

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hemolytic uremic syndrome (HUS), also known as “hamburger disease”, is a clinical syndrome characterized by microangiopathic hemolytic anemia and thrombocytopenia. HUS is the most common cause of acute kidney injury in children younger than three years old [1]. Bacterial toxin, especially shigatoxin-producing Escherichia coli (STEC), also called as verotoxin-producing Escherichia coli (VTEC), is well known infectious etiology of HUS. E. coli serotype O157:H7 is the most common serotype, but various E. coli strains other than O157:H7 were reported [2].
HUS is generally a self-limiting disease with spontaneous recovery; however, 26% of patients develop renal failure, and mortality occurs in about 3%–5% [34]. The onset of HUS is usually preceded by gastroenteritis, characterized by fever, vomiting, abdominal pain, and diarrhea that is initially watery but then becomes bloody.
These symptoms, especially in infants or young children, may mimic appendicitis or other acute abdomen.
Although appendicitis is included in the differential diagnosis of HUS, HUS may present with appendicitis. There have been a limited number of reports in the literature worldwide on the presence of HUS after perforated appendicitis, or, its subsequent progression acute appendicitis [567]. However, this is the first case report in Korea of “Early appendicitis” that subsequently progressed to HUS.
Herein, we report a case of HUS preceded by appendicitis in a 23-month-old boy.
CASE REPORT
A previously healthy 23-month-old boy was admitted to the general ward with abdominal pain and bloody diarrhea of 3 days duration. The diarrhea began as loose stool, 2–3 times a day, but worsened to bloody, mucoid watery diarrhea, and became more frequent, with hourly discharges. Abdominal physical examination revealed no palpable masses, hyperactive bowel sound, and tenderness on both lower iliac fossa with mild muscle guarding.
Abdominal radiography showed gaseous distension of the colon (Fig. 1). Laboratory findings included leukocytosis (22.64 k/mm3) with an upper left shift (segment 82.9%), mild anemia (12.5 g/dL), thrombocytosis (456 k/mm3) and decreased serum glucose (65 mg/dL) and sodium (134 mg/dL) levels. Plasma urea and creatinine concentrations, and those of other electrolytes were within normal limits, and C-reactive protein (CRP) was also nearly normal (0.66 mg/dL).

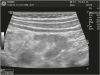
The patient was subjected to bowel sonography to exclude intussusception; with results showing no evidence of intussusception but edematous bowel wall thickening, which suggested enteritis, and a 6 mm dilatation of the appendix with wall thickening, which was suspicious of early appendicitis (Fig. 2). Intravenous antibiotics were initiated upon the suspicion of bacterial enteritis and symptomatic medication was administered for watery diarrhea and abdominal pain.
However, on hospital day (HD) #2, the patient exhibited more severe abdominal pain than that on the initial assessment. Physical examination revealed focal tenderness in the both lower quadrants with localized guarding and no evident rebound tenderness. Contrast abdominal computed tomography (CT) demonstrated a dilated, fluid filled tubular structure in the lower right quadrant indicative of appendicitis (Fig. 3). On the basis of these findings, the patient was transferred to the department of general surgery and undertaken laparoscopic appendectomy. The laparoscopic findings included wall thickening in the cecum and mild inflammation in the appendix. Pathologic examination of the resected segment revealed telangiectasia of the serosa, and the lumen contained suppurative exudate with acute inflammation, but no thrombotic microangiopathy was observed (Fig. 4).
Fig. 3
Enhancing wall thickening and fluid filled dilatation of appendix on abdominal-pelvis computed tomography.

Fig. 4
Histologic examination shows telangiectasia of the serosa and the lumen contains suppurative exudate. (A) H&E, ×40; (B) H&E, ×400.
H&E, hematoxylin and eosin.

On HD #3 and #4, the fever did not subside and abdominal pain persisted. Hemoglobin decreased from 12.5 to 8.0 g/dL and platelet decreased from 456 to 29 k/mm3. Serum electrolytes also showed an imbalance, with sodium 134 mmol/L and potassium 5.1 mmol/L. Urea had increased to 46.1 mg/dL and creatinine also increased to 2.7 mg/dL. Peripheral blood morphology revealed the presence of schistocytes, a diagnostic indication of HUS.
The patient was transferred to the Seoul National University Children's Hospital due to rapid aggravation of creatinine level and the possibility of requirement of dialysis due to acute renal failure. On HD #5, stool polymerase chain reaction, taken the first day of admission at our hospital, was positive for VTEC which is one of the common causes of HUS.
At that hospital, his laboratory findings were worsened to creatinine 3.98 mg/dL, hemoglobin 6.3 g/dL, and platelet 19,000/mm3. Other laboratory findings including CRP had no significant change. After 5 days of daily hemodialysis and supportive management, his urine output, fever, bloody diarrhea, and abdominal pain were recovered. Also, the laboratory findings were much improved to creatinine 0.69 mg/dL, hemoglobin 10 g/dL, platelet 396,000/mm3 at the time of discharge (Fig. 5). After discharge, he takes medication for hypertension but has no another complication so far.
Fig. 5
Laboratory findings during HD #1 to #18. He undertaken appendectomy on HD #2, and transferred to another hospital for hemodialysis on HD #4. After daily hemodialysis for 5 days, his urine output, fever, and abdominal pain were improved. The abnormal laboratory findings were recovered until discharge on HD #18.
HD, hospital day; Hb, hemoglobin; PLT, platelet; Cr, creatinine; AST, aspartate transaminase; ALT, alanine aminotransferase.

DISCUSSION
In 1994, a massive outbreak of E. coli serotype O157:H7 infection was reported in the western United States of America. The patients had a history of consuming ground beef at a fast-food restaurant chain. Subsequently, STEC raised public and medical awareness, and HUS began to be referred to as “hamburger disease” [8]. In Korea, ground beef is used widely in a variety of foods other than hamburger.
Thus, when clinicians inquire about a patient's history of gastrointestinal symptoms, culture-based examinations can be helpful. In our case, the boy reported having eaten “Donggeurangttang”, the Korean meat ball, made with ground beef 1 week before the onset of the primary symptom. The beef has been stored in freezer for several months.
Also, when evaluating a child with acute abdominal pain, careful history taking and repeated physical examinations are important [9]. Our patient's symptoms and physical examinations, as well as the imaging studies corresponded to acute appendicitis. Of note, the patient was set to be discharged after checking the routine laboratory studies on HD #4.
Thus, despite a primary diagnosis of acute abdomen from the initial imaging tests and physical examinations, clinicians should always be aware of a potentially fatal disease, such as HUS and careful serial checkup of the patient's vital signs, and urine output and laboratory examinations should be performed.
HUS is the most common cause of acute renal failure in previously healthy infants and young children and is a significant cause of acute mortality and morbidity in these patients [10]. Early recognition of HUS, meticulous maintenance of fluid balance, and proper dialysis prevent acute mortality.
To our knowledge, the case presented herein is the first case report of acute appendicitis followed by HUS in South Korea.
 XML Download
XML Download