

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Alemtuzumab is an anti-CD52 monoclonal antibody that depletes and repopulates circulating T and B lymphocytes, thereby shifting cytokine expression toward a less-inflammatory condition.1 Alemtuzumab was shown to be a highly efficacious therapy with tolerable safety in previous studies—including clinical trials—that mainly involved Western patients with multiple sclerosis (MS).234567891011 The prevalence of MS is much higher in Western populations than in Asian populations, and various disease-modifying therapies (DMTs) for MS have been approved later in Asian countries than in Western countries.1213 In order to broaden the use of alemtuzumab as an efficacious and tolerable therapeutic option for patients with active MS, the therapeutic outcomes of alemtuzumab need to be comprehensively evaluated in various racial groups.
Alemtuzumab was approved for use in Korea in 2015, and was reimbursed by the government as a second-line DMT after treatment failure of first-line DMTs starting in December 2015.13 The administration of alemtuzumab basically consists of two courses of infusion, 1 year apart.14 By 2018, a subset of the patients in our clinic could be reached for 2 years of follow-up after initiating alemtuzumab. In this study we aimed to elucidate the efficacy and safety profiles of alemtuzumab in Korean patients with active MS.
METHODS
Patients
This study enrolled 23 consecutive patients with highly active relapsing MS who had been diagnosed using the 2010 McDonald criteria and treated with alemtuzumab at the National Cancer Center (NCC) in Korea between 2015 and 2018.15 Alemtuzumab was administered at 12 mg daily at baseline (for 5 consecutive days) and 1 year later (for 3 consecutive days).14 Prophylactic intravenous methylprednisolone (IVMP; 1 g daily for 3 days) was started immediately before the infusion of alemtuzumab, and oral herpes prophylactic agents were started upon the initiation of alemtuzumab and continued for at least 1 month following the last alemtuzumab infusion.14 All of the patients had exhibited radiological and/or clinical disease activity at 1 year preceding the initiation of alemtuzumab despite the use of first-line DMTs. The Institutional Review Board of the NCC approved this study protocol (approval no. NCC 2014-0146) and written informed consent was obtained from all of the enrolled patients.
Efficacy
Expanded Disability Status Scale (EDSS) scores and brain MRI scans were evaluated prospectively every 3 and 6 months, respectively. Clinical relapse was defined as a clinical exacerbation with objective signs on a neurological examination that lasted at least 48 hours and was confirmed by a neurologist.56 At the time when clinical relapse was diagnosed, EDSS scores and brain and/or spinal cord MRI scans were also assessed according to the presence of clinical symptoms.
The efficacy was investigated clinically and radiologically. The clinical assessment involved an evaluation using the annualized relapse rate (ARR) and changes in EDSS scores. Disability worsening was defined as an increase of ≥1.0 point if the baseline EDSS score was >0, or an increase of ≥1.5 points if the baseline EDSS score was 0; disability improvement was defined as a decrease of ≥1.0 point in patients with a baseline EDSS score of ≥2.0. Radiological assessment was performed using brain MRI, including the presence of new or enlargement of T2-weighted lesions or gadolinium-enhanced T1-weighted lesions.56 No evidence of disease activity (NEDA) was defined as no clinical relapse, no worsening of the EDSS score, and no radiological activity.56
Safety
Adverse events and medical events of interest were investigated. Infusion-associated reactions (IARs) were defined as adverse events that occurred during the initiation of the infusion or within 1 day postinfusion.56 Laboratory tests for hematology, serum creatinine, and urinalysis with microscopy were performed monthly. Thyroid function tests were performed at least every 3 months.
RESULTS
Demographics
The mean age of the 23 patients with MS was 36 years and their female:male ratio was 16:7. Seventeen and 12 of the 23 patients reached the 1-year and 2-year follow-ups after initiating alemtuzumab, respectively. The second course of alemtuzumab in the second year of initiation was administered in 16 patients; 1 patient refused the infusion of the second course of alemtuzumab because of EDSS scores worsening despite receiving alemtuzumab. The median baseline EDSS score was 4.0 (range 0–7.5), the mean disease duration was 9.7 years (range 2–20 years), and the mean follow-up duration after initiating alemtuzumab was 17 months (range 1–24 months). The mean number of previous DMTs before initiating alemtuzumab was 1.8 (range 1–4).
Efficacy
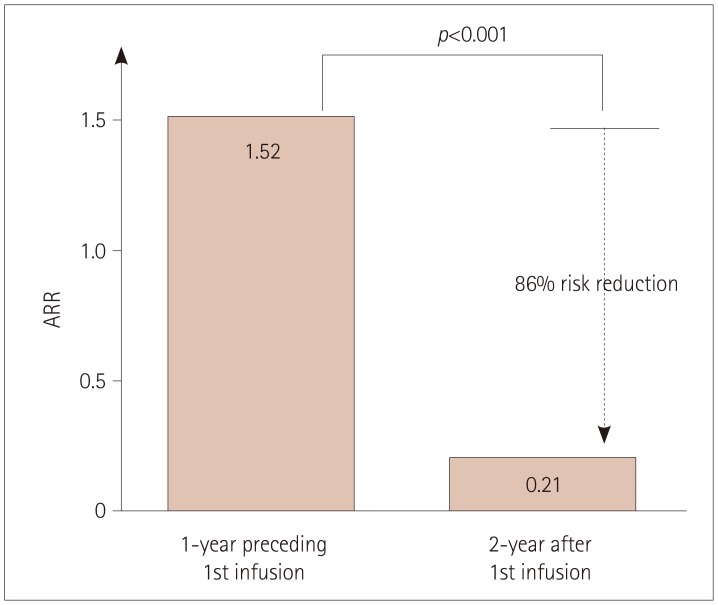
The mean ARR decreased markedly from 1.52 during the 1-year period preceding the alemtuzumab administration to 0.21 after initiating alemtuzumab (p<0.001), indicating a 86% risk reduction (Fig. 1). At the completion of 2 years of follow-up after commencement of alemtuzumab, 9 (75%) of the 12 patients were relapse-free. Five clinical relapses were observed in the other 3 patients, and as we reported previously,16 one clinical relapse (EDSS score at nadir of 9.5) was severe to require additional plasma exchanges after IVMP (1 g daily for 5 days). Three clinical exacerbations (EDSS scores at nadir of 4.0–7.0) were treated with IVMP alone, and one minor relapse recovered without IVMP treatment.
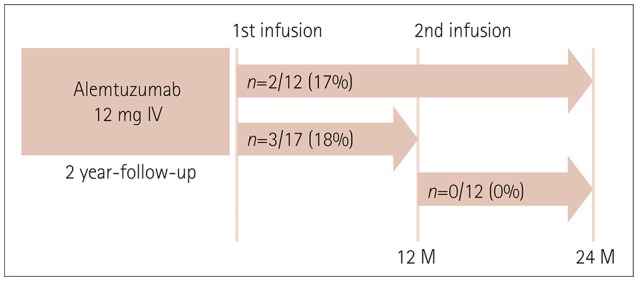
At the completion of 2 years of follow-up after initiating of alemtuzumab in 12 patients, the EDSS score had improved in 3 (25%) patients, remained stable in 7 (58%), and worsened in 2 (17%) (Fig. 2). During the first and second years after initiating alemtuzumab, improvements of EDSS scores were observed in 4/17 (24%) and 1/12 (8%) patients, respectively, stable EDSS scores were observed in 10/17 (59%) and 11/12 (92%) patients, and worsening of EDSS scores was observed in 3/17 (18%) and 0/12 (0%) patients. At the completion of 2 years of follow-up after initiating alemtuzumab, the median EDSS score had improved from 4.0 to 3.3, but this change was not statistically significant. The median EDSS score improved from 4.0 to 3.5 in 17 patients during the first year after initiating alemtuzumab and remained stable at 3.3 in 12 patients during the second year after initiating alemtuzumab.
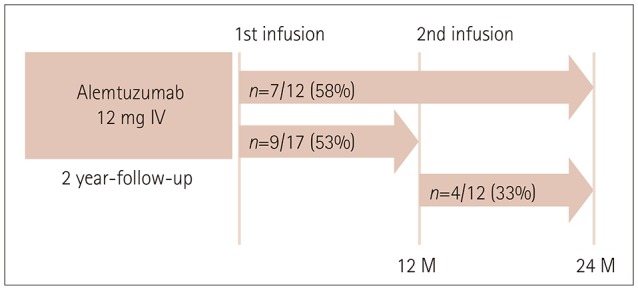
At the completion of 2 years of follow-up after initiating alemtuzumab, radiological activity was observed in 7/12 (58%) patients (Fig. 3). Radiological activity was observed in 9/17 (53%) patients during the first year after initiating alemtuzumab and 4/12 (33%) patients during the second year after initiating alemtuzumab. Radiological activity alone without clinical activity was observed in 4/12 (33%) patients at the completion of 2 years of follow-up after initiating alemtuzumab. During the first and second years after initiating alemtuzumab, 6/17 (35%) patients and 1/12 (8%) patient, respectively, showed radiological activity alone without clinical activity.
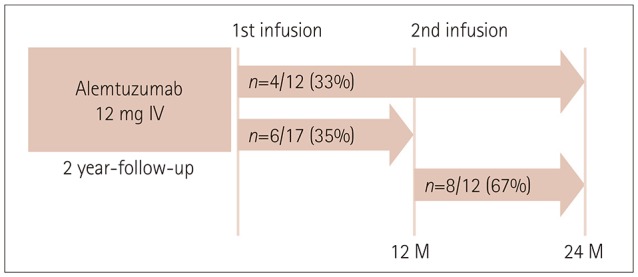
At the completion of 2 years of follow-up after initiating alemtuzumab, NEDA was observed in 4/12 (33%) patients (Fig. 4). During the first and second years after initiating alemtuzumab, NEDA was observed in 6/17 (35%) and 8/12 (67%) patients, respectively. Three of the 4 patients who exhibited disease activity despite the second course of alemtuzumab were treated with a third course of alemtuzumab. In one patient who experienced two severe relapses (EDSS scores at nadir of 9.5 and 7.0, respectively) at 10 months after the first and 10 months after the second infusion of alemtuzumab,16 the treatment was switched to natalizumab. Two of the patients treated with a third course of alemtuzumab experienced clinical relapse with EDSS scores at nadir of 3.5 and 4.0, respectively, and the third patient exhibited only radiological activity.
Safety
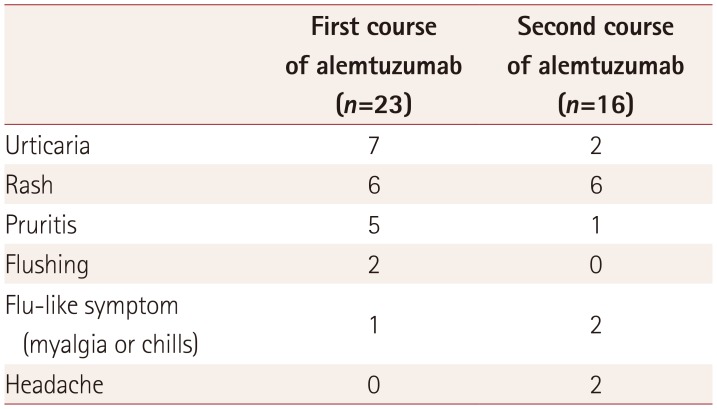
Nineteen (83%) of 23 patients exhibited IARs, including most commonly rash, urticaria, pruritis, flushing, headache, and myalgia. Table 1 lists the details of IARs in patients with MS. During the first and second courses of alemtuzumab, IARs were observed in 17/23 (74%) and 10/16 (63%) patients, respectively. All of these IARs were reversible, and self-limiting or controlled by symptomatic treatments (antihistamine, antipyretics, and analgesics); no patient experienced anaphylaxis.
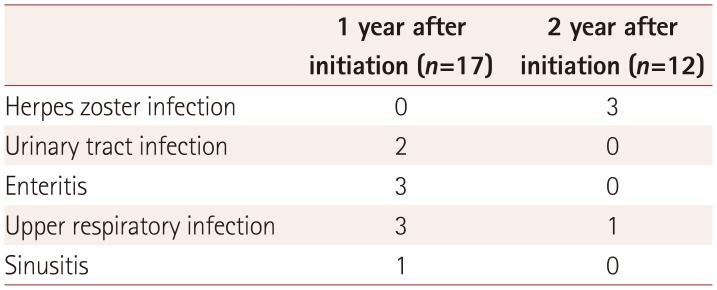
Ten (43%) of the 23 patients exhibited infection events during follow-up after initiating alemtuzumab. Three patients experienced herpes zoster infection at 20 months (two patients) or 22 months (one patient) after initiating alemtuzumab. All infection events were self-limiting, or were treated by antibiotics or antiviral agents; the details of these events are presented in Table 2.
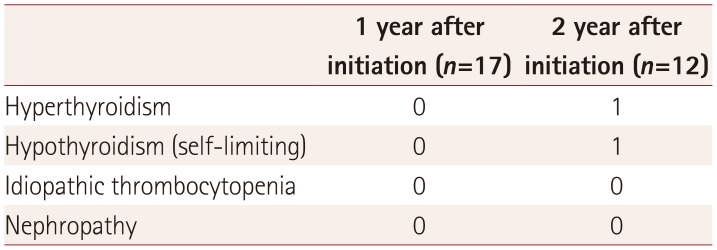
Two patients had thyroid dysfunction, one of whom required persistent medication during follow-up (Table 3). One patient experienced hyperthyroidism at 20 months after initiating alemtuzumab, and was treated with propylthiouracil until the last follow-up; the patient's free thyroxine level had normalized after 1 month of treatment. Another patient showed a high level of thyroid-stimulating hormone combined with a low free thyroxine level at 18 months after initiating alemtuzumab; however, this was self-limiting after 6 months without applying medication. No patient experienced other manifestations of secondary autoimmunity during follow-up, including hematological or renal involvement.
DISCUSSION
The administration of alemtuzumab to Korean patients with highly active MS significantly reduced the risk of clinical relapse, and the neurological disability score tended to improve during 2 years of follow-up. NEDA was observed in 4 (33%) of 12 patients; the proportion of patients with NEDA increased after the second course of alemtuzumab compared with after the first course, and reached 67% during the second year after initiating alemtuzumab. More than 80% of patients experienced IARs; however, all symptoms were manageable and no patient experienced a severe adverse event that required the discontinuation of alemtuzumab. All infection events were treatable and secondary autoimmunity developed only as thyroid dysfunction responsive to standard medication. Taken together, these results suggest that alemtuzumab is an efficacious and tolerable therapeutic option for Korean patients with highly active MS.
Patients with disease activity despite first-line DMTs might have a bad prognosis for neurological disability.171819 Timely escalation with potent DMTs is important for reducing clinical relapse and disability progression in these patients.2021 Prior to alemtuzumab being approved in Korea the only available second-line DMT was mitoxantrone, whose lifetime use is limited by its cumulative-dose-dependent cardiotoxicity.713 Alemtuzumab was approved for use as a second-line DMT in Korea at the end of 2015, and the current study has demonstrated that alemtuzumab provides a new opportunity to reduce disease activity and neurological disability accumulation in Korean patients with highly active MS.
Because all of the enrolled patients were treated with alemtuzumab as a second-line therapy in the current study, we compared the present findings with data from CARE-MS II clinical trial rather than those of CARE-MS I which enrolled only treatment-naïve patients.35 The proportions of patients with NEDA (33% vs. 32%) and improvement of disability (25% vs. 22%) in the current study were comparable with CARE-MS II data from primarily Western cohorts during 2 years of follow-up after initiating alemtuzumab.5 With respect to safety issues, the incidence of IARs in the present study was comparable to that in CARE-MS II56 and showed a similar pattern, decreasing from 74% to 63% after the second course of alemtuzumab (from 84% to 71% in CARE-MS II). Thyroid dysfunction as a manifestation of secondary autoimmunity was observed only during the second year after initiating alemtuzumab.56 The peak year of thyroid dysfunction was reported at year 3 following alemtuzumab in the previous study,6 longer-term observation is needed in our cohort.
A retrospective analysis has inherent methodological limitations, although routine laboratory tests (every 1 month), EDSS scores (every 3 months), and brain MRI scans (every 6 months) were evaluated prospectively at regular intervals to monitor the treatment effect and safety. Additionally, this study enrolled only a small number (n=23) of patients. However, considering the significant difference in the prevalence of MS between Western countries and Korea (67–350/100,000 persons vs. 3.5–3.6/100,000 persons), the enrolled patients could represent approximately 437 to 2,300 MS patients in Western populations.1222 We observed comparable efficacy and safety of alemtuzumab in Korean MS patients, which represents valuable real-world evidence for the use of a new potent and tolerable therapeutic option for active MS patients in Asian populations.
Notably, one patient showed a severe clinical relapse even after administering the second course of alemtuzumab, the therapeutic regimen was subsequently changed to natalizumab. Additionally, a third course of alemtuzumab was needed in three patients who exhibited mild-to-moderate disease activity after the second course of alemtuzumab. Observations of the therapeutic outcomes in these patients and patients without an additional DMT after the second course of alemtuzumab are ongoing. In the previous extension study, 55.5% of patients showed remission without a DMT over 3 years after the second course of alemtuzumab, and patients with disease activity received the third course of alemtuzumab and exhibited improved clinical/radiological outcomes with tolerable safety up to the 3-year follow-up.623 The disease course of MS can be quite heterogeneous, and personalized therapeutic approaches for individual patients are warranted. In the era of expanding therapeutic choices for patients with MS, physicians should have a comprehensive understanding of the benefit and risk profiles of each therapeutic option, and the benefit-to-risk balance should be favorably maintained to facilitate tailored therapeutic strategies for patients with MS.
In conclusion, alemtuzumab therapy in Korean patients with active MS reduced disease activity without uncontrolled safety concerns during 2 years of follow-up. An additional investigation is ongoing to assess the longer-term therapeutic outcomes of alemtuzumab therapy.
 XML Download
XML Download