

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Restless legs syndrome (RLS) is a common neurological disorder that is characterized by an urge to move the legs.1 Various previous studies have found that the prevalence of RLS in the general population is typically 5–15%,2 and can reportedly be as high as 45%.3 In a large epidemiological study in South Korea, 3.9% of the population fulfilled the criteria for RLS.4 The worldwide prevalence of RLS in Parkinson's disease (PD) patients was found to be 14–16%, but this was lower among East Asians, at 0.98–12%.56 However, a study in Korea reported on in 2013 found that the prevalence of RLS in drug-naïve PD patients was 16.5%.7 These previous findings indicate that the prevalence of RLS in PD patients is relatively high, and there might be a link between these two diseases since they both respond well to dopaminergic drugs. There have been various studies of the effects of RLS on PD, including motor symptoms,7 poor sleep quality, and quality of life (QoL),8 and the associations of RLS with autonomic functions.910
In this study we aimed to determine the frequency of RLS in PD, and identify various clinical characteristics including motor and nonmotor symptoms in PD patients with and without RLS. PD with RLS was compared to idiopathic RLS (iRLS). We also investigated the differences between RLS in PD patients and iRLS, and the response of RLS in PD patients to treatment with a dopamine agonist.
METHODS
This study was approved by the Institutional Review Board of Dongsan Medical Center (IRB No. 2014-04-051), and written informed consent was obtained from all patients enrolled in the study.
All of the patients with PD in this study were clinically diagnosed using criteria of the Brain Bank of the Parkinson's Disease Society of the United Kingdom and enrolled in a movement disorder clinic at a regional tertiary hospital from 2013 to 2017. Patients with Parkinson-plus syndrome, vascular parkinsonism, and secondary parkinsonism were excluded, as were patients with diseases that could cause other secondary RLS, such as iron-deficiency anemia, pregnancy, chronic renal disease, peripheral neuropathy, myelopathy, and medication-induced RLS. RLS was diagnosed through face-to-face interviews and examinations by a neurologist (YWC) who is an expert in RLS in order to exclude any mimicking diseases based on diagnostic criteria of the International Restless Legs Syndrome (IRLS) Study Group revised in 2003.1
When enrolling the patients after RLS diagnosis, motor symptoms of PD were assessed using the Unified Parkinson's Disease Rating Scale Part III (UPDRS-III), and the severity of PD was evaluated using the Hoehn and Yahr (H&Y) stage. Also, the levodopa equivalent dose (LED) was calculated in each treated PD patient. Nonmotor symptoms were evaluated using a battery of rating scales, including the Beck Anxiety Index (BAI), Beck Depression Index (BDI), Insomnia Severity Index (ISI), Parkinson's Disease Sleep Scale (PDSS), Pittsburgh Sleep Quality Index (PSQI), Scales for Outcomes in Parkinson's Disease for Autonomic Symptoms (SCOPA-AUT) for autonomic dysfunction, and Mini Mental State Examination (MMSE) for assessing cognitive impairment. Blood tests for hemoglobin, serum ferritin, iron, and total iron-binding capacity (TIBC) were performed simultaneously. In addition, the IRLS for RLS severity and an RLS-related QoL questionnaire were completed prior to starting RLS treatment.
The PD group was divided into those with RLS [PD-RLS (+)] and those without RLS [PD-RLS(−)]. When patients were enrolled into the PD-RLS(+) group in this study, they were asked about the onset timing between motor symptoms of PD and RLS, in terms of whether their RLS symptoms or their first symptoms of PD appeared first. Depending on the onset time of RLS, we divided PD-RLS(+) patients into two groups: those with RLS preceding PD onset and those with RLS after PD onset.
In addition, to compare PD-RLS(+) and iRLS we randomly selected age- and sex-matched iRLS patients from our hospital sleep-disorder database.
We observed how the RLS-related symptoms of patients diagnosed with RLS changed when adding adjustable dosages of a dopamine agonist (pramipexole) based on the clinical response at 2 weeks after the RLS diagnosis. The questionnaires on RLS severity, RLS-related QoL, depression, anxiety, sleep quality, and autonomic symptoms were reapplied after 2 weeks of administering pramipexole at 0.125 mg/day, and the scores were compared with those before treatment.
Statistical analyses were performed with SPSS Statistics (version 24.0, IBM Corp., Armonk, NY, USA). Probability values of p<0.05 were considered significant. Demographic variables, motor symptoms, nonmotor symptoms, levels of iron and related proteins in serum, and the results of sleep questionnaires were compared between PD-RLS(+) and PD-RLS(−). The independent t-test, chi-square test, and Fisher's exact test were used to compare the characteristics of patients in the PD-RLS(+) and PD-RLS(−) groups. The same methods were used to compare the PD-RLS(+) and iRLS groups. Pearson correlation analyses were performed between RLS severity and the clinical data of PD-RLS(+). Comparisons between before and after administering a dopamine agonist were performed in the PD-RLS(+) group using the paired t-test. The PD-RLS(+) group comprised 16 patients who conformed to a normal distribution according to a Kolmogorov-Smirnov test. After confirming the results of the tests, a parametric analysis was performed using the t-test.
RESULTS
The study enrolled 74 PD patients. The subjects were aged 65.5±9.1 years (mean±SD) and 30 (40.5%) of them were male. The age at PD onset was 63.0±9.7 years and the PD duration was 2.8±3.9 years. The UPDRS-III score was 24.0±12.2 and the H&Y stage was 2.1±0.7. Sixteen (21.6%) of the 74 subjects were diagnosed with RLS. The severity of RLS symptoms using the IRLS was 22.7±10.7.
Sixteen (21.6%) of the 74 PD patients were drug-naïve, with the remainder treated by dopaminergic drugs such as levodopa/aromatic L-amino acid decarboxylase inhibitor, monoamine oxidase-B inhibitor, and amantadine. Two (12.5%) of the drug-naïve PD patients were diagnosed with RLS, and 14 (24.1%) of the 58 patients who were already being treated were diagnosed with RLS (p=0.496).
Comparison of PD-RLS(+) and PD-RLS(−) groups
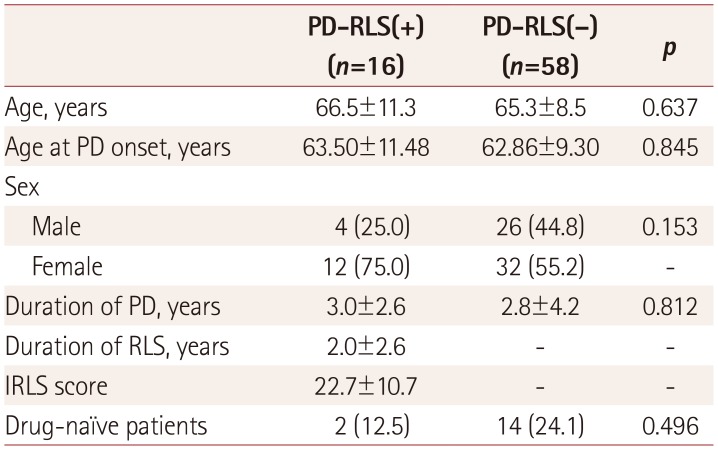
None of the demographic variables differed significantly between PD subjects with and without RLS (Table 1). The only significant intergroup difference was in the LED dose between naïve and treated patients (0 and 406.8±291.1 mg, respectively; p<0.001), as expected. The durations of PD and RLS were 3.0±2.6 and 2.0±2.6 years, respectively, in patients with RLS, and their IRLS score was 22.7±10.7.
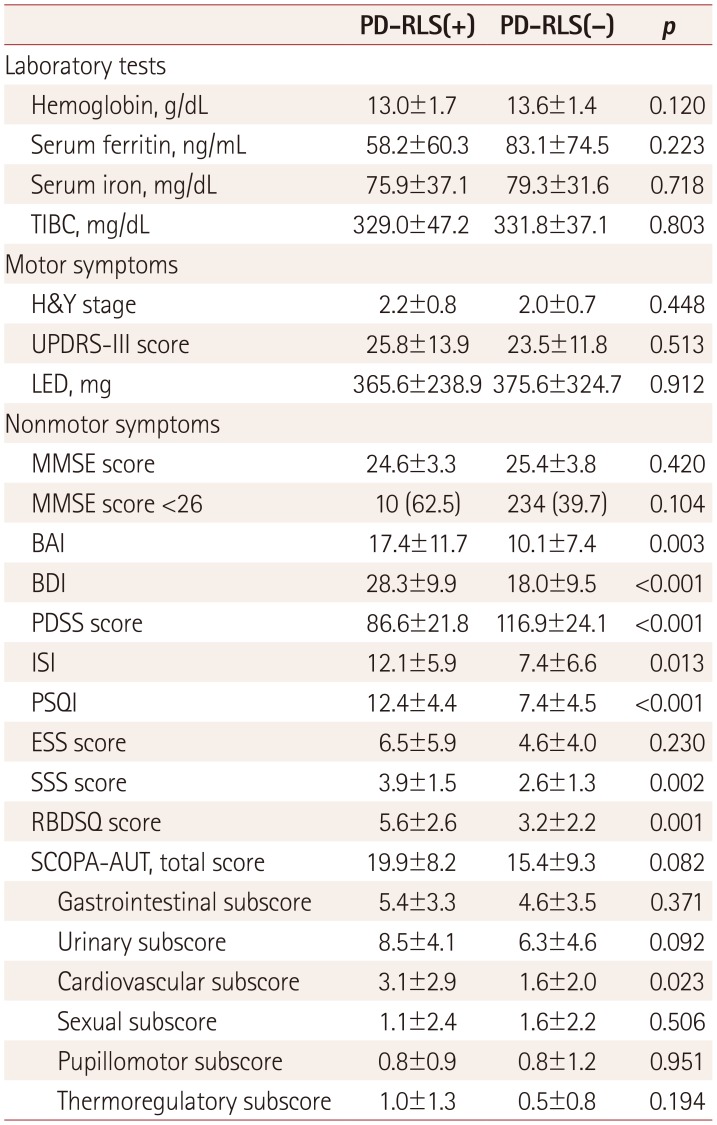
There were no statistically significant differences between PD-RLS(+) and PD-RLS(−) in terms of motor symptoms, disease duration, H&Y stage, UPDRS-III score, or LED (Table 2), or in serum iron, ferritin, or TIBC. Comparisons of nonmotor symptoms in indicated that the BAI, BDI, ISI, PSQI, and SCOPA-AUT score (cardiovascular subscore) were significantly higher in PD-RLS(+) than in PD-RLS(−). There was a particularly large difference in BDI between the PD-RLS(+) and PD-RLS(−) groups (28.3±9.9 vs. 18.0±9.5), indicating that depression was more severe in the latter. The PDSS score was significantly lower in PD-RLS(+) than in PD-RLS(−) (Table 2). However, the MMSE score did not differ significantly between PD-RLS(+) and PD-RLS(−) (Table 2).
Three (18.8%) of the 16 PD-RLS(+) patients experienced RLS symptoms prior to the onset of PD. Most of the demographic variables and clinical data did not differ significantly with the onset timing, with only the H&Y stage being significantly lower in RLS preceding PD onset than in RLS after PD onset (1.3±0.6 vs. 2.4±0.8, p=0.042).
Comparison of PD-RLS(+) and iRLS groups
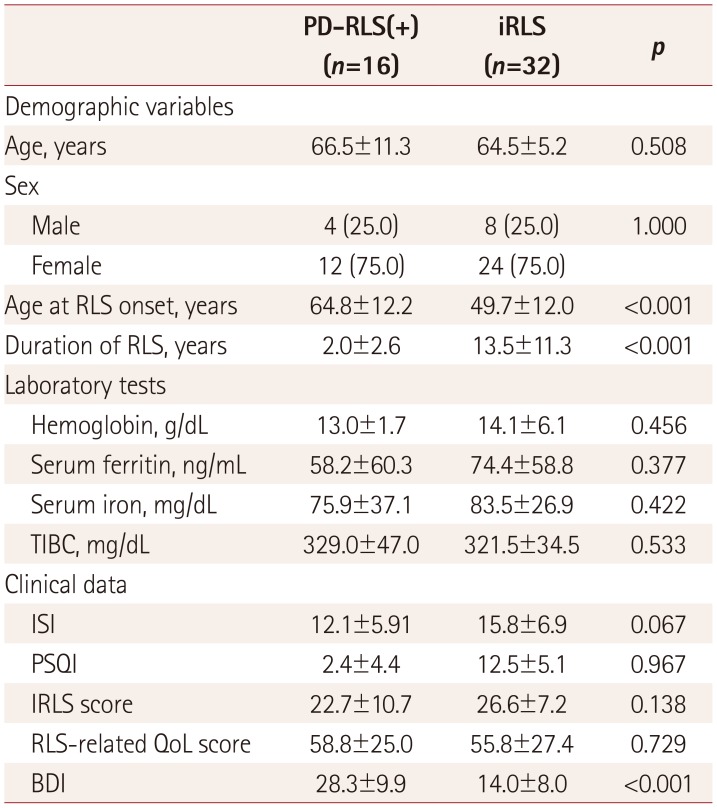
To compare PD-RLS(+) and iRLS, we reviewed data from 32 age- and sex-matched iRLS patients. Table 3 compares the demographic variables and clinical data between these two groups. The results from laboratory tests and for RLS severity, sleep quality, and anxiety did not differ significantly between the two groups. However, compared to PD-RLS(+), the iRLS group showed a significantly younger onset age, longer disease duration, and less-severe depression (p<0.001) (Table 3).
Correlation between RLS severity and clinical data in PD-RLS(+)
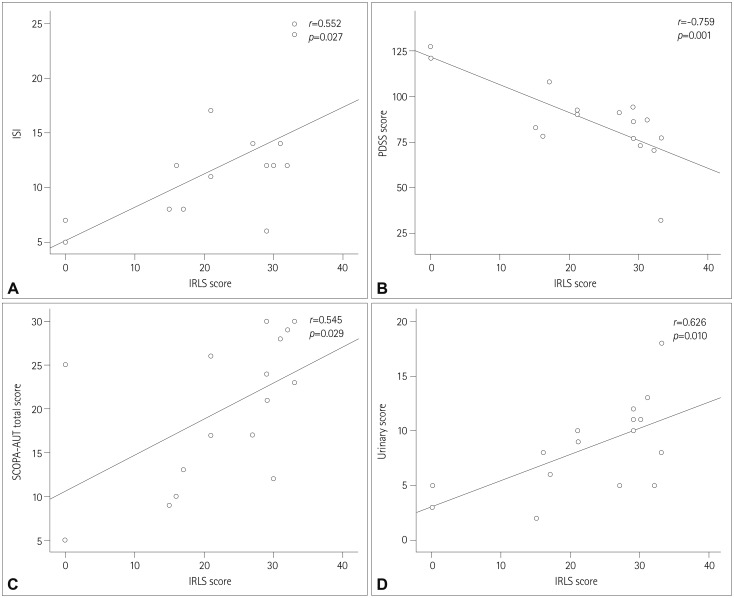
Correlation analyses revealed statistical significance only for the BDI and PDSS score with RLS severity. No association was found between RLS severity and parkinsonism based on the H&Y stage and scores for parkinsonism, which were significantly higher in patients with RLS. Significant correlations were found between the IRLS score and the PDSS score (r=−0.759, p=0.001), ISI (r=−0.552, p=0.027), SCOPA-AUT total score (r=0.545, p=0.029), and SCOPA-AUT urinary subscore (r=0.626, p=0.010) (Fig. 1). There were no correlations between IRLS scores and demographic variables, motor symptoms, and laboratory data.
Changes after dopamine-agonist treatment in PD-RLS(+)
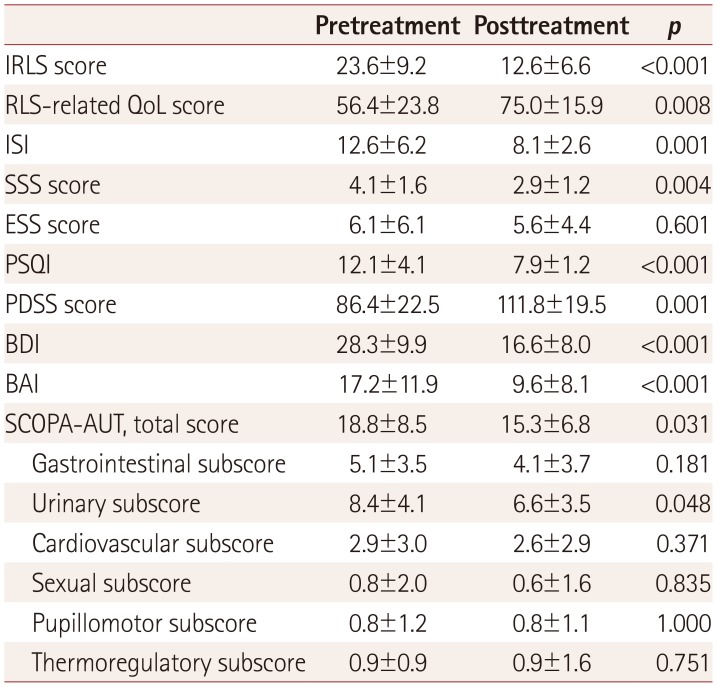
In 16 PD-RLS(+) patients, the RLS severity decreased significantly after the administration of the dopamine agonist pramipexole at 0.125–0.5 mg/day. In addition, RLS-related QoL, depression, anxiety, and sleep quality all improved, with significant improvements observed on the SCOPA-AUT scale (total score and urinary subscore) (Table 4). Motor symptoms did not change significantly between before and after dopamine-agonist treatment.
DISCUSSION
We observed that the frequency of RLS is higher in PD patients than in the general population. In addition, we found that PD-RLS(+) patients had worse nonmotor symptoms such as depression, anxiety, sleep quality, and autonomic dysfunction than did PD-RLS(−) patients. The severity of RLS was mainly related to sleep quality and autonomic dysfunction. It was also observed that the H&Y stage was lower in RLS preceding PD than in PD preceding RLS. PD-RLS(+) patients were older and had a shorter duration of RLS than did those with iRLS. In addition, RLS symptoms improved after dopamine-agonist administration in the PD-RLS(+) group, although this result was from a small sample (n=16).
The frequency of RLS in PD patients was markedly higher than in our previously published study involving the general Korean population (21.6% vs. 3.9%),4 and also higher than in a previous study of Koreans with PD (21.6% vs. 16.5%).7 The latter difference may have been due to the previous study targeting untreated PD patients while this study included both treated and untreated patients. A previous study in Western countries found that the prevalence of RLS was 21% in treated PD patients,11 while in this study it was 12.5% in the untreated group and 24.1% in the treated group. However, there was no difference in age, PD onset age, or duration of PD symptoms between the present treated and untreated groups. These observations suggest that the use of dopaminergic drugs is associated with the development of RLS symptoms. Lee et al.12 reported that a longer duration of dopaminergic treatment was related to the presence of RLS in PD patients. Also, RLS severity was found to improve with decreasing dopaminergic treatment after subthalamic nucleus deep-brain stimulation (STN-DBS).13 These factors suggest that overstimulation of dopamine receptors can cause RLS in PD patients.14
Comparisons of demographic variables revealed no significant differences in age, onset age of PD, sex, or disease duration between PD-RLS(+) and PD-RLS(−). These findings suggest that demographic variables are not related to RLS in PD patients. However, previous studies of PD-RLS(+) have found a younger age of PD onset and the predominance of males in Malaysia,15 an older age at the onset of PD in India,16 and a prolonged disease duration in China.10 These findings could have been due to selection bias of study samples, the smallness of the included samples, or race-specific genetic characteristics affecting the demographic variables of PD-RLS(+) patients. The H&Y stage and UPDRS-III score did not differ significantly between our PD-RLS(+) and PD-RLS(−) groups. Previous studies found RLS to be associated with PD motor symptoms, suggesting that both motor symptoms and RLS are associated with the dopaminergic system;71017 that is, the decrease in dopamine production with PD progression could lead to RLS aggravation.18
A possible reason for an absence of significant differences in motor symptoms in the present patients is that they had already been treated with dopaminergic drugs and were at H&Y stage 3 or lower, and thus their motor symptoms were not severe. While an H&Y stage of 3 or lower was not an inclusion criterion for this study, most of the subjects were early-stage PD patients.
The scores on the scales related to nonmotor symptoms were worse in PD-RLS(+) than in PD-RLS(−), showing more depression and anxiety, lower sleep quality, and more autonomic dysfunction, which has also been reported previously.9161920 Depression and anxiety are believed to result from decreases in dopamine and 5-hydroxytryptamine in the central nervous system contributing to poor sleep quality in PD-RLS(+). A previous study found that the levels of these two neurotransmitters in CSF were lower in PD-RLS(+) than in PD-RLS(−).10 Autonomic dysfunction in PD-RLS(+) may be a consequence of a lower cardiovascular subscore, which is believed to be associated with the A11 dopaminergic diencephalospinal pathway that innervates preganglionic sympathetic neurons and the dorsal horn in the spinal cord.21 Cognitive dysfunction in nonmotor symptoms was not observed in either group, suggesting that cognitive dysfunction is more closely related to acetylcholine than dopamine, and is mainly observed in the late phases of PD.10 Therefore, cognitive dysfunction was unlikely to be observed in the present study since the included patients were all in the early or middle stage of PD.
The serum iron, ferritin, and TIBC results did not differ between the PD-RLS(+) and PD-RLS(−) groups, which was similar to previous findings,72223 suggesting that iron metabolism is not affect by RLS in PD patients. However, a previous study found that PD-RLS(+) patients had reduced levels of iron and ferritin and an increased transferrin level in CSF compared to PD-RLS(−) patients.10 This may mean that measurements of iron and iron-related proteins in the peripheral system do to accurately reflect iron metabolism in the brain of PD-RLS(+) patients.
Previous studies comparing the characteristics of PD-RLS(+) and iRLS patients have shown that the onset age is younger in iRLS than in PD-RLS(+), RLS is more severe in iRLS, and that the two groups exhibit opposite seasonal patterns.172425 In addition, a family history of RLS is more common and the ferritin level is higher in iRLS than in PD-RLS(+).24 In our study the RLS onset age was younger and the RLS duration was longer in iRLS. However, serum ferritin levels and RLS severity were not significantly different between the two groups. These results are consistent with those of previous studies. Depression was more severe in PD-RLS(+) than in iRLS, which suggests that depression results from PD-related motor disability or other comorbidities, as well as RLS per se.26 Information on family histories and the seasonal patterns of RLS was not collected in the present study.
In the PD-RLS(+) group, depression, anxiety, QoL, sleep quality, and severity of RLS symptoms all improved after administering the dopamine agonist. Although the number of patients in the PD-RLS(+) group was small and there was no blinding for dopamine-agonist treatment and no control arm, it is possible that RLS in PD patients responds to dopamine agonists regardless of the conventional dopamine treatment. Of course, it is difficult to clearly determine whether this result was due to the dopamine agonist itself or the effect of increasing the LED. There is still no established treatment for RLS in PD patients. One previous study administered levodopa, dopamine agonists (ropinirole, pramipexole, and pergolide), opioid, and clonazepam to patients with RLS after STN-DBS.27 Another study showed that RLS that had developed during PD treatment improved after STN-DBS.28 There is a recent case report of safinamide being effective for RLS treatment in PD patients.29 However, more research is needed into how to treat RLS in PD.
Three (18.8%) of our 16 PD-RLS(+) patients had RLS before the onset of PD, which is a higher prevalence than in previous studies.10 Recent studies suggest that RLS is a nonmotor symptom that precedes PD motor symptoms.3031 Other studies have suggested that RLS slows the onset and progression of PD.3233 This explains why the H&Y stage was significantly lower in our group with RLS preceding PD onset than in the group where RLS occurred after the PD onset.
The limitations of this study include the inclusion of a relatively small number of patients from a single tertiary hospital, its cross-sectional design, and the heterogeneity of the patients due to dopaminergic treatment. We enrolled patients from an outpatient clinic of a tertiary hospital, and so patients with advanced motion limitations could not be enrolled due to attendance difficulties. It is possible that this enrollment procedure caused selection bias. In addition, the ability to detect effects of dopamine-agonist treatment in the PD-RLS(+) group would have been reduced by the smallness of the sample, the short treatment period, the lack of blinding, and the absence of a control arm.
In conclusion, in this study we found that the prevalence of RLS was higher in treated patients with PD than in our previously published study that involved a general Korean population, and that RLS had a negative effect on nonmotor symptoms. Depression was more severe in the PD-RLS(+) patients than in those with iRLS.
 XML Download
XML Download