

 Citation
Citation Print
Print



INTRODUCTION
Pediatric constipation is commonly encountered by medical practitioners.1 Approximately 3% of children who visited a pediatric clinic have constipation, and 25% of these children are referred to pediatric gastroenterology clinics.2 A study from a tertiary center for pediatric gastroenterology in the Netherlands showed an even higher rate (45%) of consults were due to defecation disorders.3 The symptoms of pediatric constipation can decrease the quality of life and negatively affect childhood development.13
The majority of children with constipation do not have an underlying medical disease.4 The ROME III criteria, which defined and presented the diagnostic criteria for pediatric functional constipation (FC), was updated in 2016 to the ROME IV criteria; this update decreased the duration of symptoms from 2 months to 1 month for children aged ≥ 4 years.5
We distributed a questionnaire throughout Korea to investigate the real-world practice patterns of pediatricians for FC. In addition, we compared the differences in clinical practice between general pediatricians and pediatric gastroenterologists (PGs).
METHODS
A total of 239 out of 500 (47.8%) members of the Korean Society of Pediatric Gastroenterology, Hepatology, and Nutrition (KSPGHAN) responded to the questionnaire. The study population was pediatricians who manage children with FC aged 0–18 years.
The survey was anonymized and conducted for one week using an online mobile phone application. The survey had 40 questions that took an average of 12 minutes to complete on the following subjects. It had been modified after a pilot study. The awareness and application of the definition for pediatric FC, use of various diagnostic methods, management duration and follow-up patterns, rate of relapse, and pharmacologic and non-pharmacologic treatment. We used the definition of FC from ROME IV criteria that required ≥ 2 of the following symptoms or signs without organic cause: ≤ 2 defecations per week, ≥ 1 episode of incontinence per week, history of excessive stool retention, history of painful or hard bowel movements, presence of a large fecal mass in the rectum, and history of large-diameter stools that could obstruct the toilet. In addition, the duration of symptoms should be ≥ 1 month.67 We collected information whether they perform perianal examination, digital rectal examination (DRE), imaging studies and laboratory investigation. We collected information on disimpaction practices, and pharmacologic and non-pharmacologic treatments. The treatments were divided into two groups: age ≥ 1-year and age < 1-year. In the age ≥ 1-year group, we included the medications polyethylene glycogen (PEG) 4000, PEG 3350, lactulose, magnesium, lactitol, and probiotics. In the age < 1-year group, we included formula changes, PEG 4000, PEG 3350, lactulose, and probiotics. We asked about diet modification, toilet training, defecation diaries, and multidisciplinary approaches that included dieticians and pediatric psychologists. In addition, we asked about the treatment methods for encopresis.
We assessed the clinical practice patterns for pediatric FC, and we assessed if there were differences between PGs and general pediatricians.
Descriptive statistics for continuous variables were reported as the mean ± standard deviation, and categorical variables were reported using counts and percentages. The χ2 test, Fisher's exact test, or Student's t-test were used to investigate the significance of differences between the PGs and general pediatricians, as appropriate for the data type. A P value < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 20.0.1 (SPSS Inc, Chicago, IL, USA).
Ethics statement
The Institutional Review Board (IRB) of the Korea University Guro Hospital approved this study (2018GR0272). Participants were informed of the purpose of medical research in the preface of the online questionnaire. Informed consent was implied by voluntarily participating in the survey after being informed of the purpose of the study. Written consent was waived under IRB's approval.
RESULTS
Characteristics of participants
A total of 46.9% of the KSPGHAN members who answered the questionnaire worked in the Seoul and Gyeonggi province metropolitan areas; the distribution was consistent with the national population distribution (43.3% live in metropolitan areas) (Fig. 1). Our study's participants included 60 (25.1%) PGs, who represented 75% of the total nationwide PGs. The characteristics of participants were described in Table 1.
 | Fig. 1Distribution of participants for the nationwide survey for functional constipation in children.
|
Table 1
Characteristics of participants

![]()
Awareness and application of ROME IV criteria on pediatric functional constipation
The pediatricians were asked to indicate the symptom duration specified in the ROME IV criteria for FC, and the most common answers were as follows: ≥ 1 month (90/205, 37.7%), ≥ 2 months (88/205, 36.8%), and ≥ 2 weeks (27/205, 11.3%). For the diagnostic clinical symptoms or signs of FC, 79.3% (46/58) of PGs answered ≤ 2 defecations per week compared to 54.4% (80/147) of general pediatricians (P = 0.001), and general pediatricians more commonly chose ≤ 1 defecation per week (52/147, 35.4%). A total of 53.9% of participants correctly answered that ≥ 2 of the six symptoms and signs of constipation in the ROME IV criteria are needed for a diagnosis of FC. Overall, 16.6% (34/205) of participants were aware of the ROME IV criteria, which are a symptom duration of ≥ 1 month, ≤ 2 defecations per week, and the presence of ≥ 2 of the six symptoms or signs of constipation. The PGs had a higher percentage of correct answers than the general pediatricians (31.0% vs. 10.9%), but the difference was not statistically significant.
The number of respondents who correctly identified the symptoms and signs of the ROME IV criteria in clinics were as follows: Hard stool or toilet obstruction (195/205, 81.6%), ≤ 2 defecations per week (170/205, 71.1%), fecal incontinence (152/205, 63.6%), painful or hard bowel movement (145/205, 60.7%), excessive stool retention (144/205, 60.3%), and presence of a large fecal mass in the rectum (105/205, 43.9%).
Physical examination and diagnostic evaluations
Perianal examination and DRE were performed by 63.9% (131/205) and 81.5% (167/205) of respondents, respectively; PGs had a higher tendency to practice perianal examination and DRE than general pediatricians (P < 0.001). The primary reason given for the avoidance of physical examinations was patient discomfort (54.2%), and 30.9% of respondents did not perform a DRE when a diagnosis of FC could be obtained by the patient’s medical history. In general, a diagnostic evaluation was not performed, except for suspected organic disease (140/205, 68.3%). The respondents most commonly performed a simple X-ray, followed by blood analysis, a colon study, computerized transmission tomography, and ultrasonography.
Managements
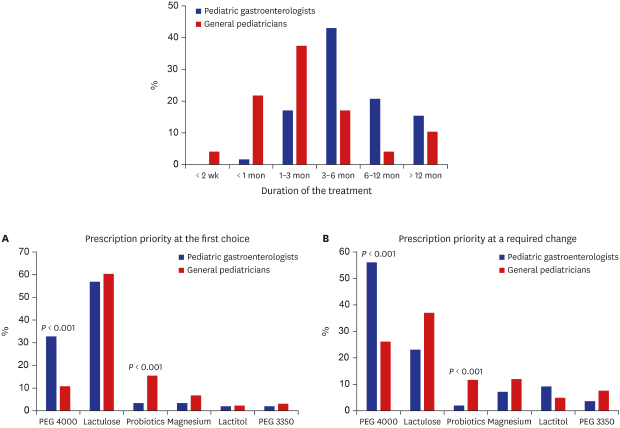
The most common treatment duration among the respondents was 3–6 months (128/205, 57.6%), followed by 1 month (33/205, 16.1%) and ≥ 12 months (24/205, 11.7%). A total of 63.8% (37/58) of the PGs treat children with FC for more than 6 months (37/58, 63.8%), and 59.2% (87/205) of the general pediatricians less than 3 months. The difference in treatment duration between the PGs and general pediatricians was significant (P < 0.001) (Fig. 2). The initial phase of treatment among the respondents was 3.87 ± 2.39 weeks (range, 1–24 weeks). The follow-up interval during the initial treatment among the respondents was 1.57 ± 0.96 weeks (range, 1–8 weeks). The follow-up interval during the maintenance treatment among the respondents was 4.36 ± 2.56 weeks (range, 1–12 weeks).
 | Fig. 2The difference in the treatment duration between PGs and general pediatricians. The treatment duration was significantly different between PGs and general pediatricians (P < 0.001).PGs = pediatric gastroenterologists.
|
Fecal disimpaction was performed by 78.8% (167/205) of respondents, primarily with a rectal enema (120/205, 59.1%). A high-dose medication was prescribed in the initial treatment phase by 70.7% (145/205) of respondents, primarily within the first 2 weeks (99/205, 48.3%).
We asked participants to choose the priority in prescriptions for maintenance treatment in children aged ≥ 1-year. The respondents ranked their prescriptions as the first as follows: Lactulose (59.1%), PEG 4000 (17.7%), probiotics (11.8%), magnesium (5.9%), PEG 3350 (2.7%), and lactitol (2.2%) (Table 2). The reasons given by respondents for the priority were the following: treatment effect, patient’s compliance, and cost of medication, with 66.7%, 25.3%, and 8.1% as the first reason, respectively.
Table 2
The priority in prescriptions for maintenance treatment (rank from 1st to the 6th) in children with functional constipation aged ≥ 1 year

![]()
A required change to a patient’s treatment regimen altered the rank of prescriptions by the respondents to the following: PEG 4000 (35.8%), lactulose (32.8%), magnesium (10.4%), probiotics (8.6%), lactitol (6.4%), and PEG 3350 (6.4%) (Table 3). The reasons given by respondents for changing treatment were the following: poor response, poor patient compliance, and cost of medication, with 78.4%, 23.5%, and 1.9% as the first reason, respectively.
Table 3
The priority in prescriptions in cases of a required change to a patient’s treatment regimen (rank from 1st to the 6th) in children with functional constipation aged ≥ 1 year

![]()
For patients aged < 1-year, the prescription priority among respondents showed that lactulose was most commonly prescribed (72/173, 41.6%), followed by formula changes (55/173, 31.7%), probiotics (39/173, 22.5%), and PEG 4000 (7/173, 4.0%). In the 2nd prescription priority, probiotics were the most common (50/173, 28.9%), followed by lactulose (46/173, 26.5%), formula changes (37/173, 21.3%), PEG 4000 (25/173, 14.4%), and lactitol (2/173, 1.1%).
The most commonly prescribed medications were lactulose and PEG 4000 among PGs (52/58, 89.7%), and lactulose and probiotics among general pediatricians (97/128, 75.7%; P < 0.001). For patients with FC aged ≥ 1-year, PGs prescribed PEG 4000 more frequently than general pediatricians (P < 0.001), and general pediatricians prescribed probiotics more frequently than PGs (P < 0.001) (Fig. 3). For patients with FC aged < 1-year, PGs prescribed lactulose more frequently than general pediatricians (P = 0.035), and general pediatricians prescribed probiotics more frequently than PGs (P < 0.001). In infants, PGs preferred to use lactulose or change formula, and general pediatricians preferred to use probiotics.
 | Fig. 3The pharmacologic treatment in children aged ≥ 1 year with functional constipation and the difference in prescription priority between PGs and general pediatricians; (A) at the first choice for maintenance, and (B) at a required change to a patient's regimen. There was a significant difference in prescription priority between PGs and general pediatricians for PEG 4000 and probiotics (P < 0.001).
|
A total of 59.6% (102/171) of the respondents used defecation diaries; and 60.8% (104/171) educational brochures in < 25% of their patients. The defecation diary was used more frequently among PGs than general pediatricians (P = 0.002). A total of 89.0% of respondents provided education on toilet training, with 59.0% providing a detailed method. More than half of the respondents answered that they worked with a dietician (144/171, 84.2%) and pediatric psychiatrist (159/171, 93.0%) in < 25% of their patients. A total of 59.6% of respondents recommended diet modification with importance of > 50% (among a 5-point scale; score 1, no recommendation, to score 5, recommend with importance of 75%–100%). The recommendations of increased fluid, dietary fiber, and prune, apple, or pear juice with importance of ≥ 50% were answered in 40.4%, 59.1%, and 40% of respondents, respectively. The respondents answered that they never restrict dairy products, banana or persimmon, or instant food in 36.8%, 28.1%, and 28.2%, respectively.
Pharmacologic treatment for encopresis (128/171, 74.8%) was the most common, followed by toilet training (111/171, 64.9%), diet modification (89/171, 52.0%), behavioral treatment (62/171, 36.2%), and biofeedback (15/171, 8.7%).
Most respondents (140/205, 68.3%) answered that they experienced relapse in 10%–50% of their patients. Overall, 58.4% of the participants got their information about FC from an academic seminar, and 58.4% of participants answered that they did not get enough information about FC.
DISCUSSION
We found discrepancies in our study between actual practice and the ROME IV criteria, and between PGs and general pediatricians. To become a PG in Korea, a pediatrician must have specific training and clinical experience and pass a license examination.
A previous study reported that less than half of the surveyed pediatricians in the Mediterranean area used the ROME criteria for functional gastrointestinal disorders; in addition, most pediatricians were using the symptoms reported by parents to diagnose FC, and those who were aware of the ROME criteria (40%) were primarily using the ROME II or III criteria.8 In our study, many pediatricians are applying their own clinical experience to diagnose childhood FC rather than implementing updated international consensus (ROME criteria) in everyday practice. General pediatricians more commonly chose ≤ 1 defecation per week as a diagnostic criterion for FC than PGs, which suggests that the diagnosis and treatment of pediatric FC may be delayed in a primary-care setting.
The Rome Foundation Working Team reported a deficiency in the knowledge and use of the ROME criteria, especially among general practitioners.9 Borowitz et al.10 reported that American primary-care pediatricians had a lack of familiarity with the ROME criteria. Koppen et al.11 reported that approximately one third of their surveyed respondents were unfamiliar with the ROME criteria, and this unfamiliarity was more common among general pediatricians and physicians from the United States than those from the Netherlands.
The diagnosis of pediatric FC is based on a “positive” approach that avoids unnecessary tests to rule out an organic cause.1213 Scarpato et al.8 reported that 42% of pediatricians considered FC a diagnosis of exclusion that was reached after a thorough diagnostic evaluation for other etiologies. The 2014 European Society for Pediatric Gastroenterology, Hepatology, and Nutrition and North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN/NASPGHAN) joint guideline for FC in children recommends that a patient's history and a physical examination should be used for diagnosis rather than routine tests in the absence of severe symptoms.1 In this study, most respondents answered that they did not perform diagnostic evaluations unless an organic disease was suspected.
The Rome criteria and 2014 ESPGHAN/NASPGHAN guideline recommend DRE when a diagnosis of FC is uncertain,1 because it helps clinicians discriminate FC from other organic diseases and functional non-retentive fecal incontinence.167 However, several studies have shown that DRE is often avoided in clinical practice, with 43%–61% of practitioners either never or only occasionally performing the procedure,8111415 and these results are similar to our findings.
The 2014 ESPGHAN/NASPGHAN guideline states that PEG and rectal enemas are equally effective for fecal disimpaction in FC treatment.1 Bekkali et al.16 reported no difference between the effectiveness of an enema and that of high-dose oral PEG for fecal disimpaction. The working-group guideline prefers PEG for fecal disimpaction, because it is an oral agent.1 A recent study showed that the majority of respondents (67.4%) performed fecal disimpaction,17 and others reported frequencies at 20% and 47%, respectively.1018 In our study, fecal disimpaction was performed by 78.8% of respondents, primarily using rectal enemas (59.1%) and PEG (15.3%). A study in the Netherlands and United States reported that the majority of responders used PEG for fecal disimpaction.11 Widodo et al.19 reported that pediatricians preferred lactulose over rectal enemas for fecal disimpaction. We found that fecal disimpaction was frequently performed before the maintenance treatment, and the specific methods used were based on the clinician's personal choice and regional culture, instead of the international consensus or current guidelines.
The 2014 ESPGHAN/NASPGHAN guideline states that PEG is superior in the effectiveness, adherence, and safety of fecal disimpaction and maintenance treatment for pediatric FC.1 PEG is available in two molecular weights: PEG 3350 and PEG 4000.20 Previous reports showed a significantly frequent stool passage in PEG than in placebo or lactulose.212223 In a previous study, most respondents preferred PEG, with a higher use in children aged > 1 year; however, lactulose was used as frequently as PEG in children aged < 1 year.11 Another study reported that lactulose was used most frequently, and PEG was used in only 10% of respondents.17 Borowitz et al.10 reported that magnesium hydroxide was the most commonly prescribed laxative (77%).
The respondents in our study most commonly chose lactulose, followed by PEG 4000 and probiotics. We found different prescription practices according to age (≥ 1 year and < 1 year) and between PGs and general pediatricians. General pediatricians may lack information about or experience with PEG. General pediatricians tend to use probiotics more than PGs in both age groups. Several other studies have shown the same tendency to frequently prescribe pre-, pro-, or synbiotics for pediatric FC.2425 Theoretically, alterations of gut microbiota can enhance gut motility through the production of short-chain fatty acids that lower the Ph in the colon and result in better colonic peristalsis and a decrease in colon transition time.26 However, no sufficient clinical evidence has been presented to support the use of probiotics, and the 2014 ESPGHAN/NASPGHAN guideline does not recommend their routine usage.1
Koppen et al.27 recommended that maintenance treatment should be continued for at least 2 months, and a weaning initiation should begin after a symptom-free duration of 1 month. Pijpers et al.28 reported that only 50% of pediatric patients with FC had symptom remission and laxative independence after 12 months of treatment, these results correlate with the 2014 ESPGHAN/NASPGHAN guideline that states approximately 50% of pediatric patients with FC referred to pediatric gastroenterologists will recover and stop pharmacologic treatment after 6–12 months.1 Some surveys showed a short duration of treatment for < 1 month, in 45%–86% of respondents.1719
The total treatment duration in our study was significantly longer in the PGs than that in the general pediatricians. PGs are more aware of the importance of adequate treatment duration, and may care for children whose symptoms are more complicated. To our knowledge, this study is the first to explore the differences in treatment duration between PGs and general pediatricians. No randomized-controlled trials have investigated the optimal duration of medical treatment in children with FC.1
The non-pharmacologic treatments were not being actively performed in our study. However, defecation diaries were used more frequently by the PGs than the pediatricians. Education is regarded as the first step in the non-pharmacologic treatment of pediatric FC for both parents and children, but more than half of the respondents in our study do not actively educate. Approximately 60% of the respondents in our study provide detailed explanations on toilet training for constipated children.
The dietary fiber, fluid, and physical activity are recommended with normal intake and level.1 Dietary intervention, such as an increase in fiber or fluid intake, is commonly recommended in pediatric FC.101529 In our study, the participants recommended diet modification primarily with an increase of fluid and fiber intake. Randomized-controlled trials have been performed about the effects of dietary fiber in pediatric FC.303132 A recent Korean study reported an enhancement of bowel movement and better stool consistency in pediatric patients with additional fluid intake during treatment of FC with PEG 4000,33 however, the quality of the evidence was low according to a recent systematic review.34
We found several discrepancies between actual practice and the ROME IV criteria, and between PGs and general pediatricians. Active educational efforts and activities are needed for primary care physicians in the practice of pediatric FC. Our survey data may aid in the construction of practical guidelines in consideration of the regional characteristics in the aspect of social culture, diet characteristic, and the general medical environment, and educational programs for pediatric FC.
 XML Download
XML Download