acute optic neuropathy (sudden onset of decreased visual acuity and/or abnormal visual field consistent with ischemic optic neuropathy with a relative afferent pupillary defect) within the previous 14 days, 3) pale or hyperemic optic disc swelling and/or delayed choroidal filling demonstrated in fluorescein angiography, and 4) all other possible causes of acute optic neuropathy excluded, including optic nerve tumor, retinal vessel occlusion, autoimmune disease, inflammatory conditions, cancer masquerade syndromes, and other infectious etiologies.1213
We additionally classified AAION and presumed NAION in this study cohort as follows. AAION associated with GCA was diagnosed if three or more of the following GCA diagnostic criteria were met:14 1) age at onset of >50 years, 2) new-onset headache, 3) temporal artery abnormality as indicated by tenderness or reduced pulsation in a physical examination, 4) elevated erythrocyte sedimentation rate (ESR) of >50 mm/h, and 5) abnormal temporal arterial biopsy findings indicating necrotizing vasculitis with predominant mononuclear cell infiltration or granulomatous inflammation. The other patients with ischemic optic neuropathy who did not fulfill the GCA diagnostic criteria were diagnosed as presumed NAION.
We investigated medical records to determine the presence of systemic illness, and reviewed the presenting symptoms and/or signs of AAION. We evaluated the initial and final best-corrected visual acuities (BCVA), intraocular pressure, slit-lamp biomicroscopy findings, dilated fundus examination findings, Humphrey visual field test results, and optic disc and fundus photographs (Kowa Co., Tokyo, Japan) at each follow-up visit in the patients with AAION associated with GCA. The findings of fundus fluorescein angiography, indocyanine green angiography, and contrast-enhanced MRI of the brain and orbit were also reviewed for the patients with AAION.
Literature search and review
The PubMed, MEDLINE, Google Scholar, and Research Information Sharing Service (www.riss.kr) databases were searched in October 2018. Papers containing the terms ‘arteritic anterior ischemic optic neuropathy’ or ‘giant cell arteritis’ in the main text, ‘Korean’ in the title or abstract, and ‘Korea’ in the affiliation of the corresponding author were identified. We also conducted a literature search to identify Caucasian AAION patients, and compared the data of the Korean and Caucasian cohorts.
Go to :
RESULTS
Incidence of AAION associated with GCA at a single medical center in Korea
The medical records of 142 patients with AION were collected from the clinical medical record search program provided by Pusan National University Hospital, and the medical records of all patients were reviewed. Three patients (2.1%) were finally diagnosed with AAION: two (cases 5 and 7) had biopsy-confirmed GCA, and one (case 6) met the GCA diagnostic criteria (new-onset headache, elevated ESR, and tenderness in the temporal area). The median age of the patients with AAION was 75 years (range, 68–81 years), and all of them were female. Two had bilateral AAION. The median visual acuity of the affected eye was 20/2,000 at the initial visit [range, no light perception (NLP) to 20/80] and 20/2,000 at the final visit (range, NLP to 20/100).
The demographic and baseline characteristics of the patients with AAION associated with GCA in our study group are provided in Table 1. Presumed NAION was diagnosed in 139 (97.9%) patients. These patients had a median age of 68 years (range, 50–96 years), 76 (54.7%) of them were female, and 5 (3.6%) had bilateral involvement. The median visual acuities of the affected eye at the initial and final visits were 20/100 (range, NLP to 20/25) and 20/63 (range, NLP to 20/20), respectively.
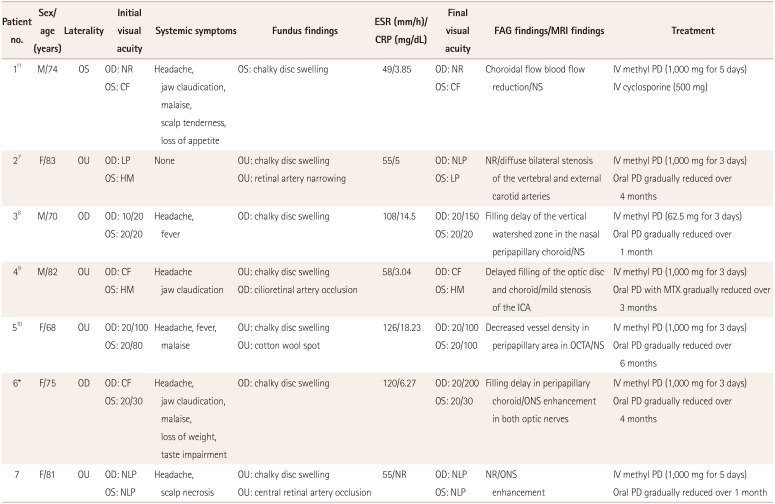
Table 1
Summary of cases of AAION associated with GCA in Korea
*Not confirmed in biopsy.
AAION: arteritic anterior ischemic optic neuropathy, CF: counting fingers, CRP: C-reactive protein, ESR: erythrocyte sedimentation rate, F: female, FAG: fluorescein angiography, GCA: giant-cell arteritis, HM: hand motion, ICA: internal carotid artery, IV: intravenous, LP: light perception, M: male, MRI: magnetic resonance imaging, MTX: methotrexate, NLP: no light perception, NR: not reported, NS: no significant findings, OCTA: optical coherence tomography angiography, OD: right eye, ONS: optic nerve sheath, OS: left eye, OU: both eyes, PD: prednisolone.
![]()
Clinical features of AAION associated with GCA in Korean patients
Five Korean patients with AAION associated with biopsy-confirmed GCA were identified in the literature review, one of whom was included in the cohort of the current study. Two other patients with AAION associated with GCA from our study cohort were identified in the literature search. Eleven eyes of seven patients with AAION associated with GCA were evaluated. Because our study included consecutive patients during the research period, one previously reported case (case 5) was included in this investigation.
The clinical features and treatment outcomes are presented in Table 1. The 11 eyes comprised 2 patients with the simultaneous onset of bilateral AAION, 2 patients who developed contralateral vision loss after 2–4 weeks, and 3 patients who had unilateral involvement only. Five patients (71.4%) had severe vision loss (BCVA of <20/200) at the initial visit. In these cases the optic disc appeared chalky and swollen, but neither peripapillary hemorrhages nor hard exudations were found. The retinal cotton spot was observed in four eyes, and retinal artery occlusion or narrowing was observed in three eyes (Fig. 1, 27.3%). Typical systemic symptoms associated with GCA were present before and at the time of vision loss in six patients (85.7%), including headache and at least one of the following symptoms: scalp tenderness, jaw claudication, fever and general malaise, and anorexia and weight loss. One patient presented with occult GCA; that is, no systemic symptoms or signs. One patient presented with scalp necrotic lesions (Fig. 1). No patients complained of diplopia. Contrast-enhanced MRI of the orbit revealed abnormal enhancement along the bilateral optic nerve sheath (ONS) in two patients (cases 6 and 7). The mean ESR was 71.4 mm/h (range, 49–126 mm/h) and the mean C-reactive protein level was 8.48 mg/L (range, 3.04–18.23 mg/L). High-dose intravenous methylprednisolone and subsequent oral corticosteroids with tapering was administered in all cases. The follow-up period ranged from 3 to 12 months. At the final follow-up, the disc edema had resolved in all eyes and the ESR had normalized, but there was a significant improvement of ≥2 lines in the visual acuity in only one eye (9.0%). All patients eventually developed diffuse optic atrophy in the affected eyes, and four patients were considered legally blind (57.1%).
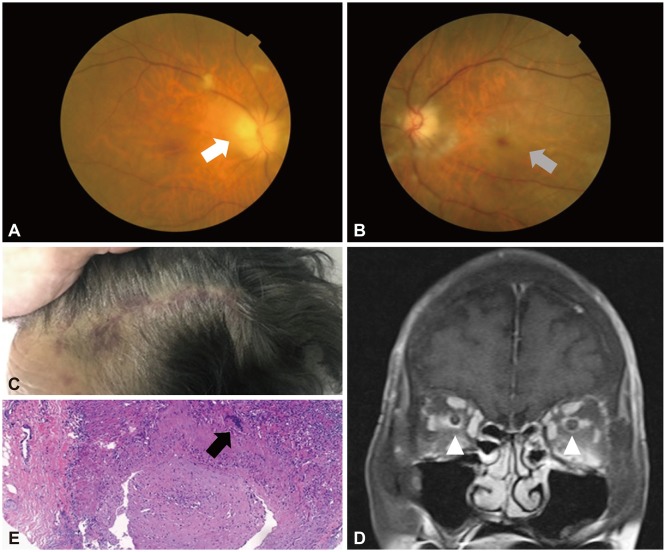 | Fig. 1Clinical findings in case 7. Fundus photographs revealed chalky optic disc swelling with cotton wool spots in the right eye (arrow, A) and pale optic disc swelling with ischemic macular edema and central retinal artery occlusion (arrow, B). C: Multiple purpuric skin lesions were observed in the frontoparietal scalp area. D: Bilateral optic nerve sheath enhancement was observed in contrast-enhanced orbital MRI (arrowheads). E: Histology revealed giant cells (arrow), lymphohistiocytic cells infiltration, and arterial wall thickening with elastic fiber fragmentation. Hematoxylin-eosin staining (×40).
|
Go to :
DISCUSSION
The true prevalence rates of AAION and NAION in Korea could not be concluded from our data, but we found a markedly lower relative incidence of AAION (2.1%) compared to NAION (97.9%). The clinical manifestations of AAION associated with GCA in Korean patients were similar to those described previously, with the exception of the laterality (Table 2).
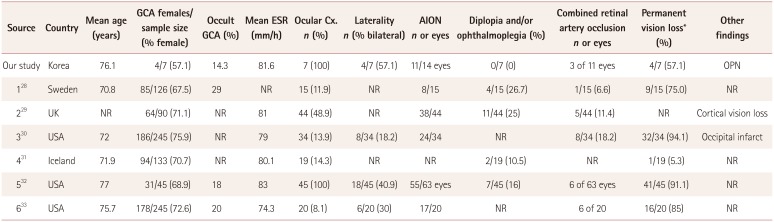
Table 2
Comparison of ocular complications associated with GCA between Korean and Caucasian patients
![]()
Epidemiology is an important tool for assessing risk and the genetic or environmental relationships while considering the likelihood of a range of differential diagnoses. GCA is the most common systemic vasculitis in patients aged >50 years, and the prevalence of GCA is lower in Asian than Caucasian populations.6 Pereira et al.5 reported this finding for a United States population, and concluded that the etiology of GCA is more strongly associated with the genetic background than environmental influences. Hayreh15 analyzed a large data set for a predominantly Caucasian clinicbased cohort to reveal prevalence rates of 10% and 90% for AAION and NAION, respectively. In contrast, Gruener et al.16 reported a markedly lower prevalence for AAION vs. NAION in an Arab population, of 2.3% vs. 97.7%, respectively; these values are similar to our current data. This discrepancy between Caucasians and Arabs may indicate that the prevalence of GCA varies with race.
All patients in the current study who were older than 60 years presented with the rapid onset of severe vision loss and developed the typical pallid ‘chalky white’ disc edema. In particular, these ocular findings (i.e., chalky white disc swelling with or without retina ischemia) were a distinctive feature of the patients with AAION. We therefore suggest that a detailed fundus examination could be beneficial for the differential diagnosis of patients with NAION. Typical systemic symptoms of GCA were present in most of the patients, and headache, jaw claudication, and malaise were common symptoms in our Korean patients with GCA. However, one patient had occult GCA, with the ocular involvement of GCA but without any systemic symptoms or signs of GCA. Hayreh et al.3 reported that GCA should be considered in persons aged >55 years with amaurosis fugax or vision loss, the development of acute ocular ischemia, and abnormal C-reactive protein levels with or without an elevated ESR and systemic symptoms, because 21.2% of GCA patients had occult presentations.
GCA has recently been recognized as a systemic vascular disease that is not confined to the ocular arteries.17 Previous studies have demonstrated that approximately one-third of patients with GCA develop serious peripheral vascular disease during long-term follow-up,18 and there is a growing body of evidence that unrecognized extraocular involvement could be even more common. One patient in our cohort had scalp necrosis as an extraocular involvement, and this in association with GCA is associated with a higher risk of vision loss and a higher mortality rate compared to GCA without scalp necrosis.1920 In addition, scalp necrosis after steroid treatment may indicate an inadequate steroid dosage.20 Therefore, scalp necrosis in GCA should be considered as a more-aggressive disease process and treated with a sufficient dose of steroid to prevent a poor prognosis. As in result, we recommend that regular workups for systemic vascular complications as well as ocular complications should be performed in patients with AAION as sociated with GCA.
Contrast-enhanced orbital MRI was not performed in the present typical GCA cases because GCA is mainly diagnosed based on fundus findings, the presence of systemic symptoms, laboratory findings, and a temporal artery biopsy. Enhancement of the ONS in contrast-enhanced MRI is an important finding for diagnosing optic perineuritis (OPN).21 OPN has generally been considered an idiopathic disease, but it occasionally occurs as a manifestation of specific infectious, systemic inflammatory disorders or GCA.212223242526 However, Morotti et al.25 suggested that ONS enhancement related to GCA may be underestimated due to the atypical clinical features of GCA and since corticosteroid therapy tends to be introduced early before GCA has been confirmed pathologically. Most cases of OPN exhibit dramatic improvement after steroid treatment,2122 whereas the cases of ONS enhancement with GCA in the literature2425 as well as those in the current study did not respond to steroid treatment. This suggests that optic nerve damage in GCA with ONS enhancement is linked to not only ONS autoinflammation but also ischemic damage to the optic nerve. However, Liu and Miller27 reported that cases of unilateral AAION associated with GCA exhibited bilateral ONS enhancement in contrast-enhanced MRI. We experienced a similar finding in case 6, but we could not conclude the prevalence of ONS enhancement associated with GCA, and the possibility of GCA should be considered in patients with presumed OPN exhibiting a poor response to steroid treatment, elevated ESR, pale optic disc swelling combined with retinal artery narrowing, or systemic symptoms related to GCA.
All of our patients received steroid treatment, but this resulted in improvement in only one of them, with most patients having poor final visual outcomes. This finding is similar to previous reports.282930313233 However, >50% of our Korean patients with AAION associated with GCA had bilateral involvement. Although we could not identify the true incidence of bilateral involvement in our Korean patients with AAION due to the small number of included patients, our findings highlight that AAION associated with GCA needs to be treated promptly, and it may still cause permanent bilateral vision loss.
Our study was subject to several limitations. We only investigated a small number of patients whose exact medical history was not available in the literature; however, most of the patients in this study did have biopsy-confirmed GCA. We could not report the incidence and morbidity rates of AAION associated with GCA in our Korean population, and so our study could only address the ratio of AAION-to-NAION cases. We also could not conduct statistical comparisons between AAION and NAION in our Korean population, but the prevalence of AAION was much lower than that of NAION. Cardiovascular risk factors, a small optic disc, and obstructive sleep apnea have been strongly associated with NAION.343536 We therefore suggest that a further study involving a large population survey is needed to determine the genetic association and/or environment influences in AAION and/or NAION among different races. An additional drawback of our study is that we limited our analysis to a literature review and comparison. One striking finding was that the clinical manifestations of GCA in our Korean population were similar to those in our Caucasian population. Moreover, we found that prompt diagnosis and early treatment are also very important for preventing permanent and sometimes bilateral vision loss in Korean patients.
In conclusion, AAION associated with GCA is a very rare condition in Korea. However, GCA should be considered in cases of ischemic optic neuropathy because AAION patients have poor visual outcomes, which sometimes occur bilaterally.
Go to :
 XML Download
XML Download