

 Citation
Citation Print
Print



INTRODUCTION
Anti-programmed cell death-1 (PD-1) antibodies nivolumab and pembrolizumab are immune checkpoint inhibitors that enhance immune response by inhibiting PD-1 receptors. PD-1 is a cell-surface receptor that is expressed on activated T cells; binding of its ligands downregulates T cells activation.1 Tumor cells express PD ligand-1 (PD-L1) to negatively regulate anti-tumor immune response and create an immune tolerance state; therefore anti-PD-1 therapy targets the PD-1/PD-L1 pathway and enhances T cell response. Anti-PD-1 therapies have been approved by the U.S. Food and Drug Administration (FDA) for treatment of several types of cancer, including metastatic melanoma, non-small cell lung cancer, kidney cancer, bladder cancer, head and neck cancers, and Hodgkin lymphoma. However, aberrant immune activation can lead to a spectrum of side effects such as hypothyroidism, gastrointestinal tract disorders, elevated aminotransferase levels, respiratory disorders and adverse skin conditions.2345
Due to the promising results reported for malignant tumors, more patients are expected to receive anti-PD-1 therapy in the near future. However, use of PD-1 inhibitors is a relatively new therapeutic strategy and there have been reports of cutaneous adverse events (AEs) associated with PD-1 inhibitors. Cutaneous AEs occur more frequently with the use of PD-1 inhibitors but are associated with less severe symptoms compared to treatment with anti-cytotoxic T-lymphocyte-associated protein-4 (CTLA-4) antibodies, another immune checkpoint inhibitor.678 Rash, pruritus and vitiligo are the most commonly reported cutaneous AEs.568910 Recently Sanlorenzo et al.10 also reported that cutaneous AEs were associated with longer progression-free intervals in patients with melanoma undergoing treatment with pembrolizumab.
In the future, we expect more cancer patients to be treated with anti-PD-1 therapy. It is important for dermatologists to recognize cutaneous AEs and their correlation with treatment response. We conducted a single-institution, retrospective study to describe the frequency and spectrum of cutaneous AEs in patients with various types of cancer. We also evaluated whether types of anti-PD-1 therapy or underlying tumor malignancies were associated with cutaneous AEs and investigated possible correlations of cutaneous AEs with treatment response in lung cancer patients.
METHODS
Patients
We reviewed records of patients from Asan Medical Center, Korea who received anti-PD-1 therapy (either nivolumab or pembrolizumab) as part of clinical trials or by FDA approved use between August 1, 2014 and April 1, 2017. Patients who received regimens combined with other therapies such as targeted therapy, chemotherapy, and radiation therapy and patients with concomitant exposure to anti-CTLA4 ipilimumab were excluded from this study.
We reviewed each patient's medical records and collected the following data: patient demographics, underlying malignancy, baseline Eastern Cooperative Oncology Group (ECOG) scale status, type of anti-PD-1 therapy and number of treatment cycles, cutaneous AEs attributed to anti-PD-1 therapy, and time to disease progression. For patients that exhibited cutaneous AEs, we collected information regarding onset timing of cutaneous AEs, treatment of cutaneous AEs, and grade of AEs based on the National Cancer Institute's Common Terminology Criteria for Adverse Events (version 4.03).
Statistical analysis
Statistical analysis was performed using SPSS, version 19 (IBM Corp, Armonk, NY, USA). Patients were classified into two groups: those with cutaneous AEs (group A) and those without (group B). To compare groups, Student's t-test, Pearson's χ2 test, or Fisher's exact test was used. Subgroup analysis evaluated the time to disease progression in patients with lung cancer. Time to progression was calculated from the first anti-PD-1 treatment cycle to progression. Kaplan-Meier survival curves were used to illustrate the time to event analysis and for comparisons between groups we used log-rank test. Cox proportional hazard regression analyses were carried out to test association between gender, age, ECOG score and time to progression. P < 0.05 was considered significant.
RESULTS
Patient characteristics
We included 211 patients in our study. The median age of patients was 61 years (range, 21–91 years). One hundred thirty-seven patients (65.9%) were men and 86 (35.1%) were women. The median treatment cycle was 7.0 cycles (range, 1–30 cycles). In total, 134 patients were treated with nivolumab (63.5%) and 77 with pembrolizumab (36.5%). Underlying malignancies treated were lung cancer in 106 patients (50.2%), renal cell carcinoma in 17 patients (8.1%), gastric cancer in 17 patients (8.1%), melanoma in 16 patients (7.6%), colorectal cancer in 16 patients (7.6%), bladder cancer in 13 patients (6.2%), hepatocellular carcinoma in 11 patients (5.2%), esophageal cancer in 9 patients (4.3%), oropharyngeal cancer in 4 patients (1.9%) prostate cancer in 1 patient (0.4%), and tonsillar cancer in 1 patient (0.4%). The mean number of treatment cycles was 4 (interquartile range, 2–10).
Cutaneous AEs
Of 211 patients, 35 (16.4%) developed cutaneous AEs. Characteristics of patient groupings were compared in Table 1. There were no significant differences between groups for age, gender, type of the anti-PD-1 therapy, underlying tumor malignancy, previous radiotherapy, and baseline ECOG scores. Patients with cutaneous AEs received longer treatment cycles compared to patients without cutaneous AEs (P = 0.001). Although there was no significant difference in underlying tumor malignancy between groups, cutaneous AEs were observed more frequently in patients with hepatocellular carcinoma (4 of 11 patients, 36.4%) and less frequently in patients with melanoma (1 of 16 patients, 6.3%).
Table 1
Comparison of characteristics of patients treated with anti-PD1 therapy
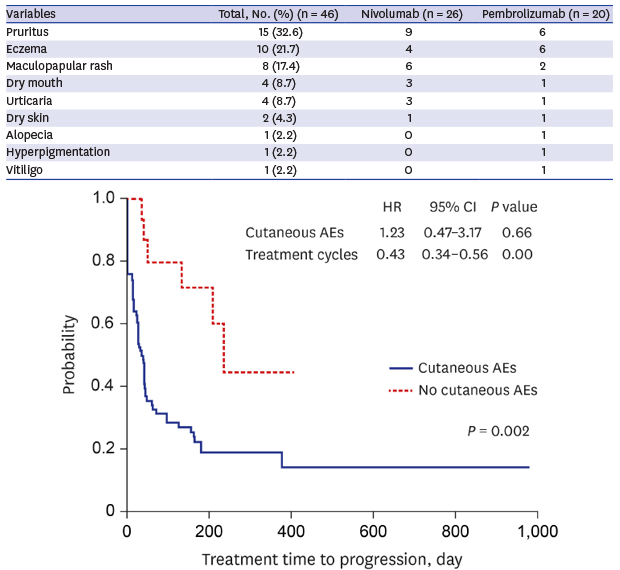
Forty-six anti-PD-1 therapy-related cutaneous AEs were recorded (Table 2). Six patients experienced two cutaneous AEs and one patient experienced four cutaneous AEs. Median time before the onset of cutaneous AEs was 50.0 days (range, 1–378 days). Median number of cycles before cutaneous AEs was 3 (range, 1–22 cycles). Median cumulative dose before the onset of cutaneous AEs was 590 mg (150–4,400 mg).
Table 2
Cutaneous adverse events of anti-PD1 therapy
Pruritus (n = 15, 32.6%) was most commonly reported followed by eczema (n = 10, 21.7%), and maculopapular rash (n = 8, 17.4%). Grade 1 cutaneous SEs were reported in 30 cases (65.2%) and grade 2 were reported in 11 cases (23.9%). One patient with lung cancer experienced grade 3 maculopapular rash 29 days after the start of treatment, with the eruption resolving after 3 days. One patient was treated with systemic corticosteroids (prednisone, 15 mg/day) for 10 days. Twenty patients (43.5%) received treatment for cutaneous AEs and 14 patients (30.8%) visited dermatologic clinics for skin examinations. No patient discontinued the anti-PD-1 therapy due to cutaneous AEs. Other systemic immune-related AEs were reported in 7 patients (20.0%) including pneumonitis in 5 patients and hypothyroidism in 2 patients.
The mean time of onset of pruritus was 55.0 days (range, 1–280 days) after anti-PD1 therapy; five patients reported grade 2 pruritus. Three patients reported improved condition with continued treatment while the others experienced no improvement. Median time of onset of eczema was 87.6 days (range, 2–280 days). Types of eczema present on patients included xerotic eczema (4 patients), seborrheic dermatitis (2 patients), systemic contact dermatitis (one patient), and unspecified eczema (one patient). Mean onset time of maculopapular rash was 86.9 days (range, 14–378 days) after anti-PD-1 therapy. Mild to moderate eruptions were treated with topical corticosteroids. Pigmentation abnormalities were reported in 2 patients treated with pembrolizumab. One patient treated for advanced gastric cancer reported hyperpigmentation 323 days after the onset of treatment, and one patient with bladder cancer reported vitiligo 324 days after the onset of treatment.
We grouped cutaneous AEs according to the antibodies used in anti-PD-1 therapy regimens. Hypopigmentation, hyperpigmentation, and alopecia were only reported in patients treated with pembrolizumab. There were no significant differences between treatments in type (P = 0.50) or grade of cutaneous AEs (P = 0.207). Timing of onset of cutaneous AEs was significantly longer in patients treated with pembrolizumab (mean ± standard deviation, 118.4 ± 124.9 days) compared to those treated with nivolumab (55.9 ± 53.9 days) (P = 0.047). Also, number of cycles before cutaneous AEs was significantly longer in patients with pembrolizumab (3, range 1–22 cycles) compared to patients with nivolumab (3, range 1–13 cycles) (P = 0.027).
Cutaneous AEs and disease progression
We examined records of lung cancer patients to investigate associations between cutaneous AEs and disease progression. Of 106 patients treated for lung cancer, 15 (14.2%) developed cutaneous AEs. There were no significant differences in age, gender, anti-PD-1 therapy type, or baseline ECOG between patients with and without cutaneous AEs. Patients with cutaneous AEs received a significantly higher number of treatment cycles (mean, 13.0 cycles) compared to patients without cutaneous AEs (mean, 6.1 cycles) (P = 0.009). Survival analysis revealed that patients with cutaneous AEs had significantly longer progression-free survival (PFS) (log rank test, P = 0.028); the hazard ratio was 0.291 (95% confidence interval [CI], 0.125-0.674; P = 0.004) (Fig 1). Results from a multivariate analysis associating longer PFS with cutaneous AEs in lung cancer patients were non-significant after applying a correction for the number of treatment cycles.
Fig. 1
Kaplan-Meier survival curves for progression-free survival. Cutaneous adverse effects did not associate with a longer progression free survival after corrected for number of treatment cycles by multivariate cox proportional hazard regression.
AE = adverse event, HR = hazard ratio, CI = confidence interval.
DISCUSSION
Nivolumab and pembrolizumab, anti-PD-1 antibodies, are relatively new drugs and little is known about associated cutaneous AEs. This study describes the characteristics of cutaneous AEs exhibited by cancer patients treated with PD-1 inhibitors. The overall incidence of cutaneous AEs seen in our study was 16.4% (17.2% in patients treated with nivolumab and 15.6% in those treated with pembrolizumab). A previous study relating the incidence of cutaneous AEs to anti-PD-1 therapy reported an incidence of nivolumab-related AEs of 14.3% (95% CI, 8.7%–22.7%) and pembrolizumab-related AEs of 16.7% (95% CI, 11.9%–23.0%), results similar to this study.9 Cutaneous AEs were not associated with type of anti-PD-1 therapy or characteristics of the patients such as age, gender and baseline ECOG status. Length of treatment cycle was positively associated with the cutaneous AEs; people with longer treatment durations were more likely to have side effects. Mean latency periods of cutaneous AEs in our study were relatively long (about 2 months for pruritus and 3 months for eczema and maculopapular rash).
In this study, we found no significant differences in the incidence of cutaneous AEs relating to underlying tumor malignancy. Pooled incidences of cutaneous AEs from pivotal clinical studies were 17.3% in squamous non-small cell lung cancer patients treated with nivolumab, 39.5% in melanoma patients treated with nivolumab and 42.0%–46.3% in melanoma patients treated with pembrolizumab.510 Previous studies of melanoma trials performed by dermatologists have shown that the incidence of cutaneous AEs was higher than in other cancer trials.5710 Cutaneous AEs were the most frequently reported AEs in anti-PD-1 therapy but ‘severe skin reactions’ of grade ≥ 3 AEs were seen in only 0.01%–1.7% patients.58910 This difference of incidence rates of cutaneous AEs among studies might be explained by reporting effects. Investigators who are not dermatologists may not recognize mild cutaneous AEs. In our study, cutaneous AEs were most common in HCC patients (4 of 7 patients, 36.4%) followed by lung cancer patients (15 of 91, 14.2%). Only one of 15 patients (6.3%) with melanoma reported cutaneous AEs. Further studies will be needed to determine whether the incidence of cutaneous AEs in melanomas in our study is accurate or low due to reporting bias.
Pruritus (32.6%) was the most common cutaneous AE in our study, followed by eczema (21.7%) and maculopapular rash (17.4%). These three AEs account for more than two thirds of the total cutaneous AEs seen in our study. Pruritus (12.0%–36.1%) and maculopapular rash (12.1%–29%) were also commonly reported in other studies. However, in a dermatologist-led study, Hwang et al.7 reported types of cutaneous SEs different from those seen in our study. The most frequent cutaneous AEs in the dermatologist-led study were lichenoid reaction (17%), eczema (17%), and vitiligo (15%). Lichenoid drug eruption in response to anti-PD-1 therapy is becoming well recognized. The reaction is mediated by lymphocyte damage of basal keratinocytes and grouped as immune-related AEs.1112131415 Lichenoid drug eruption is characterized by flat-topped erythematous or violaceous papules, often grouped and confluent on the trunk and extremities and histologically show an interface dermatitis. In our study lichenoid eruptions may have been misdiagnosed and grouped as “maculopapular rash” or “eczema.” The mean latency period between drug initiation and onset of skin eruptions was approximately 3 months for both maculopapular rash and eczema in our study, timing similar to onset of lichenoid drug eruption which varies from months to a year or more. To diagnose a lichenoid drug eruption, a detailed skin examination by a dermatologist coupled with a skin biopsy are required.
Abnormalities in pigmentation were reported in two patients treated with pembrolizumab. Hyperpigmentation was reported in a patient treated for advanced gastric cancer and vitiligo was reported in a patient treated for bladder cancer. Vitiligo, another immune-related cutaneous AE, was reported in 8.0%–30.2% of melanoma patients treated with PD-1 antibodies.7810 Vitiligo has been recognized to occur in melanoma patients during treatment,16 resulting from breakdown of immune tolerance as cancer treatment releases melanocyte-associated antigens.17 Our study was the first to report vitiligo in a non-melanoma patient treated with PD-1 antibodies and suggests different mechanisms are involved in pigment abnormalities in patients treated with anti-PD-1 therapy. PD-L1 is known to be expressed by melanocytes and melanocytic nevi,1819 and anti-PD-1 therapy may affect dysregulation of melanocyte function causing hypo- or hyperpigmentation. Wolner et al.20 reported the disappearance of pigmented skin lesions including nevi, seborrheic keratoses and solar lentigines following pembrolizumab treatment for melanoma.
The prognostic value of cutaneous AEs as a marker for treatment response is currently unclear. In a large meta-analysis, vitiligo was significantly associated with progression-free survival (PFS) and overall survival in melanoma patients receiving immunotherapy.21 Recently, a study reported that cutaneous AEs were associated with better outcomes among patients treated with pembrolizumab, after correcting for the number of treatment cycles.10 Patients in the above-mentioned study had a variety of cancers, including melanoma, lung cancer, prostate cancer and Merkel cell carcinoma. However, in our study, cutaneous AEs were not associated with better outcomes in patients with lung cancer after correcting for the number of treatment cycles. This can be explained by the fact that patients who respond to anti-PD-1 therapy often have longer treatment cycles and have more time to develop cutaneous AEs compared to those patients who do not respond to therapy. Moreover, cutaneous AEs include autoimmune toxic effects as well as various types of skin reactions. Further investigation will be needed to establish whether a correlation exists between the occurrence of specific immune-related cutaneous AEs such as lichenoid drug eruption and the antitumor responses of PD-1 antibodies.
Our study has certain limitations. It is a retrospective cohort study with a heterogeneous group of patients exhibiting various underlying tumor malignancies. Also, conducted by a single-center, there are limitations to generalization. Only 14 patients (30.8%) with cutaneous AEs visited the dermatology clinic, suggesting cutaneous AEs rates in the study could be lower than expected and detailed diagnosis of cutaneous AEs were not available. Finally, the median overall survival data and long-term prognostic value of using cutaneous AEs as a marker for treatment response could not be determined based on the relatively short follow-up period of the study.
In conclusion, our study described the spectrum of cutaneous AEs of either nivolumab or pembrolizumab in 211 patients. Anti-PD-1 therapy showed a favorable cutaneous safety profile in variable underlying malignancies. Prevalence of cutaneous AEs did not differ by the type of anti-PD-1 therapy, underlying tumor malignancy or patient characteristics. Pruritus, eczema, and maculopapular rash was common in patients undergoing anti-PD-1 therapy and appeared late in treatment. Long-term and regular evaluation of a dermatologist during anti-PD-1 therapy is important to properly diagnose and manage cutaneous AEs. The development of cutaneous AEs in patients with lung cancer was not associated with better clinical outcomes and additional studies searching for biomarkers to predict response to anti-PD-1 therapy are needed.
 XML Download
XML Download