

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Digital dentistry is a hot topic in the dental field, in which digital data are used in all processes.12345678 Conventional treatments were limited to provisional and single-unit crowns.910 However, digital dentistry has a growing potential and is currently used in the fabrication of long-span crown and bridges, implant prostheses, dentures, and total dentistry.11121314151617 Rehabilitation with complete denture is a treatment for edentulous patients and includes several stages such as diagnosis, preliminary impression followed by definitive impression, measurement of the centric relation (CR) and vertical dimension (VD), wax denture try-in, and delivery of definitive denture.18 Digitization of the procedure could simplify the complex process of fabricating the prosthesis and also shorten the time required.13 Computer-aided design (CAD) files can be stored permanently; this enables the manufacture of materials without the need for additional impressions. In addition, various types of articulations can be achieved, allowing applicability as an educational tool. Several techniques for fabrication of complete dentures and outcome of patient satisfaction have been reported.1920
However, digitization of complete dentures is a challenging process,21 considering that total dentistry is performed in edentulous areas where it is difficult to obtain the surface impressions, and VD and CR values using digital methods. Therefore, many studies have used the existing analog method.1112131415 Digital dentures are often limited to fab rication of the prostheses and not used in the clinical setting.13 The impression of the surface, and VD and CR acquisitions are difficult to digitize with the current technology in complete denture treatment.
Digitization as a protocol for use in total dentistry can be completed in a short time-period. It involves newly developed concepts, materials, and techniques as well as prosthetic manufacturing. The conventional open-mouth technique of impression-making is validated and widely used in fabricating the complete denture,15 but it is time consuming and requires additional information of the VD, CR, and anterior tooth position; therefore, it is advantageous to apply a closed-mouth impression technique for the digitization of complete dentures. The closed-mouth impression technique involves making an individual tray containing an occlusal rim in the preliminary model and, subsequently, the definitive impression in which the maxillary and mandible occlusal rims are in contact with each other; provisional VD and CR are simultaneously determined. This method has the advantage of reducing the number of clinic visits since definitive impression can be achieved through definitive intermaxillary relationship.1617 Closed-mouth technique with digital device, as the method of choice for making the impression, allows the achievement of more accurate impression surface and VD and CR values at a shorter time-period compared to existing conventional techniques. We combined our new approach and the average VD values in edentulous patients in the production of the digital device with 3D printing.
However, a closed-mouth impression method performed with a digital device would have poor reliability if there are significant differences in the impression as compared to that through existing conventional techniques. Therefore, a comparative study on the differences between impressions obtained through the various techniques is needed. Studies including a digitized device and software have been reported;22232425 the method employed was to scan the target objects using a scanner and overlay the acquired images using software in order to compare the differences.25 The technique of superimposition is simple, reliable, and has been used in several recent studies.2627 In this study, superimposition technology of a surface-matching software was used to compare the effectiveness of the conventional impression method (CI) versus simple modified closed-mouth impression method with a novel tray (SI), and the impressions acquired with the digital impression method using an intraoral scanner (DI) were compared to determine the capability to capture the complete edentulous surface. The null hypothesis of the study is that there is no difference among the three impression techniques in all areas of maxillary and mandibular edentulism.
MATERIALS AND METHODS
Five volunteers (four men and one woman; mean age, 62.7 years) with maxillary and mandibular edentulous jaws were included. Power analysis with effect size of 2.2, alpha of 0.05, and power of 0.80 revealed that five people per group would be needed to detect the postulated effect size. Ethical approval was obtained from the Institutional Review Board of Chonnam National University Dental Hospital (IRB no. CNUDH-2017-015). All volunteers who underwent conventional or digital impression in the study signed informed consents form prior to participation. The inclusion criteria were as follows25: fully edentulous patients requiring fabrication of complete dentures at least three months after extraction, absence of masticatory or motor system disorder, and ability to understand and respond to spoken Korean.
The entire process was carried out by a single prosthodontist with thirty years of experience. Impressions were made using each of the three methods of CI, SI, and DI in every volunteer, amounting to a total of fifteen impressions.
For each volunteer, prior to performing the CI method, a preliminary impression was made using irreversible hydrocolloid (Cavex Impressional, Cavex Holland BV, Haarlem, The Netherlands) and an edentulous impression metal tray (Schreinemakers metal edentulous impression trays, Clan Dental Products, Maarheeze, The Netherlands); subsequently, an individual tray was made with acrylic resin (Quicky, Nissin Dental Products Inc., Kyoto, Japan) using conventional methods, and definitive impressions were made with the open-mouth technique.28 Modeling compound (Peri Compound, GC Corporation, Tokyo, Japan) and vinylpolysiloxane (Exadenture, GC Corporation, Tokyo, Japan) were used as materials for the definitive impression.
In the SI method of the present study, a new tray was designed to facilitate efficient, simultaneous determination of the VD, CR, and anterior tooth positions in a preliminary impression model as follows. First, the preliminary cast was scanned using a model scanner (D700, 3Shape, Copenhagen, Denmark), and the scan file was transferred to a dental CAD software (3Shape's CAD Design software, 3Shape, Copenhagen, Denmark). The tray was designed using the individual tray module of the software. For the space occupied by the modeling compound under nonselected pressure, the inner space of the tray was set to 4 mm. The handle of the maxillary tray was omitted, and the VD and position of the maxillary anterior teeth were set by making the plate detachable instead of with occlusal rim (Fig. 1A). The handle of the mandibular tray was also omitted, a short rim was created at the anterior position, and the CR was set by biting down with the maxillary plate. Subsequently, a rim with an undercut was made on the posterior aspect of the mandibular tray to ensure stability of the silicone bite-material (Regisil, Dentsply International Inc., Milford, DE, USA) (Fig. 1B).
Modeling compound was applied to the maxillary tray using a molding machine with an automatic border,29 which was then placed at the correct position within the oral cavity. The plate of the maxillary tray was moved to the anterior, posterior, superior, and inferior positions of the maxillary anterior teeth and subsequently fixed with resin (Revotek LC, GC Corporation, Tokyo, Japan); a definitive impression was obtained using the conventional method.28 The mandibular tray was applied to the edentulous mandibular ridge while the maxillary impression was positioned in the mouth. After determining the CR position using the bimanual method,30 the volunteers were instructed to close their mouth such that the anterior rim and maxillary plate were in contact. The plate or anterior rim was removed (as required) to ensure accurate determination of the VD. The preset CR and VD were rechecked after molding of the mandibular border, and a definitive impression was made using the closed-mouth technique.31
Digital impressions of the edentulous jaws (DI method) were made using an intraoral scanner (CS3500, Carestream Dental LLC, Atlanta, GA, USA) and individual retractor (Scan retractor, DIO Corporation, Busan, Korea) as follows. First, the edentulous jaws were cleaned, saliva was wiped dry, and retractor was adjusted according to the size of the arch. Scanning was performed by retracting the lip and cheek with the scanner head while stretching and fixing the vestibular area with the retractor. The maxilla was scanned from the left to the right maxillary tuberosity along the posterior palatal seal; next, the vestibule and palate were sequentially scanned to overlap with the scanned residual ridge. In a similar manner, the mandible was scanned from the retromolar pad on one side to the contralateral side along the residual ridge, followed by buccal vestibular scanning with retraction of the lip and cheek; finally, the lingual vestibule was scanned with retraction of the tongue. The scanned data were confirmed visually and saved in Standard Tessellation Language (STL) format.
CI and SI methods were used to obtain dental stone models (Zostone, Shimomura Gypsum Co., Ltd., Saitama, Japan) following conventional procedure, and the STL-model cast file was obtained using a model scanner.
The STL files of each edentulous surface from the CI method were superimposed onto those from the SI and DI methods using surface-matching software (Geomagic Control 2014, 3D Systems, Rock Hill, SC, USA);31 specifically, the best-fit algorithm of the software was used. Comparisons of the CI and SI methods were made at five different regions of the maxilla and mandible.32 Due to limitations of the DI method in making the impression of movable tissue, the CI and DI methods were compared at four areas of the maxilla and two areas of the mandible. Comparisons of the CI and SI methods, and the CI and DI methods are shown in Fig. 2. The overall study workflow is shown in Fig. 3.
Statistical analysis was performed using Statistics Package for the Social Sciences software (SPSS version 23.0, SPSS Inc., Chicago, IL, USA). Kruskal-Wallis test was used to compare the impression techniques among multiple areas in the five volunteers.32 P < .05 was considered to indicate statistical significance.
RESULTS
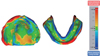
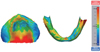
The results of SI superimposed on those of CI are shown in Fig. 4, Fig. 5 and Fig. 6. CI achieved less depressed values overall with a mean difference of 0.03 ± 0.01 mm in the maxilla; the soft palate had the greatest difference of about 0.14 ± 0.02 mm, and the variations in the other areas were −0.10 ± 0.03 mm (medial palatine raphe), 0.04 ± 0.01 mm (hard palate), 0.01 ± 0.05 mm (residual ridge), and 0.07 ± 0.02 mm (buccal vestibule). The average difference was −0.27 ± 0.56 mm in the mandible, and the CI method achieved more depressed values in this region. Moreover, there was the greatest difference in the lingual vestibule (about −1.2 ± 1.40 mm), and the differences in the other areas were −0.25 ± 0.04 mm (residual ridge), −0.34 ± 0.08 mm (buccal shelf), −0.26 ± 0.17 mm (retromolar pad), and 0.53 ± 0.09 mm (buccal vestibule). The results of superimposition for the SI and the DI methods are shown in Fig. 5, Fig. 6 and Fig. 7. DI achieved more depressed values and showed an average difference of 0.09 ± 0.08 mm in the maxilla. The soft palate had a much greater difference of 0.86 ± 0.77 mm, and the variations in the other areas were 0.05 ± 0.05 mm (medial palatine raphe), 0.18 ± 0.15 mm (hard palate), and 0.05 ± 0.07 mm (residual ridge). The mandible was subjected to less pressure under the DI method and had a difference of 0.04 ± 0.05 mm. A difference in the value of the residual ridge was 0.11 ± 0.17 mm and that of the buccal shelf was 0.09 ± 0.15 mm. There was no statistically significant difference among the values.
DISCUSSION
This study compared the performances of the CI, SI, and DI methods in edentulous jaws. Compared with the CI method, the SI method achieved somewhat different results; however, the overall difference was not significant. There was no difference between the results obtained through the CI and DI methods in the supporting areas. Based on these findings, the null hypothesis of this study was rejected.
The workflow for digital denture requires an efficient method for delivery of patient information in the clinic and production of digital prostheses in the laboratory. In this study, the VD and CR values were obtained on the same day of making the definitive impression by using a newly designed tray to enhance efficiency of the closed-mouth technique. The experimental results revealed a difference of 0.03 mm, which is clinically acceptable.33 Therefore, the proposed method can be applied to a digital denture protocol in the clinical setting.
The conventional individual tray for complete dentures was produced in three steps of making the preliminary impression, stone model, and tray comprising auto-polymerized resin and required an extended amount of time. In this study, the proposed new tray was produced by 3D printing of a CAD file in approximately an hour, without making of a stone cast after the preliminary impression. The individual tray was fabricated from an impression through intraoral scanning; therefore, it was easy to use. Moreover, since the occlusal rim was constructed based of the average VD,3435 measurement of the VD was possible with minor adjustment. Additionally, the mandibular occlusal rim was constructed based only on the anterior part of the tray; hence, it was possible to obtain the CR position rapidly. Automatic border modeling used in this method enabled a technique to increase the speed of locating the trays.29 The maxillary tray was first fixed with a modeling compound gun and then positioned according to the CR through bimanual method,30 and the rim of the mandibular tray was adjusted to the VD. Since the trays could be easily fixed using modeling compound, the process of making a definitive impression with polyvinylsiloxane impression material was also simple.
There was no clinically significant difference between the CI and SI methods in capturing the impression in edentulous individuals, which is consistent with the results of a previous report.36 However, the statistical values of the present results may represent difficulties when considering clinicians' viewpoint. In particular, the soft palate presented the largest difference, due to not only the presence of movable tissue, but also limitations of the location. However, in the case of edentulous mandibular impressions, the SI method could be the causal factor for the impression results because the patient's mouth is closed and the impression is made to withstand the patients' muscle strength and tongue movement; the tongue movement resulted in extension of the border of the impression in the lingual vestibule area. The results of this study are consistent with those of previous studies on impression using the closed-mouth functional technique.37 Clinically acceptable extension of the lingual border is a key factor to enhance the retention of the mandibular complete denture.36 Our results demonstrated that the SI method can improve retention of the mandibular denture.
Impression acquisition methods using an intraoral scanner are gradually gaining popularity in the dental field.1 These techniques are commonly used in the partially edentulous jaw; in case of completely edentulous, several errors may occur due to lack of anatomical indicators. In addition, obtaining an impression of the complete edentulous arch has several challenges due to inappropriate shape and size of the scanner. Despite the incapability of an intraoral scanner to make a definitive impression of complete dentures, we compared the DI method to the existing CI method to provide basic information that may enable future study on digital denture. Movable tissues such as the vestibule and soft palate were extremely unstable in some cases; therefore, the performances of the DI and CI methods were compared only in the supporting areas.
Our results indicated that there was no difference between the CI and DI methods in the supporting areas. Other studies have suggested several complementary measures to overcome the accuracy limitation.3839 However, since only the supporting areas with limited movable tissues were compared, the results are considered almost similar. Recently, in the field of digital dentistry, several advances have been made in the intraoral scanner,40 and its accuracy has been proven in many studies.41424344 Our study demonstrated that intraoral scanners can be used in soft tissues. The results obtained by scanning of the soft tissues were different from those of the teeth, since the shape and size of the scanner are optimized for scanning of the teeth. Improved results may be obtained using a scanner developed with specialized shape for targeting soft tissues.
In the present study, we newly attempted 3D analysis of edentulous patients. However, the study was limited to five patients. Additionally, there is uncertainty regarding the best-fit algorithm for appropriate comparisons in the dental field. Future studies on the fabrication of digital dentures with a larger-sized sample are needed. Our study highlights that it is possible to fabricate complete dentures in a single day in the near future.
CONCLUSION
Within the limits of this study, the following conclusions were drawn. First, there was no significant difference between the open-mouth CI method and closed-mouth SI method in maxillary and mandibular edentulous patients. Second, there was no significant difference in the supporting areas between the DI method and CI method in edentulous patients.





 XML Download
XML Download