

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Neurocritical care has been classified as a subspecialty of neurology that primarily focuses on critical care for neurologically ill patients and neurological care for critically ill patients.1 Previous studies have found that providing neurocritical care services may improve clinical outcomes in critically ill patients with neurological diseases, including traumatic brain injury, intracerebral hemorrhage, and subarachnoid hemorrhage.23456 Social awareness about patient safety has also increased the awareness about high-quality neurocritical care among patients and neurologists. Having a neurointensivist staff member and organizing the intensive care unit (ICU) infrastructure are crucially important for providing adequate care to neurocritically ill patients.78 However, there is currently a lack of full-time neurointensivists in Korean hospitals despite the presence of neurological, neurosurgical, or general ICUs in most general hospitals.9 To our knowledge, the effects of full-time neurointensivist staffing in a dedicated neurological intensive care unit (NRICU)—which may comprise a different patient population than a neurosurgical ICU, a combined neurological and neurosurgical ICU, or a general ICU—on the quality of care and outcomes of neurocritically ill patients have not been described previously.
The ICU can be organized in two ways in terms of the role played by an intensivist, and this may influence the quality of critical care and patient outcomes.10 In an open-type ICU, patients are admitted to the ICU under the care of a nonintensivist physician, and an intensivist is available to provide their expertise via elective or mandatory consultations.11 In a closed-type ICU, patient care is transferred to an intensivist who is responsible for the clinical management and family meetings.12 For general critical care, the closed-type ICU is thought to be a more favorable setting than the open type in terms of patient safety and efficiency in the use of ICU resources.111314 However, studies of the effects of the two ICU types on quality of care and patient outcomes in the field of neurocritical care are lacking.
Here we report the effects of full-time neurointensivist staffing in a closed-type NRICU on the quality of critical care and patient outcomes.
Go to : 
METHODS
Study design and population
A quasi-experimental uncontrolled before-and-after study design was utilized. Patients were included in the current study if they were admitted to the NRICU of the Department of Neurology at Asan Medical Center, Seoul, Korea between March 1, 2010 and February 28, 2016. Patients were excluded if they were younger than 18 years, did not have medical records available for analysis in this study, or if brain death was declared before admission to the NRICU. Two time periods were defined according to the appointment of a neurointensivist: the before period (from March 1, 2010 to February 28, 2013) and the after period (from March 1, 2013 to February 28, 2016). This study was approved by the Institutional Review Boards, and the need for written informed consent was waived because of the retrospective design of the study (IRB No. 2016-0379).
Infrastructure and staffing of the NRICU
The NRICU of Asan Medical Center includes 13 beds, 7.5 of which are formally assigned to patients admitted to the Department of Neurology. When critically ill patients are admitted to the Department of Neurology, they are admitted routinely to the NRICU. During the before period, these patients were managed by neurology residents, neurology fellows, and attending neurologists, and elective consultations with general intensivists were performed as necessary (open-type ICU). A full-time neurointensivist (S.-B.J.) was appointed on March 1, 2013, after which neurology patients in the NRICU were managed by neurology residents and this neurointensivist. Patient care in the NRICU was transferred to the neurointensivist (closed-type ICU). For 92 patients with seizures or status epilepticus, the neurointensivist provided mandatory comanagement with attending neurologists; such management was transferred completely to the neurointensivist after January 2016. The neurointensivist was also responsible for every consultation to the Department of Neurology for patients with a neurological problem during admission to general ICUs. In addition, the neurointensivist covered one session per week of the outpatient neurology clinic, where he followed up patients discharged from the NRICU and patients previously consulted at general ICUs. There were no other changes to the nurse staffing and infrastructure of the NRICU during the 6-year period of the current study. The characteristics of the NRICU infrastructure are compared between the two time periods in Table 1.
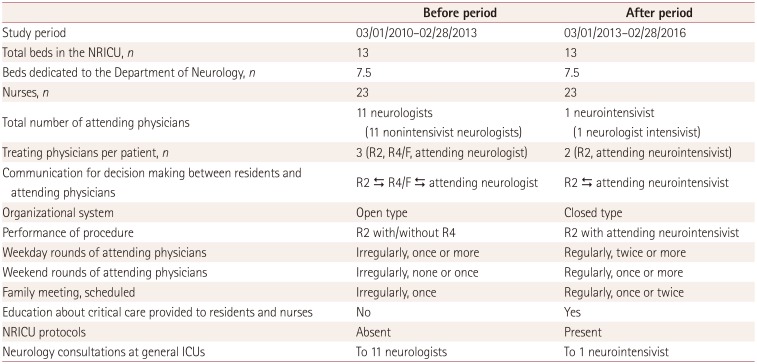
Table 1
ICU infrastructure and practices during the two study periods
![]()
The neurointensivist introduced protocols for use in the NRICU, including barbiturate coma therapy, targeted temperature management, measurement and management of intracranial pressure, osmotherapy, management of malignant infarctions, evaluation of brain death, evaluation and management of meningoencephalitis, and evaluation and management of comatose restoration of spontaneous circulation after cardiopulmonary resuscitation. The neurointensivist held regular sessions to educate neurology residents and NRICU nurses regarding these protocols and general issues related to neurocritical care.
Data collection
Electronic medical record and medical cost data were queried by the Information Technology Service Management of Asan Medical Center for all patients admitted to the NRICU during the study period. Data were obtained on demographics, comorbidities, vital signs, laboratory tests, medications, procedure records, complications, and clinical status (severity of illness) on admission, including scores on the Glasgow Coma Scale and Acute Physiology and Chronic Health Evaluation II (APACHE II). Additional patient information and formal reports on imaging investigations were retrieved from the electronic medical records and the picture archiving and communication system, respectively. Information on the survival status up to 6 months after admission to the NRICU was obtained from the electronic medical records. Hospital-acquired pneumonia and catheter-associated urinary tract infection were defined in accordance with international guidelines.1315 Venous thromboembolism was diagnosed when computed tomography and/or ultrasonography revealed a thrombus in the venous structures. Gastrointestinal bleeding was diagnosed in an endoscopy examination. The predicted in-hospital mortality rate was calculated based on the APACHE II score.16
Neurology consultations, inter-ICU transfers, family satisfaction, and medical costs
The number of neurology consultations was assessed from general ICUs and the number of intrahospital inter-ICU transfers. Transfers were categorized into transfers from general ICUs (nonneurology departments) to the NRICU (neurology department) and transfers from the NRICU to general ICUs. The current study regarded the numbers of neurology consultations and inter-ICU transfers from general ICUs to the NRICU as proxies for the satisfaction of general intensivists (nonneurologists) with the neurological service provided by neurologists during the before period or by a neurointensivist during the after period.
A hospital customer-satisfaction team conducted a patient-family satisfaction survey regularly (twice yearly) throughout the 6-year study period. This survey consisted of a face-to-face interview with 30 families of patients admitted to the NRICU who were chosen randomly by the team. The questionnaire comprised one item assessing the general satisfaction with medical services in the NRICU and four items assessing opinions about physicians (neurologists or a neurointensivist), including their kindness, trust, explanations, and availability for family meetings. Each item of the questionnaire was rated on a 5-point scale, with the lowest score representing dissatisfaction and the highest score representing satisfaction.
Total medical costs incurred during the hospital stays were calculated for the two study periods. They were organized into cost per year and cost per patient, with the latter further categorized into deductible and nondeductible costs.
Statistical analysis
Data are presented as median and interquartile range (IQR) values for continuous variables and as number and percentage values for categorical variables. Baseline characteristics (demographics, comorbidities, diagnosis, and severity of illness), clinical management, quality indicators, clinical outcomes, the number of neurology consultations, the number of inter-ICU transfers, and the family satisfaction scores were compared between before and after appointing a full-time neurointensivist. Pearson's χ2 test and Fisher's exact test were used for categorical variables, and the t test or the Mann-Whitney U test was used for continuous variables, as appropriate. The Kaplan-Meier method was used to generate survival curves, and the curves were compared using a Cox proportional hazards analysis with adjustments for demographics, comorbidities, and severity of illness (total acute physiology scores on the APACHE II score). Statistical significance was defined as a two-tailed p value of <0.05. All data were analyzed using SPSS (version 21, IBM Corporation, Armonk, NY, USA).
Go to :
RESULTS
There were 15,210 admissions to the Department of Neurology during the study period: 7,550 during the before period and 7,660 during the after period. Of these, 1,057 and 1,229 patients were admitted to the NRICU during the before and after periods, respectively. Sixty-two patients who were admitted to the NRICU during the before period were excluded for the following reasons: younger than 18 years (9 patients), medical records unavailable due to transfer to the Department of Psychiatry (3 patients), and hospital readmission to the NRICU (50 patients). Likewise, 25 patients who were admitted to the NRICU during the after period were excluded for the following reasons: younger than 18 years (3 patients), medical records unavailable (2 patients), hospital readmission to the NRICU (18 patients), and brain death declared prior to admission to the NRICU (2 patients). The remaining 2,199 patients were included in the final analysis, comprising 995 (13.2%) during the before period and 1,204 (15.7%) during the after period. Accordingly, the number of patients who were admitted to the NRICU increased by 21% after appointing a neurointensivist (p<0.001). The 2,199 patients included 1,354 (61.6%) men. The patients were aged 63.4±14.6 years (mean±SD; median, 66.0 years; IQR, 55.0–74.0 years), and their APACHE II score was 11.1±6.3 (median, 10.0; IQR, 7.0–15.0; Table 2).
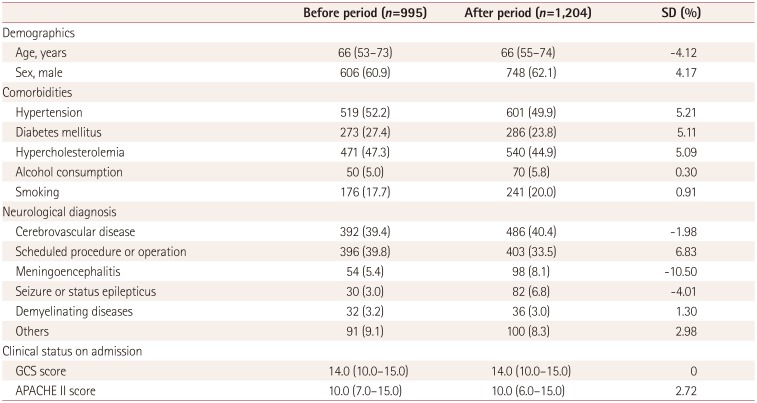
Table 2
Baseline characteristics
![]()
Clinical practices, quality indicators, and outcomes
The clinical practices and complications during admission to the NRICU are listed in Table 3. Prophylaxis for deep-vein thrombosis with subcutaneous unfractionated or low-molecular-weight heparin was performed more frequently during the after period than during the before period (p<0.010). There were nonsignificantly fewer patients with kidney injury requiring continuous renal replacement therapy during the after period than during the before period (p=0.070). The specialized neurocritical care treatments of continuous electroencephalographic monitoring (p<0.001), intracranial pressure monitoring (p=0.078), therapeutic hypothermia (p<0.001), and barbiturate coma therapy (p=0.013) were performed more frequently during the after period than during the before period. The complication rates in the NRICU did not differ significantly between the two periods.
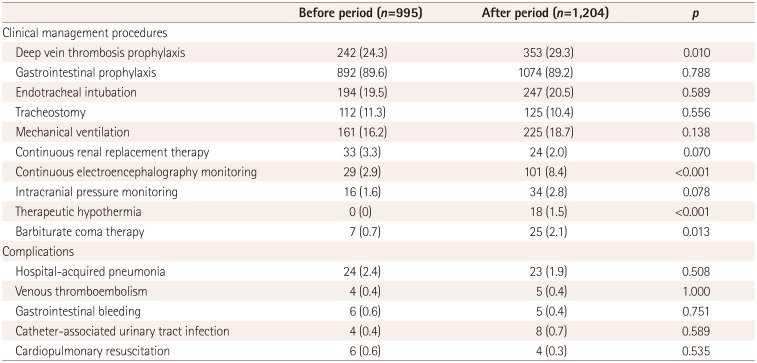
Table 3
Clinical practice and complications
![]()
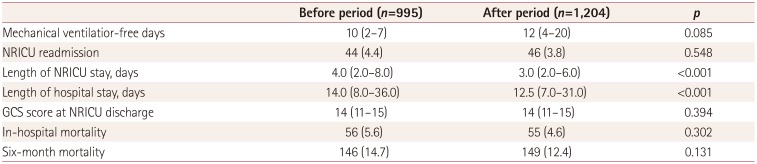
Patient outcomes and quality indicators regarding clinical management are presented in Table 4. Among the patients on mechanical ventilation, there were nonsignificantly more mechanical ventilatior-free days during the after period than during the before period [median, 12 days (IQR, 4–20 days) vs. median, 10 days (IQR, 2–7 days), p=0.085]. The ICU stay was significantly shorter during the after period than during the before period [median, 3 days (IQR, 2–6 days) vs. median, 4 days (IQR, 2–8 days), p<0.001], as was the hospital stay [median, 12.5 days (IQR, 7–31 days) vs. median, 14 days (IQR, 8–36 days), p<0.001] . The predicted in-hospital mortality rate was 9.8% during the before period and 9.7% during the after period according to APACHE II scores; the corresponding observed rates were 5.6% (56/995) and 4.6% (55/1,204), respectively. The 6-month mortality rate did not differ significantly between the after and before periods [n=149 (12.4%) vs. n=146 (14.7%), p=0.131]. Applying a Cox proportional hazards model revealed that appointing a neurointensivist did not result in statistically significant differences in 6-month mortality after adjustments for demographics (age and sex), comorbidities (hypertension, diabetes mellitus, hypercholesterolemia, alcohol, and smoking), and acute physiology scores on the APACHE II score (hazard ratio, 0.82; 95% confidence interval, 0.652–1.031; p=0.089) (Fig. 1).
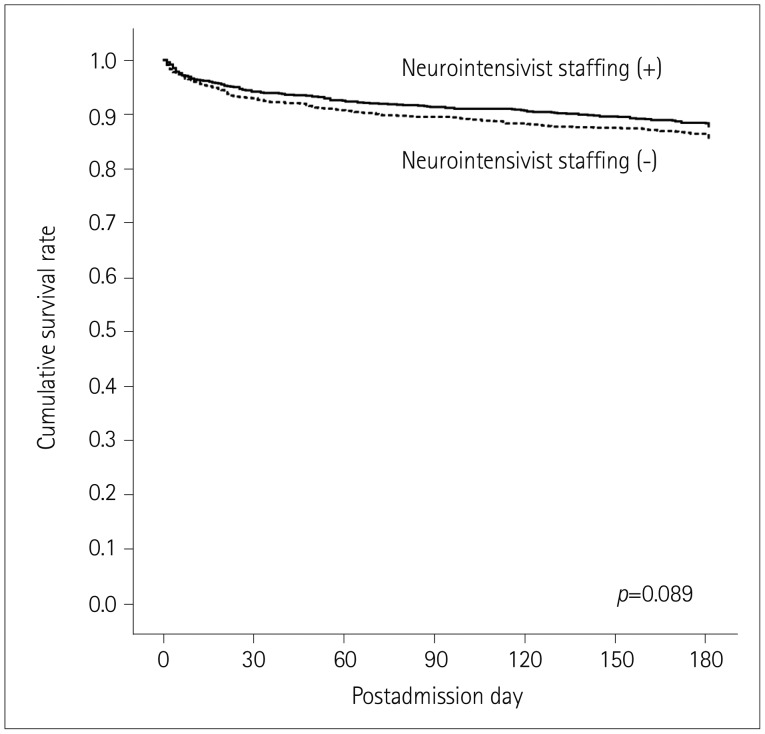 | Fig. 1Presence of a neurointensivist and 6-month survival outcomes. Kaplan-Meier curves showing the proportion of surviving patients stratified by whether a neurointensivist was appointed.
|
Table 4
Clinical outcomes and quality indicators
![]()
Neurology consultations, inter-ICU transfers, and family satisfaction
The number of neurology consultations increased after appointing a full-time neurointensivist, from 2,070 (9.7%) to 3,097 (14.7%) (p<0.001). Inter-ICU transfers from general ICUs to the NRICU [21 (2.1%) vs. 40 (3.3%), p=0.111] increased nonsignificantly, and inter-ICU transfers from the NRICU to general ICUs [29 (2.9%) vs. 8 (0.7%), p<0.001] decreased significantly (Table 5). The mean scores for the general satisfaction of patient families with medical services during admission to the NRICU increased from 78.3 to 89.7; that is, the degree of general satisfaction increased by 14.6%. The mean scores for questions about physicians in terms of their kindness (from 81.3 to 91.7), decision-making (from 81.0 to 91.3), explanations (from 79.7 to 91.0), and availability for family meetings (from 72.3 to 85.0) also all increased.
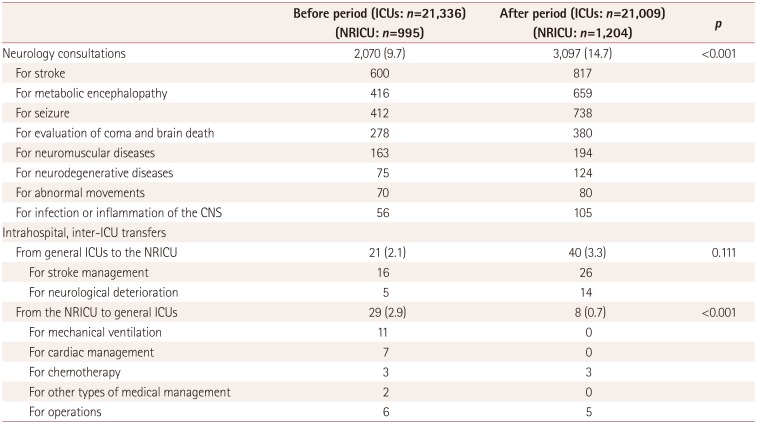
Table 5
Neurological consultations and inter-ICU transfers among patients admitted to the NRICU and general ICUs
![]()
Medical costs
The total medical cost incurred during the hospital stays was 15,325,767,625 won for 995 patients during the before period and 16,880,071,965 won for 1,204 patients during the after period. The annual medical cost increased from 5,108,589,208 won during the before period to 5,626,690,655 won during the after period. Thus, the annual hospital income increased by 518,101,447 won after appointing a single neurointensivist. The total median medical cost per patient was 10,993,897 won during the before period and 9,914,534 won during the after period (p=0.001). The medical cost paid by patients decreased from 3,925,302 won to 3,288,087 won (p<0.001), and that paid by the National Health Insurance Corporation decreased from 6,811,628 won to 6,214,627 won (p=0.026) after appointing a neurointensivist. Thus, both the medical cost per patient paid by the patients themselves and that paid by the National Health Insurance Corporation decreased significantly after appointing a neurointensivist (Table 6).
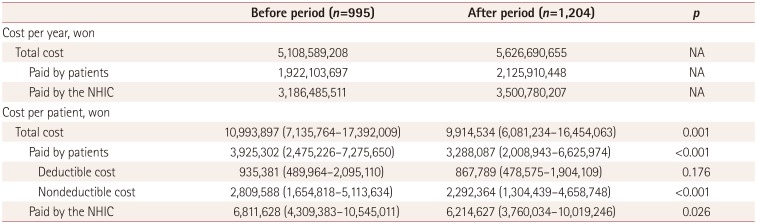
Table 6
Medical costs incurred during hospital stay
![]()
Go to :
DISCUSSION
We investigated the effect of appointing a full-time neurointensivist to manage a closed-type NRICU. After appointing a neurointensivist, the length of NRICU stays decreased by 1 day (from 4 to 3 days); this decrease was maintained in our analysis of the length of hospital stays (from 14.0 to 12.5 days). The decreases in the lengths of ICU and hospital stays did not occur at the expense of patient safety, including the ICU readmission rate. Rather, the decrease in length of stay allowed significantly more admissions to the NRICU (which increased by 21%), which demonstrates the more efficient utilization of NRICU beds. Furthermore, the in-hospital and 6-month mortality rates showed decreasing tendencies, from 5.6% to 4.6% and from 14.7% to 12.4%, respectively, but these changes were not statistically significant. Neurology consultations from general ICUs increased by 50%. Inter-ICU transfers from the NRICU to general ICUs decreased, whereas those from general ICUs to the NRICU increased. The patient families also reported an increase in general satisfaction regarding the medical services provided by physicians (neurologists or a neurointensivist) during admission to the NRICU. Moreover, the medical cost for each patient incurred during the hospital admission and paid either by patients or the National Health Insurance Corporation decreased significantly. However, the total medical costs paid to the hospital increased due to the number of patients increasing. Thus, the current study suggests that appointing a full-time neurointensivist in a preexisting NRICU improves the quality of care and outcomes for neurocritically ill patients.
The in-hospital mortality rate in the current study decreased by 1% after implementing a full-time neurointensivist; that is, 1 more of every 100 neurocritically ill patients survived after this change. However, this finding did not reach statistical significance, which is probably due to the sample size being insufficient and the already low mortality rate of the preexisting NRICU infrastructure of the study hospital. Alternatively, the lower mortality in the current study compared with previous studies may have been due to differences in the study populations: patients with traumatic brain injury, intracerebral hemorrhage, and subarachnoid hemorrhage who are admitted to a neurosurgical ICU or a combined neurological and neurosurgical ICU generally have a higher mortality rate than patients with ischemic stroke and other neurological diseases.1718 The observed in-hospital mortality rate was below that expected based on APACHE II score during both the before period (5.6% vs. 9.8%) and the after period (4.6% vs. 9.7%), respectively. The decrease in the 6-month mortality rate may be related to the beneficial effects provided by having a neurointensivist in the NRICU because appropriate care during the critical phase of illness may improve the long-term outcomes of patients.19 Our findings suggest that appointing a neurointensivist and changing the organization of an NRICU from an open type to a closed type can reduce patient mortality. However, this interpretation requires confirmation since this was a single-center study and our findings did not reach statistical significance.
Studies assessing the satisfaction of general intensivists and the families of patients in the NRICU are lacking. We considered the number of neurology consultations and inter-ICU transfers as proxies for the satisfaction of general intensivists who were working in nonneurology ICUs with the performance of neurologists or the neurointensivist. These proxies were used because no data from prospective surveys of coworkers were available, and a survey initiated during the after period could be affected by recall bias. The number of neurology consultations from general ICUs and inter-ICU transfers from general ICUs to the NRICU increased after appointing a neurointensivist. This could be interpreted as indicating that the satisfaction of general intensivists with the neurology service provided by the neurointensivist increased compared to the service provided by neurologists. Alternatively, the decrease in the number of inter-ICU transfers from the NRICU to general ICUs might be related to the competence of a closed-type NRICU run by a neurointensivist. To assess the satisfaction of the families of patients, the results of the prospective survey performed during the before period and the after period were available for the current study. These results showed that the general satisfaction of patient families with critical care in the NRICU and with how the physicians performed increased after appointing a neurointensivist. Thus, having a neurointensivist staff member might also satisfy the general intensivists by managing neurological problems occurring in general ICUs and satisfy the patient families by providing improved critical care in the NRICU.
Our study was subject to some limitations. First, a single-center retrospective study inherently has a risk of selection bias, and so the results of our study might not be broadly applicable to other centers. The NRICU of our hospital was separate from the neurosurgical ICU, and the current study was designed to evaluate patients admitted to the NRICU. Thus, most patients who presented with traumatic brain injury, intracerebral hemorrhage, and subarachnoid hemorrhage were not included in the current study. In addition, the infrastructure and environment of a hospital, and the training background, capability, and working environment of the neurointensivist may affect the study results. Second, the quality of critical care and clinical outcomes might have improved due to either appointing a neurointensivist or the availability of new advanced medical technology, given that the study period was 6 years. Improved family satisfaction could also be due to both the neurointensivist and hospital-wide efforts to provide better medical care for hospitalized patients. Likewise, we interpreted the numbers of neurology consultations and inter-ICU transfers from general ICUs to the NRICU as proxies for the satisfaction of our coworking general intensivists, but increases in these numbers might not directly represent increased satisfaction. Third, the clinical outcomes of the patients were defined using the survival rate rather than functional outcomes because the latter data were not available for the current retrospective study. The mortality rate may be an inadequate parameter for evaluating the clinical outcomes of neurocritically ill patients. Fourth, the satisfaction of neurology residents and nurses regarding the education they received about neurocritical care and management in the NRICU was not investigated, because none of the residents and only a small proportion of the nurses were employed in the NRICU throughout the 6-year study period. Fifth, the professional burnout of the neurointensivist was not assessed. Although the current study showed that appointing a neurointensivist was associated with improvements in quality indicators and patient outcomes, running a closed-type NRICU for a prolonged period with a single neurointensivist may eventually lead to negative impacts on patient care and safety due to neurointensivist burnout.20
In conclusion, appointing a full-time neurointensivist and implementing organizational changes for running a closed-type NRICU have beneficial effects on quality indicators of critical care, patient outcomes, and satisfaction of general intensivists and patient families. However, the present results should not be interpreted as evidence that appointing a single neurointensivist is sufficient to run a closed-type NRICU. Given the shortage of neurointensivists in Korea, hospital administrative efforts should also be made to prevent professional burnout and enable shift work for neurointensivists.
Go to :
 XML Download
XML Download