

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Progressive supranuclear palsy (PSP) is a progressive tauopathy characterized by postural instability, dizziness, and recurrent falls.1 Similar signs and symptoms are typically found in patients with impairment of vestibular function.2 Otolith organs detect gravity and linear accelerations and thereby contribute to the vestibulospinal reflexes that prevent patients from falling.3 Impaired function of the otolith organs leads to postural instability,45 and saccular function was shown to be an important factor contributing to the age-related slowing of gait speed.678
A clinically important sign for diagnosing PSP is the presence of saccadic or gaze palsy contrasting with a relatively well-preserved angular vestibulo-ocular reflex (VOR).9 Nevertheless, there are conflicting findings about whether impaired vestibular reflexes contribute to postural imbalance and falls in patients with PSP. For instance, there is some evidence that the angular VOR can be affected when viewing a nearby target.10 Furthermore, the translational VOR, which is important for linear head movements, can be markedly impaired in PSP.10 It was also shown that patients with PSP have disinhibited vestibulo-collic reflexes.11 Corresponding to this, there is some evidence that the amplitudes of cervical vestibular evoked myogenic potentials (cVEMPs) are reduced in patients with PSP,10 indicating a reduced function of the saccule; however, this was not confirmed in subsequent studies.12
There is no systematic approach for vestibular testing in patients with PSP, and data on the correlation between vestibular function and patient symptoms are insufficient. However, major progress in the development of techniques for measuring vestibular function have made it possible to examine and differentiate dysfunctions of all five important vestibular receptors in the inner ear using caloric testing and the video head impulse test (vHIT) for semicircular canal testing,13 and VEMP for otolith function.1415
Therefore, in the present prospective study we systematically investigated the functioning of the semicircular canals, saccule, and utricle, as well as the functions of the ocular motor system and postural balance.
Go to : 
METHODS
Seventeen patients with PSP and 17 age-matched controls with no history of neurological disease were included in this prospective study. Inclusion criteria for the patients were having probable PSP according to the clinical criteria of the National Institute for Neurological Disorders and Society for PSP,1 and being willing and able to participate in the examinations. Exclusion criteria were known other reasons for their stance and gait instability, including other known vestibular diseases such as Ménière's disease, unilateral, or bilateral vestibulopathy, and being unable to stand for 1 min unaided. One patient was excluded in the analysis due to excessive missing data. The age-matched participants underwent a complete neurological examination and had no history of other diseases that could affect gait and postural control. Eight patients were taking medications against symptoms of PSP: (seven were taking L-dopa, one was taking amantadine, one was taking rotigotine, one was taking rasagiline, one was taking donepezil, and one was taking acetyl-DL-leucine).
The details of the included patients are listed in Table 1.
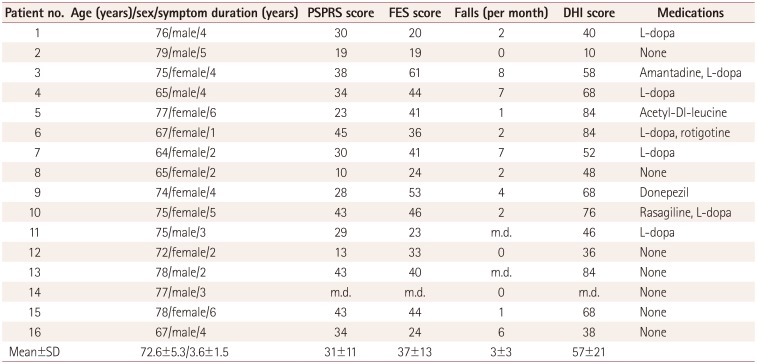
Table 1
Patient characteristics
![]()
All patients received the vHIT to test the horizontal semicircular canal, cVEMPs for saccular function, ocular VEMPs (oVEMPs) for utricular function, video-oculography, and posturography. Seven patients underwent caloric testing.
vHIT and video-oculography
The vHIT and video-oculography were performed with an infrared camera using the EyeSeeCam System® (EyeSeeTec, Fürstenfeldbruck, Germany).15 The system was calibrated using horizontal saccades or smooth pursuit in patients with greater impairments. The vHIT involved making recordings while rotating the head ten times to each side at angular velocities of between 100°/sec and 200°/sec. We analyzed the gain between head and eye movements at 60 msec after the beginning of the head movement. Patients were asked to look at a moving point to test saccades with stimulus amplitudes of 30° horizontally and 20° vertically, smooth pursuit (0.1 and 0.2 Hz), gaze holding (with stimuli of 10° up and down and 20° to the side), and optokinetic nystagmus (with stimulus of 10°/sec).
Vestibular evoked myogenic potentials
In this study we used the Interacoustics Eclipse System with the standard protocol applied in our clinic as described elsewhere16 for examining VEMPs. Subjects were examined while lying supine on a chair with their back elevated 30° above the horizontal. The oVEMP and cVEMP amplitudes are shown as absolute values and corrected amplitudes, which were calculated by dividing the peak-to-peak amplitude by the mean rectified Electromyography level calculated over the prestimulus interval. The amplitude asymmetry ratio for oVEMP and cVEMP was calculated using the following formula reported by Rosengren: asymmetry ratio=[(larger response-smaller response)/(larger response+smaller response)×100].14 An asymmetry ratio exceeding 35% was considered abnormal.
Ocular vestibular evoked myogenic potentials
We used the bone-conducted oVEMP induced by a minishaker (Bruel and Kjaer Mini-Shaker Type 4810; Bruel and Kjaer GmbH, Bremen, Germany) stimulated by 2-msec-long clicks of positive polarity at a repetition rate of two per second. We first tested whether it was possible to use a different gaze angle to minimize bias due to the gaze palsy, and finally decided on a gaze target of approximately 30° above the normal gaze position of the subjects, reaching this point using smooth-pursuit eye movements. The mini-shaker was placed at the Fz position. oVEMPs were recorded with an electrode alignment consisting of a recording electrode placed over the contralateral inferior oblique muscle (approximately 3 mm below the eye and centered beneath the pupil), a reference electrode on the chin, and a ground electrode placed under the chin. Two measurements were made for each eye in order to ensure reproducibility. Responses to 100 stimuli were averaged. The first reliable negative and positive peaks were designated n1 and p1, respectively.
Cervical vestibular evoked myogenic potentials
During cVEMP stimulation the patients were asked to lift their head, which led to a maximal tonic muscle tension of the sternocleidomastoid (SCM) muscle. Air-conducted tone bursts (500 Hz at 125 dB SPL) were delivered monaurally via intra-auricular speakers with foam ear tips. cVEMPs were recorded from an electrode alignment consisting of a recording electrode placed at the midpoint of the belly of the ipsilateral SCM muscle, a reference electrode placed on the manubrium, and a ground electrode placed on the forehead. The first reliable positive and negative peaks were designated p1 and n1, respectively.
Posturography
Postural control was measured using a Kistler (Kistler Instrumente GmbH, Sindelfingen, Germany) platform with the standard protocol as described elsewhere17 under ten different conditions of increasing difficulty: eyes open/head straight, eyes closed/head straight, eyes open/head extended, eyes closed/head extended, eyes open/head straight/foam-rubber platform, eyes closed/head straight/foam-rubber platform, eyes open/head inclined 60°/foam-rubber platform, eyes closed/head inclined 60°/foam-rubber platform, eyes open/tandem stance, and eyes closed/tandem stance. Each stance condition was recorded for 30 sec. Body sway was measured as the total sway path (in meters per minute) and total root mean square (RMS) distance (in millimeters). Due to the large amount of assistance needed during some of the conditions, we concentrated on the following four conditions for the analysis that modulated the visual, vestibular, and somatosensory inputs: eyes open/head straight, eyes closed/head straight, eyes open/head inclined 60°, and eyes open/head straight/foamrubber platform.
PSP Rating Scale, Falls Efficacy Scale, Dizziness Handicap Inventory, and calendar of falls
All subscales of the PSP Rating Scale (PSPRS)18 were applied: history, mentation, bulbar, ocular motor, limb motor, and gait. Scores on the PSPRS range from 0 (no impairment) to 100 (extreme disability). Subjective impairment and fear of falls were assessed by the patients completing the Falls Efficacy Scale (FES)19 and Dizziness Handicap Inventory (DHI)20 questionnaires. The patients also documented their frequency of falls over the previous 3 months, and a mean frequency of falls was calculated.
Standard protocol approvals, registrations, and patient consent
The Ethics Committee of the University of Munich provided approval for this study (IRB No. 65-14). All participants gave written informed consent, and all clinical investigations were conducted according to the principles of the Declaration of Helsinki.
Statistical analysis
Posturographic data were collected and evaluated using MATLAB (MathWorks, Natick, MA, USA), statistical analyses were performed using IBM SPSS Statistics for Windows (version 22.0 released 2013, IBM Corporation, Armonk, NY, USA).
Since the data did not conform to a normal distribution, nonparametric paired testing was performed using the Mann-Whitney U test. Differences were considered significant if p<0.05. We quantified correlations using nonparametric testing with Spearman R values.
Go to :
RESULTS
Patient characteristics
Sixteen PSP patients [9 females, age=72±6 years (mean±SD), disease duration=3.6±1.5 years, PSPRS score=31±11, FES score=37±13, DHI score=57±21, and fall frequency=3±3/month] and 17 age-matched controls (8 females and age=71±6 years) with no history of neurological disease were included in this study (Table 1).
Vestibular testing
The VOR gain was 1.0±0.1 in the patients with PSP. There was no sign of abnormal vestibular function in the seven patients who received caloric testing. Only one patient refused to have VEMPs measured (due to head and neck pain), and the VEMP was not measured in one control due to technical reasons. All of the other subjects had reproducible oVEMP and cVEMP values. There were no significant differences between PSP patients and controls in oVEMP absolute amplitudes (absolute n amplitudes: 7.1±4.1 µV and 5.9±2.2 µV, respectively; absolute p amplitudes: 7.1±3.5 µV and 6.8±3.8 µV), absolute peak-to-peak amplitudes (13.5±7.2 µV and 12.5±5.6 µV, p=0.8), or latencies (n latencies: 11.9±3.4 msec and 11.9±2.8 msec; p latencies: 16.9±3.7 msec and 17.2± 3.3 msec).
There were also no significant differences between PSP patients and controls in cVEMP amplitudes (corrected p amplitude: 0.2±0.1 and 0.2±0.1, respectively; corrected n amplitude: 0.3±0.2 and 0.2±0.1; corrected peak-to-peak amplitudes: 0.6±0.3 and 0.5±0.2, p=0.3) or latencies (p latencies: 17.4± 3.1 msec and 15.9±2.5 msec; n latencies: 25.3±3.5 msec and 24.8±2.8 msec). Three patients had an abnormal cVEMP asymmetry ratio and one patient had an abnormal oVEMP asymmetry ratio. The results of the vestibular testing are summarized in Table 2, 3.
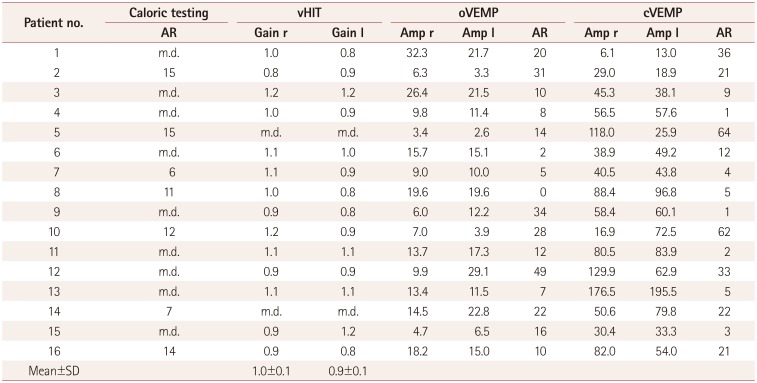
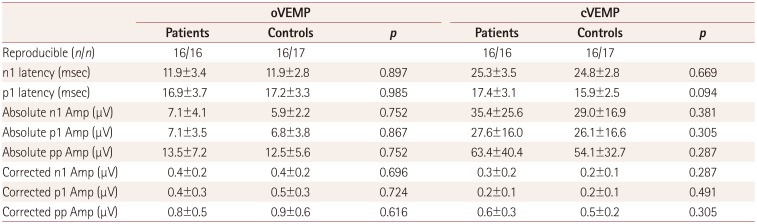
Table 2
Vestibular testing in patients with progressive supranuclear palsy
![]()
Table 3
VEMPs in patients with progressive supranuclear palsy
![]()
Video-oculography
The velocities and amplitudes of saccades were significantly lower in PSP patients than in controls for horizontal saccades (234±92°/sec and 442±66°/sec, and 22±7° and 26±3°, respectively), upward saccades (121±110°/sec and 348±78°/sec, and 9±8° and 16±4/20°), and downward saccades (109±105°/sec and 344±72°/sec, and 9±8/20° and 18±3/20°) (all p<0.05). The velocity and amplitudes of vertical saccades were 66% and 43% lower, respectively, in PSP patients than in controls, while horizontal saccades were reduced by 47% and 17%.
Vertical saccades were affected more than were horizontal saccades in all patients, but it was not possible to conclude whether upward or downward saccades were more affected.
Horizontal smooth pursuit (at 0.1 Hz) differentiated between the PSP patients and age-matched controls (horizontal gain: 0.5±0.3 and 0.8±0.1, respectively; p=0.004), while vertical smooth pursuit did not (upward gain: 0.6±0.3 and 0.7±0.3, p=0.232; downward gain: 0.7±0.3 and 0.7±0.3, p=0.953). More details are provided in Table 4.
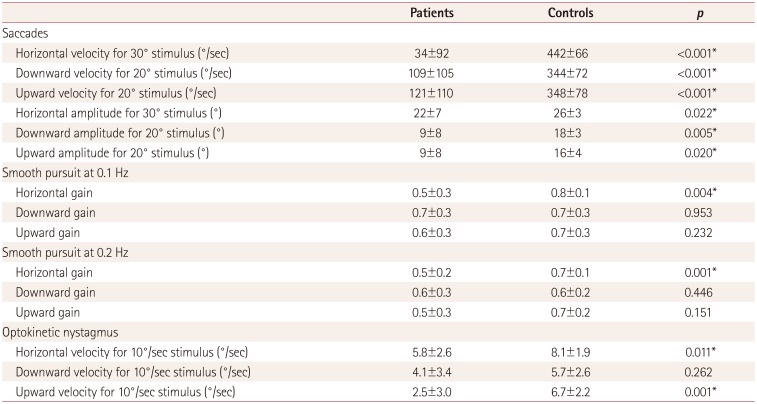
Table 4
Video-oculography in patients with progressive supranuclear palsy and controls
![]()
Posturography
There was no significant difference between PSP patients and controls with regards to the total sway path in the eyes open/head straight/hard platform condition: 1.4±0.6 and 1.4±0.5 m/min, respectively (p=0.669). However, the total RMS was significantly increased in PSP patients than in controls in the same condition (9.3±3.7 and 6.9±2.1 mm, respectively; p=0.032), and especially during modulation of the somatosensory input in the eyes open/head straight/foam-rubber platform condition (20.8±8.5 and 11.4±3.2 mm, respectively; p<0.001), representing RMS increases of 119% and 65%, respectively. The detailed results are presented in Table 5.
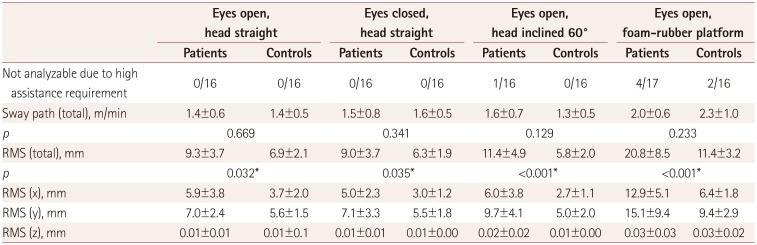
Table 5
Posturography results in patients with PSP and controls
Data are n or mean±SD values. Total sway path did not differ significantly between patients and controls. The total RMS was significantly longer in PSP patients, especially during modulation of the somatosensory input when standing on foam-rubber platform.
*Significant difference between patients and controls with p<0.05.
PSP: progressive supranuclear palsy, RMS: root mean square, x: horizontal, y: anteroposterior, z: vertical.
![]()
Correlation analysis
We found no correlations between either frequency of falls or the FES score and the oVEMP amplitude, cVEMP amplitude, v-HIT score, or saccade amplitude.
Go to :
DISCUSSION
The main findings of this prospective study are as follows:
1) There was no evidence of an impaired horizontal canal in either the high- or low-frequency range or in saccular or utricular function in patients with PSP.
2) The velocity and amplitude of vertical saccades were significantly reduced in the PSP patients. Vertical saccades were affected more than were horizontal saccades in all patients, but it could not be concluded whether upward or downward saccades were more involved. Vertical smooth pursuit can appear normal if patients have an isolated vertical saccade palsy, which strongly supports the importance of the clinical testing of saccades.
3) Quantitative testing of stance and postural imbalance assessed by posturography revealed that the RMS was significantly increased in patients with PSP.
Postmortem studies of patients with PSP have found tau pathology, especially in the subthalamic nucleus, substantia nigra, and internal globus pallidus.21 Patients with severe pathology and especially those with the phenotype of Richardson's syndrome also had tau lesions in the pontine nuclei, dentate nucleus, cerebellar white matter, and frontal cortex.21 PET examinations confirmed tau-related alterations in the midbrain, bilateral globus pallidus, bilateral frontal cortex, and medulla oblongata. Together these findings demonstrate that the affected brain structures differ depending on the phenotype and the genetic background of the patients, and that more-fulminant forms of this disease affect more regions more severely.21
In this context it is important to note that information from the horizontal canal and otolith organs is also processed in the brainstem and in a thalamocortical network22 comprising at least five distinct crossing and noncrossing vestibular pathways between the vestibular nuclei and the core region of the parietoinsular vestibular cortex.23 The basic VOR is generated by a three-neuron link between vestibular receptors, vestibular nuclei, and eye-muscle motoneurons mostly carried by the medial longitudinal fasciculus (MLF) and supported by several other pathways, such as the ascending tract of Deiters.22 Patients with PSP usually exhibit normal responses in the head impulse test (even in severe cases), which was supported by our data. As expected we found normal results for vHIT in all of our patients with PSP, which suggests that the VOR was still working. The presumed pathway for saccular information tested by the sound-evoked cVEMP involves the medial vestibulospinal tract leading to an inhibitory reflex measured from the ipsilateral SCM muscle.14 Utricular information measured by oVEMPs is probably transmitted by the MLF and oculomotor nucleus, leading to increased activity of the inferior oblique muscle on the contralateral side.14 There were no significant differences in the amplitudes or latencies of oVEMP and cVEMP between patients with PSP and controls.
Overall we found no evidence of deficits of either the otolith organs or the horizontal canals in patients with PSP, but there were signs of individual deficits regarding the transmission of vestibular information, such as due to degeneration in the brainstem or supratentorial pathways. This supports earlier findings of reduced thalamic activation appearing to be important for postural imbalance in patients with PSP.24 This could be due to individual variability in affected brain structures (as described above) depending on the phenotype, the genetic background, and the severity, as well as the progression of the disease.21 However, the small number of included patients made further distinction of the above-mentioned items impossible.
In addition to analyzing the vestibular system, this study also applied posturography. There are various data about the movements of patients with PSP when they are performing posturography tasks. One study found a longer total sway path in posturography especially during a modulated sensory input, and a positive correlation between the sway path and frequency of falls.24 Another study found significantly smaller sway path and RMS, but with consistently longer values when the eyes were closed.25 This is compatible with patients with Parkinson's disease showing abnormal postural responses with a small ankle feedback gain and larger hip feedback gain leading to unusually small postural responses as well as a slower increase and smaller peak of the center of pressure in response to surface translations.26
It is reasonable to assume that PSP patients with bradykinesia would have a shorter total sway path in posturography, which measures the distance over time due to missing fast corrective body movements. We believe that the RMS is better than the total sway path for distinguishing between PSP patients and controls. These differences become even clearer during modulation of the somatosensory input, such as when subjects are standing on a foam-rubber platform.
We are aware that our study was subject to several limitations. First, selection bias could have been present when recruiting the patients, with nonparticipation resulting from restrictions due to the disease. The disease duration, PSPRS score, and especially the fall frequency were lower in our patients than in a similar previous study.10 Second, there is a high interindividual variability in oVEMP measurements, and measuring the oVEMP in patients with PSP is more challenging because of their impaired vertical gaze.
In conclusion, this study was performed to address the inconsistencies reported previously for vestibular function in patients with PSP. We found no evidence of impairment of either high- or low-frequency horizontal semicircular function or of otolith organ function in these patients. Therefore, other causes such as degeneration of supratentorial pathways lead to postural imbalance and falls in patients with PSP.
Go to :
 XML Download
XML Download