

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Amongst the congenital chest wall deformities, absence/hypoplasia or fusion abnormalities of ribs are very rare [1]. Presentation varies from asymptomatic to severe respiratory distress in an infant. Computerized tomography (CT) scan chest with 3-dimensional (3D) reconstruction is a good investigation to delineate complex anatomy [2]. Treatment of these anatomical deviations varies from observation, physiotherapy to surgical intervention [3]. Here, we present a case of hypoplastic and fused lower ribs, its presentation, diagnostic dilemma, and management.
CASE REPORT
A 3- month-old male child presented with complaints of recurrent respiratory infection since birth and respiratory distress for 15 days. He was full term and born by normal vaginal delivery at a peripheral hospital. The mother was non-diabetic and the antenatal period was uneventful. There was no obvious chest or abdominal abnormality on inspection except for increased respiratory rate. The baby was maintaining normal oxygen saturation on room air but there were subcostal retractions and nasal flaring. On auscultation, air entry was better on the right side and the heart sounds were also better heard on the right side. There were no added sounds in both lungs.
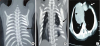
A plain radiograph chest X-ray (Fig. 1) was suspicious of bowel loops or stomach herniating into the left hemithorax. With a working diagnosis of congenital diaphragmatic hernia (CDH)/hiatus hernia, the patient was planned for emergency surgery. The patient was explored through a left subcostal incision. There was no diaphragmatic defect. Although the left diaphragm was higher up in position, it was normal, thick and muscular and not thin and redundant, as in diaphragmatic eventration. There was no paraesophageal or sliding hernia. The spleen was found to be free from its ligamentous attachments. On palpation, of the left chest wall, the lower ribs and costal cartilages were absent along with a portion of the lower sternum. There were deficiency and absence of attachment of pectoral muscles in that region creating a 4×3 cm size muscular defect, which was repaired with non-absorbable sutures. The post-operative period was uneventful and the child was discharged 5 days later. During follow up, the child was evaluated with CT chest with 3D reconstruction (Fig. 2) which was suggestive of dextrocardia, partially fused left 5th and 6th ribs, hypoplastic 7th and 8th ribs, left lung smaller in volume as compared to the right lung, sternal defect and scoliosis of the dorso-lumbar spine. To rule out any associated syndromic conditions, ultrasound (USG) of kidney, ureter, bladder (KUB), 2-dimensional (2D) echocardiography (ECHO) and gastroesophageal reflux (GER) scan were done, which were normal. The child was doing well during the last follow up at 8 months age.

DISCUSSION
Congenital absence/hypoplasia of ribs is a condition without certain etiology with the most commonly accepted pathogenesis behind the anomaly being insufficient blood supply during the embryonic period [3]. These anomalies can be subdivided into superior and inferior rib deformity. Generally, a superior rib deformity would be detected by the neonatologist at the time of birth, whereas an inferior rib deformity would most likely be overlooked [3]. The absence of superior ribs could lead to more aesthetic problems like asymmetric of shoulders and thoracic scoliosis, while the absence of multiple lower ribs could affect respiration and circulation [4]. Deformities of the inferior ribs like in the index case can cause ‘lung hernia’ that produces an unstable chest, leading to recurrent respiratory infections and paradoxical respiratory movements. Severe cases can affect heart ejection fraction also [4].
In the index case, costal cartilages of lower ribs were absent with hypoplasia of 7th and 8th rib, which created a muscular defect through which lung was herniating and was causing recurrent respiratory symptoms. On the chest radiograph, the muscular defect with lung herniation was mistaken for bowel loops entering the thoracic cavity, giving the impression of diaphragmatic hernia and the dextrocardia was mistaken for the secondary mediastinal shift (Fig. 1). Routinely, in cases of CDH, the symptomatic child requires only an X-ray chest as radiological investigation before emergency surgery. In the index case, the muscular defect was not visible with the naked eye. It may have been detected during the clinical examination at first visit if the condition had been suspected and palpation was done with prior knowledge of the condition. Although the treatment would have remained the same, i.e., closure of the muscular defect, chest wall and rib anomalies require proper pre-operative work up in the form of CT chest with 3D reconstruction.
Rib fusion may involve any segment of rib (posterior, lateral or anterior). The presence of fused ribs should raise suspicion for additional anomalies. Indeed, fused ribs are identified in up to 30% of patients with congenital scoliosis [5]. In the index case, two ribs, i.e., 5th and 6th ribs were fused and mild scoliosis of the dorso-lumbar spine was also associated. Other investigations (USG, 2D ECHO, GER scan) to rule out syndromic associations, were normal.
Poland syndrome (PS) is also associated with chest wall deformities and rib anomalies although it is known to have a mixture of clinical manifestations. In the index case, there were a few components of PS, i.e., absence of sternal attachment of pectoralis major, mild scoliosis and rib abnormality. However, major component, i.e., absence of pectoral muscles, cartilage agenesis of 2nd to 5th ribs on the ipsilateral side, athelia, amastia, upper limb anomalies like syndactyly and hemivertebra were absent. There are reports of association of PS with dextrocardia which was present in the index case also [6]. In severe cases there may be hypoplasia of latissimus dorsi and deltoid muscles as well as severe rib and diaphragmatic defects resulting in lung herniation [7].
Congenital chest wall deformities should be corrected in selected patients. Early surgical intervention should be carried out in symptomatic patients and those with large, unstable chest wall defects. The prevention of progressive deformities during the growth period or improvement of physiological function or appearance of the patient are the main indications [8]. These children require proper follow-up even in the course of conservative treatment because it is imperative to identify the optimal time to intervene so that it can minimize respiratory morbidity, maximize the growth potential of lungs and better quality of life outcomes [34].
Absence/hypoplastic or fusion abnormalities of ribs are very rare and awareness of these anomalies precede proper investigations to delineate anatomy. Treatment should be at an optimal age and depends upon symptomatology and radiological features, long-term follow-up is necessary to assess physical growth and change in symptoms.
 XML Download
XML Download