

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The number of people with dementia is estimated to double every 20 years and will reach approximately 40 million worldwide by 2020 due to the increasing aging of the world's population.1 There are 9.9 million new cases of dementia each year,2 and so health care costs will increase exponentially over time.3 It has been hypothesized that if the onset of Alzheimer's disease (AD), the most common type of dementia, could be delayed in all patients by 2 years, the worldwide prevalence in 2050 might be 22 million lower than the current estimates, which would significantly reduce the associated costs.4 It is now well established that dementia includes a long phase of preclinical pathological changes that occur prior to the manifestation of clinical symptoms. Hence, it is necessary to identify modifiable factors and early interventions that can be a focus of therapy during these preclinical or prodromal stages of the disease.5
Numerous epidemiological studies have consistently suggested the presence of strong correlations among diet, lifestyle, and onset of dementia.6789 Malnutrition is defined as an inappropriate nutritional status characterized by poor appetite, insufficient dietary intake, weight loss, and muscle wasting.10 Malnutrition places older adults at increased risks of depression, infection, falls, and low psychological well-being.11 Elderly patients with dementia may suffer from malnutrition because they are often unable to eat independently and exhibit a reduced appetite.12 Unfortunately, the studies designed to confirm malnutrition as a modifiable risk factor for dementia have been restricted by the complexity of nutrition science,5 which indicates that there is a wide array of potential confounders that cannot be fully controlled when analyzing and designing studies related to nutrition.
This study used the Mini Nutritional Assessment (MNA) to assess the relationship between cognitive stage and nutritional status. We further examined differences in brain volume between a well-nourished group and an at-risk/malnutrition group to evaluate the relationship between malnutrition and cognitive change. Our hypothesis was that lower nutritional status is independently related to dementia, as well as to cerebral structural changes that might be associated with cognition.
Go to : 
METHODS
The data analyzed in this study were obtained from the Korean Brain Aging Study for the Early Diagnosis and Prediction of Alzheimer's Disease (KBASE). The KBASE is an ongoing prospective cohort study that started in 2014 and was designed to identify new biomarkers for AD and also AD-related structural and functional cerebral changes. The Institutional Review Board of Kangwon National University approved this study, which was performed in accordance with the tenets of the Declaration of Helsinki (approval number: KNUH-2015-04-009-005).
Participants
Participants were recruited from nine university hospital across South Korea. As of April 2017, 212 participants who were 55 years or older were initially enrolled in the study. Among the subjects, 119 were cognitively unimpaired (CU), 56 had mild cognitive impairment (MCI), and 37 had clinically diagnosed AD. All of the subjects underwent a comprehensive KBASE baseline assessment that included a clinical examination, neuropsychological tests, MRI, amyloid PET, and a blood test.
The CU group (aged 55–90 years) consisted of subjects with a global Clinical Rating Scale (CDR) score of 0 and without a diagnosis of MCI or dementia. Subjects with MCI (aged 55–90 years) met the following criteria: 1) memory complaint reported by themselves or by an informant or a clinician, 2) presence of objective memory impairment, 3) intact functional activities, and 4) no dementia. All MCI subjects had a global CDR score of 0.5. With respect to criterion 2), MCI individuals scored at least one SD below the respective age-, education-, and sex-specific mean values in at least one of the four memory tests that were part of the Consortium to Establish a Registry for Alzheimer's Disease (CERAD) neuropsychological battery (namely, Word List Memory, Word List Recall, Word List Recognition, and Constructional Recall tests).13 The following inclusion criteria were applied to patients with AD (aged 55–90 years): 1) meeting both the criteria of the Diagnostic and Statistical Manual, 4th Edition for dementia14 and the criteria for probable AD in the National Institute on Aging and Alzheimer's Association guidelines,15 and 2) having a global CDR score of 0.5 or 1. The exclusion criteria were 1) presence of any psychiatric or neurological disorders that could affect mental function, 2) severe communication problems that would made assessments or brain scans difficult, 3) contraindications for MRI scanning, 4) absence of a reliable informant, or 5) being illiterate.
Neuropsychological assessment
All participants underwent a standardized clinical assessment by a trained clinician based on the KBASE protocol, which corresponded with the Korean version of the CERAD-K assessment packet.16 In addition, participants underwent a KBASE neuropsychological assessment by trained neuropsychologists that included the CERAD neuropsychological battery,13 which contained the Mini Mental State Examination (MMSE).
Amyloid PET
Seventy-nine participants underwent simultaneous three-dimensional (3D) [11C] Pittsburgh Compound B (PiB) PET and 3D T1-weighted MRI using a 3.0-Tesla PET-MRI scanner (Siemens, Washington D.C., DC, USA). A 30-minute emission scan was performed 40 minutes after the intravenous administration of a mean of 555 MBq of [11C] PiB (range, 450–610 MBq). The PiB-PET data collected in list mode were processed for routine corrections such as uniformity, ultrashort echo time-based attenuation, and decay corrections, and were reconstructed into a 256×256 image matrix using iterative methods (6 iterations with 21 subsets). Amyloid PET scans using [18F]-flutemetamol were obtained in 131 subjects. These participants underwent a 20-minute emission scan at 90 minutes after the intravenous injection of 185 MBq of [18F]-flutemetamol. Low-dose CT was performed for attenuation correction before all scans. The images were reconstructed in a 256×256×109 matrix with a voxel size of 1.33×1.33×1.5 mm3 using a 2D ordered subset expectation maximization algorithm (8 iterations and 16 subsets), and they were corrected for physical effects including radiation attenuation and scatter.
The mean standardized uptake value ratio (SUVR) was determined for each subject by dividing the mean value for all voxels within the volume of interest (VOI) by the mean uptake value for cerebellar gray matter. β-amyloid (Aβ)-positive and Aβ-negative statuses were defined according to SUVR criteria of ≥1.4 for PiB PET and ≥0.634 for [18F]-flutemetamol PET. These criteria were taken from the KBASE database as the composite VOI SUVR with the highest accuracy for discriminating between CU subjects and patients with AD.
MRI acquisition, processing, and cortical thickness measurement
All of the participants were scanned using 3-Tesla MRI with protocols based on the Alzheimer's Disease Neuroimaging Initiative-2 MRI protocols. The 3D T1-weighted MRI scans were acquired from 212 participants with the following parameters: TR=7.32 ms, TE=3.02 ms, inversion time (TI)=400 ms, flip angle=11°, and a voxel resolution of 0.8×0.8×0.8 mm3 for the GE MRI device (GE Healthcare, Milwaukee, WI, USA); TR=shortest (6.8 ms), TE= shortest (3.1 ms), flip angle= 9°, and a voxel resolution of 0.8×0.8×0.8 mm3 for the Philips MRI device (Philips Healthcare, Andover, MA, USA); and TR=2,300 ms, TE=2.14 ms, TI=900 ms, flip angle=9°, and a voxel resolution of 0.8×0.8×0.8 mm3 for the Siemens MRI device.
Images were processed using the CIVET anatomical pipeline (version 2.1; http://mcin.ca/technology/civet/).17 The T1-weighted images in native space were aligned to the Montreal Neurological Institute 152 standard space.18 The N3 algorithm was used to correct for inhomogeneities caused by intensity nonuniformities of the magnetic field.19 Nonbrain tissue was excluded using the BET algorithm.20 The registered and corrected images were classified into gray matter, white matter, and cerebrospinal fluid using an advanced neural-net classifier.21 The inner surfaces of the cortex were extracted from a defined white-matter mask, and then the outer surface of the cortex was automatically extracted using the Constrained Laplacian-based Automated Segmentation with Proximities algorithm.22 The cortical thickness values were calculated in native space using the Euclidean distance between the linked vertices of the inner and outer surfaces. The thickness values in corresponding regions were compared between individuals using surface-based 2D registration with a sphere-to-sphere warping algorithm to spatially normalize the cortical thickness values.23 These values were subsequently smoothed using a surface-based diffusion kernel in order to increase the signal-to-noise ratio. We chose a 30-mm full-width at half-maximum kernel to maximize the statistical power while minimizing false positives.24 Finally, we divided the cortical surface into 78 regions with an automated anatomical labeling template excluding the cerebellum and subcortical regions,25 and calculated the regional cortical thickness values.
Laboratory tests for blood samples
Overnight fasting blood samples were collected in the morning by venipuncture. The baseline routine blood laboratory tests included in this study were of hemoglobin, albumin, and serum lipids. Genomic DNA was extracted from whole blood, and ApoE genotyping was performed as described previously.26
Assessment of nutritional and related-factors status
Nutritional status was measured using the MNA, which is widely used for evaluating the nutritional status of the elderly. This assessment method has been well validated internationally and has a high sensitivity, specificity, and reliability. The MNA consists of 18 questions, with the total MNA score ranging from 0 to 30, and a higher score indicating a better nutritional status. The total score was used to classify each patient into well nourished (MNA score >23.5), at risk of malnutrition (MNA score=17.0–23.5), or malnourished (MNA score <17).2728 Appetite was measured with the Simplified Nutritional Appetite Questionnaire (SNAQ) that was developed for a hospital outpatient population.29 The body mass index (BMI) was calculated for all subjects using their heights and weights.
Statistical analysis
Independent t-tests and chi-square tests were used to identify between-group differences in continuous variables and categorical variables, respectively. We examined the cross-sectional relation of being at risk of malnutrition or being malnourished to the clinical diagnosis using multiple logistic regression. The criterion for a variable being retained in multiple logistic regression was p<0.2 in the univariate analysis, and clinically important measures that were also included in the pool of predictors were age, sex, education level, MMSE score, Clinical Rating Scale Sum of Boxes (CDR-SOB) score, BMI, Geriatric Depression Scale (GDpS) score, SNAQ score, Aβ status, and hemoglobin level, as well as the final diagnosis. Multicollinearity among the covariates was tested by calculating the variance inflation factor.30
The criterion for statistical significance was set at p<0.05. Statistical analyses were performed with R software (version 3.3.2, 64-bit platform, The R Foundation for Statistical Computing; https://www.r-project.org/about.html). To identify differences in cortical thickness between groups, we first performed independent two-sample t-tests on a vertex-wise basis and in 78 regions of interest, with the age, sex, education level, SNAQ score, MMSE score, GDpS score, Aβ status, clinical diagnosis, and mean cortical thickness of the whole brain as covariates. To identify the brain regions that were correlated with clinical test results, we performed a partial correlation analysis between the regional cortical thickness and MNA score, with age, sex, education level, SNAQ score, MMSE score, GDpS score, Aβ status, and clinical diagnosis as covariates. These correlation analyses were performed using a surface model. The significance level for statistical analyses was thresholded at a false-discovery-rate-corrected p value of <0.0531.31
Go to :
RESULTS
The demographic and clinical characteristics of the cohort are listed in Table 1. The prevalence of malnutrition was 1.9% (n=4), while 30.7% (n=65) of the participants were at risk of malnutrition. Because the prevalence of malnutrition was very low, we grouped malnutrition and at risk of malnutrition into an at-risk/malnutrition group (n=69, 32.6%), and these participants were compared with those in the well-nourished group (n=143, 67.4%).
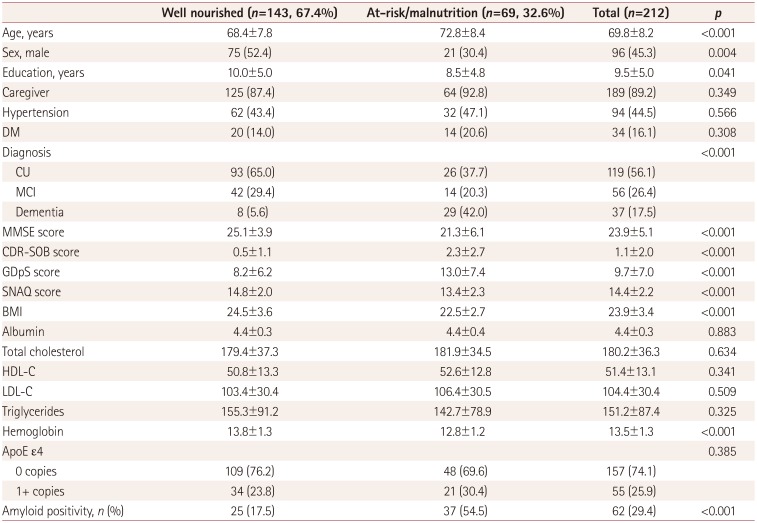
Table 1
Baseline characteristics of subjects according to the nutritional status
Data are mean±SD values except where indicated otherwise. Independent t-tests and chi-square tests were used to examine between-group differences in continuous variables and categorical variables, respectively.
BMI: body mass index, CDR-SOB: Clinical Rating Scale Sum of Boxes, CU: cognitively unimpaired, DM: diabetes mellitus, GDpS: Geriatric Depression Scale, HDL-C: high-density lipoprotein cholesterol, LDL-C: low-density lipoprotein cholesterol, MCI: mild cognitive impairment, MMSE: Mini Mental State Examination, SNAQ: Simplified Nutritional Appetite Questionnaire.
![]()
There were significant group differences in sex, age, and education level between the two groups. Participants in the atrisk/ malnutrition group were significantly older, more likely to be female, and had a lower education level than participants in the well-nourished group. The prevalence of dementia was significantly higher in the at-risk/malnutrition group than the well-nourished group (5.6% vs. 42.0%). The MMSE score, SNAQ score, BMI, and hemoglobin level were lower in the at-risk/malnutrition group, while the CDR-SOB and GDpS scores were higher. There was no significant difference in the frequency of the ApoE ε4 genotype; however, amyloid positivity in amyloid PET was more common in the atrisk/ malnutrition group. Among 62 subjects with amyloid positivity, 24 were positive in PiB PET and 38 were positive in [18F]-flutemetamol PET. In terms of clinical staging, amyloid positivity was observed in 14 (11.8%) subjects with CU, 19 (33.9%) subjects with MCI, and 30 (80.6%) subjects with dementia. There was no significant difference between the amyloid-positive and amyloid-negative dementia patients in the MNA score (21.36±3.39 vs. 23.21±2.63, mean±SD, p=0.187) or overall cortical thickness (2.96±0.17 vs. 2.96±0.11 mm, p=0.942).
The risk factors for at-risk/malnutrition, as assessed by multivariate logistic regression analysis, are presented in Table 2. The CDR-SOB score was statistically relevant, but its variance inflation factor was 3.088 and so it was excluded as a covariate. In the univariate analysis, participants with dementia showed a significantly increased odds ratio (OR) for at-risk/malnutrition of 12.52 (95% CI=5.31–32.54) compared with CU participants. Higher age and male sex were associated with at-risk/malnutrition, as were lower SNAQ and MMSE scores, higher GDpS score, and amyloid-positivity in PET.
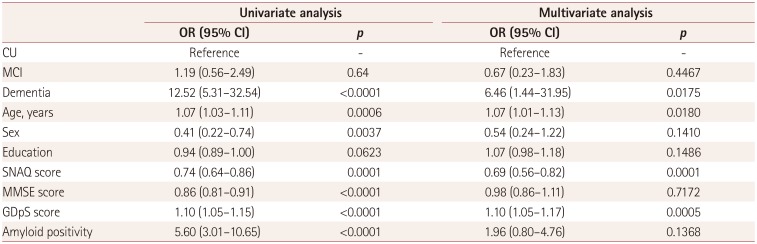
Table 2
Risk factors for being at risk of malnutrition or malnourished using univariate and multivariate logistic regression analyses
![]()
In multivariate analysis performed with the statistically relevant variables described above, dementia remained significantly associated with at risk/malnutrition (OR=6.46, 95% CI=1.44–31.95). There was no significant association between MCI and nutritional status, but there was a significant difference between subjects with MCI and subjects with dementia when MCI was used as a reference (OR=9.62, 95% CI=2.58–39.73). The significant independent risk predictors for at-risk/malnutrition also included age (OR=1.07, 95% CI=1.01–1.13), SNAQ score (OR=0.69, 95% CI=0.56–0.82), and GDpS score (OR=1.10, 95% CI=1.05–1.17).
Compared with the well-nourished group, participants in the at-risk/malnutrition group showed cortical thinning primarily in the left temporal area that included the left superior temporal gyrus, left temporal pole, and left insula after adjustment for age, sex, education level, SNAQ score, MMSE score, GDpS score, amyloid status, clinical diagnosis, and mean cortical thickness (uncorrected p<0.05) (Fig. 1). A significant negative correlation was observed between MNA score and cortical thickness in the temporal pole after adjustment for covariates (uncorrected p<0.05) (Fig. 2).
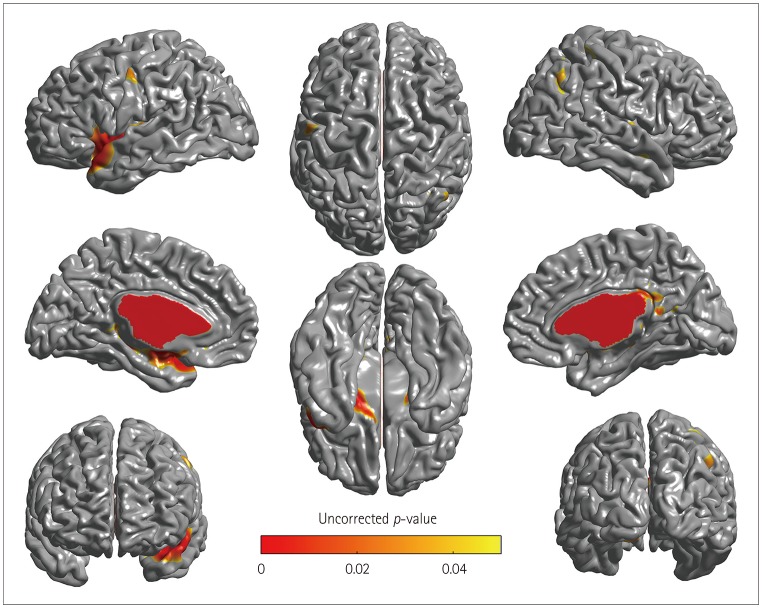 | Fig. 1Cortical thinning was associated with the risk of malnutrition in the Korean Brain Aging Study for the Early Diagnosis and Prediction of Alzheimer's Disease cohort. Regions with significant between-group differences in cortical thickness appeared in the left temporal area after adjustment for covariates. Clusters where the thickness was less in the at-risk/malnutrition group than in the well-nourished group are indicated in red.
|
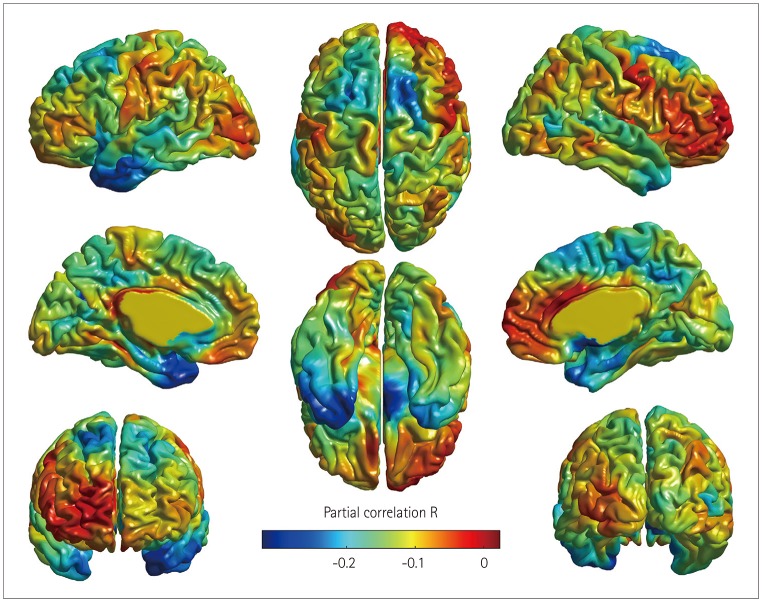 | Fig. 2Regions showing significant partial correlations between Mini Nutritional Assessment score and regional cortical thickness in the left temporal pole after adjustment for covariates. Clusters where the negative correlation was significantly stronger in all of the participants are indicated in blue.
|
Go to :
DISCUSSION
This study found a significant relationship between dementia and the risk of malnutrition after adjustment for other possible confounding factors. The risk of malnutrition differed significantly between subjects with MCI and those with dementia, but not between CU participants and those with MCI. In a comparison with other significant risk factors for malnutrition such as poor appetite, BMI, and depressive symptoms, the strongest risk factor was a diagnosis of dementia. In the present study, the prevalence of being at risk of malnutrition (MNA score ≤23.5) was 78.3% (29/37) among the participants with dementia (Table 1), which is consistent with previous studies that found high prevalence rates of malnutrition in newly diagnosed dementia patients, ranging from 26% to 80%.3233343536373839 Notably, 25% (14/56) of participants with MCI and 21.8% (26/119) of the CU participants exhibited a risk of malnutrition, and so we suspect that the nutritional imbalance associated with cognitive decline increases during the progression of dementia, rather than solely during the predementia stage. This assumption is partly consistent with a previous study finding that a longer disease duration of dementia was related to a higher frequency of being at risk of malnutrition.32 The presence of a live-in caregiver might be one of the most important factors influencing the nutritional status of elderly subjects, especially patients with dementia. However, we found no group differences with respect to caregiver status between the well-nourished and at-risk/malnutrition groups (Table 1). Additionally, the numbers of elderly subjects living alone in the present CU, MCI, and dementia groups were 9 (7.6%), 9 (16.1%), and 5 (13.5%), with no significant differences (p=0.204).
Regarding the association between dementia and malnutrition, a previous study suggested that the inability of many subjects with dementia to eat independently due to difficulties in swallowing, chewing, and recognizing hunger can result in malnutrition if aid is not provided by a caregiver.40 As dementia progresses in elderly individuals, a decreased food intake due to mealtime difficulties reduces their quality of life and physical health. In addition to the inability to eat satisfactorily, some studies have suggested that individuals with dementia experience weight loss that worsens with the progression of dementia.41 Moreover, subjects with dementia are more likely to be adversely affected by disabilities or comorbidities compared to subjects without dementia; this disparity can also lead to poor diet and malnutrition.42
Decreased appetite and BMI as well as depressive symptoms were also independently related to the nutritional status (Table 2). Among these factors, depression is the most common reversible cause of malnutrition43 and is more likely to be associated with weight loss and anorexia in older adults.4445 Depressive symptoms are frequently considered risk factors for a cognitive decline from MCI to dementia.4647 Given the relatively high prevalence of malnutrition and depressive symptoms among elderly subjects as well as the growing focus on preventable risk factors for dementia, future research should focus on the complex relationships among these factors.
Nutrition-associated atrophy was found predominantly in the left temporal area, indicating that the vulnerable areas were not distributed symmetrically. To the best of our knowledge, there have been no previous reports on reductions in cortical thickness related to undernutrition of elderly subjects, although a small number of studies have shown that eating a healthy diet (e.g., a Mediterranean-style diet) could increase the cortical thickness and improve cognitive function.48495051 Because the risk of malnutrition was found to differ significantly between subjects with and without dementia, we speculate that malnutrition could be associated with an increased risk of dementia, which is also partly supported by the nutrition-associated atrophy observed in this study. Enhancing the understanding of the neurobiological interactions between dementia and malnutrition requires longitudinal studies focusing on the causal relationship between cognitive decline and malnutrition, with consideration of both cerebral function and structure.
This study was subject to several limitations that should be considered when interpreting the findings. First, the study had a cross-sectional design, which reduced the ability to make causal inferences. Therefore, with regard to the relationship between dementia and risk of malnutrition, it was not possible to determine whether a nutritional imbalance caused dementia or the nutritional difference was a result of decreased intake secondary to cognitive decline. Second, a less stringent threshold for significance was adopted when determining the effect of undernutrition on cortical thickness in the surface model used in our study (p<0.05, uncorrected). Third, there was a low prevalence rate of malnutrition (MNA score <17), which might have reduced the intergroup difference in cortical thickness. Fourth, 7 of the 37 subjects with clinically diagnosed AD dementia were amyloid negative, which means that their dementia was unlikely to have been due to AD.52 Although, the nutritional index and mean cortical thickness did not differ significantly between amyloid-positive and amyloid-negative dementia, the ability to draw clear conclusions or perform further analyses was restricted by the small numbers of subjects. Lastly, nutritional status was categorized using the MNA questionnaire, which contains somewhat heterogeneous factors such as the activities of daily living. Therefore, detailed nutritional evaluation tools such as food-frequency questionnaires should be applied after screening by the MNA in the future in order to better address the complexity of nutritional science.
In conclusion, the nutritional status of the KBASE cohort suggested that dementia is an independent risk factor for being at risk of malnutrition. The structural changes in the left temporal region constitute additional evidence for a relationship with nutritional status. The nutritional status of patients with dementia needs to be evaluated to ensure that they have an optimal level of nutrition.
Go to :
 XML Download
XML Download