

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Appendicitis is the most common acute disease of the abdominal region requiring surgical intervention in children [1]. Urgent appendectomy has been accepted as the gold standard of treatment for over a hundred years. However, the body of research on nonoperative treatment of appendicitis (NOTA) has been increasing in recent years in adults and children alike [2]. NOTA for uncomplicated appendicitis in the pediatric population has been reported by many authors [345678]. Most studies have found NOTA to be safe and effective in terms of patient outcome as well as reduced medical cost [910]. However, studies have varied greatly in their treatment scheme or assessment of outcome. These studies also had different definitions of uncomplicated appendicitis which, at times, led to high failure rates of NOTA.
We have carried out NOTA in pediatric patients using strict diagnostic criteria for uncomplicated appendicitis. With rigorous selection of patients, we were able to safely apply NOTA in a pediatric population. The results are reported herein.
METHODS
All patients younger than 18 years visiting the emergency room (ER) with abdominal pain and diagnosed with appendicitis at Samsung Medical Center (Seoul, Korea) from March through September of 2017 were enrolled in this study. Patients' data were prospectively collected in the Pediatric Surgery Division database at Samsung Medical Center. Appendicitis was suspected when patients presented to the ER with a typical history of abdominal pain initially in the epigastric area and migrating to the right lower quadrant. Upon clinical suspicion of appendicitis, radiologic evaluation using either abdominal ultrasonography (performed by a pediatric radiology specialist) or computed tomography was performed. Diagnosis of appendicitis was confirmed when a dilated appendix with a diameter greater than 6 mm with periappendiceal infiltration was observed.
NOTA was considered in patients with uncomplicated appendicitis. Uncomplicated appendicitis was defined as: 1) appendicitis with a history of abdominal pain not exceeding 24 hours, 2) without radiologic evidence of appendicolith, appendiceal perforation or pelvic abscess, and 3) the absence of signs of frank generalized peritonitis (Table 1).
Table 1
Inclusion criteria for nonoperative treatment of appendicitis

Upon diagnosis of uncomplicated appendicitis and consent for NOTA, patients were admitted and started on intravenous antibiotics consisting of cefazolin and metronidazole. Initial assessment of abdominal pain is represented by the Numeric Rating Scale (range 0–10) and diet (including water) is restricted for the remainder of the day. The patients were evaluated on the morning of the following day and when abdominal pain had not progressed, regular diet was resumed. Abdominal pain was assessed 3 times throughout the second hospital day and progression of pain is considered as NOTA failure and the patient is selected for appendectomy. On the third hospital day, when there is no sign of progression of abdominal pain the patient is discharged. Lab tests including white blood cell (WBC) count and C-reactive protein (CRP) are performed initially, at discharge and at outpatient clinic visits. Patient was discharged even if the lab results were not normalized. Oral antibiotics (ampicillin-clavulanate) is continued until a total of seven days of antibiotics (intravenous plus oral) are given. The patient returns to the outpatient clinic for follow-up examination of symptoms. The management protocol for NOTA is outlined in Fig. 1.
Fig. 1
Management protocol for NOTA.
NOTA, nonoperative treatment of appendicitis; IV, intravenous; ER, emergency room; NPO, nothing by mouth; NRS, Numeric Rating Scale; OPD, outpatient department; f/u, follow-up.
This study was approved by the Institutional Review Board at Samsung Medical Center (IRB File No. 2019-06-037).
RESULTS
A total of 32 patients younger than 18 years old and who visited the ER were diagnosed with appendicitis. Among them, 23 patients had uncomplicated appendicitis and nine patients had complicated appendicitis. Twenty-two out of the 23 patients with uncomplicated appendicitis agreed to NOTA and were enrolled in the study. One patient's parents declined to participate and underwent laparoscopic appendectomy. All nine patients with complicated appendicitis underwent laparoscopic appendectomy. The patient selection process is outlined in Fig. 2.

The characteristics of the 22 patients who underwent NOTA are described in Table 2. There were nine boys and 13 girls. Mean age of patients was 11.8 years. Mean duration of pain prior to ER arrival was 12 hours. Radiologic evaluation of appendicitis was obtained via ultrasonography in five patients and computed tomography in 17 patients. Mean appendix diameter upon imaging was 8.3 mm.
Table 2
Clinical characteristics of patients

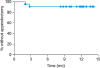
Initial success of NOTA, defined as resolution of abdominal pain and hospital discharge without appendectomy, was 100% (22 out of 22 patients). Length of hospital stay in these patients, including ER stay, was three days (median, range 2–4 days). Abdominal pain during admission showed significant decline from baseline with each passing hospital day and was 0 in all patients at discharge (Fig. 3A). Trends in the change of WBC count and CRP at initial ER visit, on discharge day, and on the day of clinic follow-up, is shown in Fig. 3B and C. WBC count was significantly decreased from baseline levels on discharge day and at outpatient clinic visit (p<0.001). Median follow-up time after discharge was 24.7 months (range 14.1–27.1 months). Two patients had recurrence of abdominal pain and were diagnosed with appendicitis at two and three months after completion of NOTA. These patients underwent routine laparoscopic appendectomy and were discharged without complications. Kaplan-Meier survival analysis revealed that 90% of patients undergoing NOTA were free from appendectomy at 15 months (Fig. 4).
Fig. 3
(A) Pain score reduction according to HD (NRS) (p<0.001). (B) (WBC count reduction of patients (p<0.001). (C) CRP count reduction of patients (p<0.001).
NRS, Numeric Rating Scale; WBC, white blood cell; CRP, C-reactive protein; ER, emergency room; HD, hospital day; OPD, outpatient department.
*p<0.05.

DISCUSSION
The dogma that appendicitis must be surgically managed in all cases has come under much scrutiny in recent years, with a large number of studies published on antibiotics therapy as the first line treatment for appendicitis in children. However, these studies showed many variations in patient selection for NOTA as well as the specifics of NOTA, including type of antibiotics used and the length of antibiotic use (Table 3) [91011]. Moreover, the definition of successful NOTA also varied between studies, leading to initial failure rates of NOTA from 1% to as high as 14% [12].
Table 3
Earlier studies of non-operative treatment of appendicitis

| Study | Symptom duration (hr) | Exclusion criteria (operation indication) | Antibiotics duration | Initial success rate (%) | Interval appendectomy (%) |
|---|---|---|---|---|---|
| Abeş et al. [3] | <24 | - Peritoneal sign | Until abdominal tenderness resolved | 15/16 (94) | 2/15 (13) |
| - Appendicolith | |||||
| - Free fluid | |||||
| Armstrong et al. [4] | <48 | - Hemodynamic compromise | Total of 7 day | 11/12 (92) | 2/11 (18) |
| - Abscess or phlegmon | |||||
| Svensson et al. [7] | - | - Perforated appendicitis | IV antibiotics for 48 hr and oral anti for 8 day | 22/24 (92) | 7/22 (32) |
| - Appendiceal mass | |||||
| Tanaka et al. [8] | - | - Pan-peritonitis | C-reactive protein level decreased to <0.5mg/dL | 77/78 (99) | 22/77 (29) |
| - Abscess or phlegmon | |||||
| Hartwich et al. [5] | <48 | - Presence of abscess | IV antibiotics for 6–8 hr and oral antibiotics for 1 wk | 21/24 (88) | 2/21 (10) |
| - Perforated appendicitis | |||||
| - Significant comorbidities | |||||
| Minneci et al. [6] | <48 | - White blood cell higher than 18,000 | IV antibiotics for minimum of 24 hr and oral antibiotics for total of 10 day | 35/37 (95) | 7/35 (20) |
| - Appendicolith, abscess, phlegmon | |||||
| - Perforation | |||||
| - Diffuse peritonitis |
Many previous studies selected patients with abdominal symptoms for less than 48 hours for NOTA, and some studies don't even have any criteria regarding duration of symptoms. Furthermore, some studies included patients who showed appendicolith in radiologic exam. We believe that if we select the patients for NOTA strictly, it may be possible to increase the initial success rate of NOTA. Therefore, we have applied stringent inclusion criteria of NOTA as uncomplicated appendicitis with a history of abdominal pain not exceeding 24 hours, without radiologic evidence of appendicolith, appendiceal perforation or pelvic abscess, and absence of signs of frank generalized peritonitis. Using these criteria, we have been able to achieve successful NOTA in 22 out of 22 consecutive pediatric patients in our center. Much of the initial reservation among surgeons surrounding NOTA is due to concerns about false positive diagnosis of uncomplicated appendicitis and delayed surgical intervention in case of perforation [13]. Although this study involves a relatively small cohort of patients, it puts forward selection criteria that may lead to minimization of false positive diagnoses of uncomplicated appendicitis and a high success rate of NOTA. There is a possibility that such stringent patient selection might lead to more patients receiving treatment with appendectomy, who would otherwise have been candidates for NOTA. However, it would better ensure patient safety when applying this relatively new treatment scheme in a larger study population or even everyday clinical practice.
Another point to raise regarding the safety of applying NOTA is the safety of delaying surgery in pediatric appendicitis [14]. Yardeni et al. [15] analyzed data from 126 children who underwent appendectomy and compared outcome measures according to the time interval from ER presentation to surgery. They showed that children receiving appendectomy within six and up to 24 hours from initial presentation had similar rates of perforation, operative time, postoperative complications, hospital length of stay and medical costs. In the treatment protocol of the current study, the patient was closely monitored for progression of abdominal pain, which was considered to be a key indicator of NOTA failure. Monitoring is most frequently done on the first and second days of admission to ensure early recognition of disease progression and timely surgical management. By doing so, NOTA may be more safely implemented among patients that require appendectomy after receiving surgery within 24 hours of presentation.
The limitations of this study are evident and have been discussed previously; the study population was small and was not sufficiently powered to prove the success rate of the NOTA protocol. However, the study provides supporting evidence for planning future clinical trials with larger patient populations applying these inclusion criteria and the treatment scheme for NOTA.
In conclusion, nonoperative treatment of uncomplicated appendicitis in children appears to be feasible and safe. Stringent patient selection for NOTA may be necessary to increase the initial success rate and safely apply NOTA for all children with uncomplicated appendicitis. Additional patient selection criteria and a standardized treatment protocol should be discussed in further studies.
 XML Download
XML Download