

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Alzheimer's disease (AD) is the most common neurodegenerative disease, which leads to deterioration of cognitive function, functional abilities needed for independent living.1 The overall number of persons with AD is increasing, representing a major public health challenge.2 It is therefore necessary to develop pharmacological and/or non-pharmacological treatments to delay or halt the cognitive and functional decline associated with the diseases. Unfortunately, current pharmacological therapies such as acetylcholinesterase inhibitor have limited efficacy in the prevention of the disease progression.34 Nonpharmacological approaches, such as cognitive training, cognitive stimulation, and cognitive rehabilitation have been studied as potential strategies for prevention and treatment of AD.5 Among various approaches, cognitive training is the most effective approach as compared to cognitive stimulation and cognitive rehabilitation in patients with mild cognitive impairment (MCI) or early AD.6 Cognitive training refers to a series of standardized tasks with inherent challenges that target specific cognitive domains,57 and is based on the principles of neuroplasticity and restoration of cognitive abilities.89 Primary objective of cognitive training is to enhance or at least maintain function in a given cognitive domain.
Accumulating evidence indicate that cognitive training could benefit patients with early AD. Recent systemic analysis reported positive effect of cognitive training among 31 randomized controlled trials in patients with mild and moderate AD.10 The pattern of effects of cognitive training was inconsistent across the studies; positive effects were mostly observed in a single global or a few training. Other small-scaled studies also reported positive effects in separate cognitive domains such as working memory and executive function.1112
A traditional cognitive training requires a face-to-face interaction and teaching of new learning strategies using paper-and-pencil approach.10 Computer-based cognitive training programs which are relatively easy to access are also being widely developed and applied.1113 However, it is challenging to equip all institutions with the electronic devices for computer-based training. Also, using electronic devices may be hard for elderly and requires special guidance. A recent study by Tsolaki et al.14 reported that both computer-based and paper-based cognitive training (PBCT) are beneficial in MCI patients, however, traditional PBCT had better results in general cognitive function, learning ability, delayed verbal recall, visual memory, verbal fluency and visual selective attention and it also transfers the primary cognitive benefit in real life.
This study designed sets of cognitive training program, “Gipum-seo,” on subskills of memory, language, attention, visuospatial function and calculation, which consists of different levels of difficulty using predesigned paper-and-pencil exercises. The program is offered over 3 months in community-dwelling older persons with mild AD. The main goal was to clarify the effects of the cognitive training on patients' cognitive functioning.
METHODS
Study subjects
Patients with memory deterioration who had visited the Veteran Health Service Medical Center, from January 2015 to October 2016, were selected for this study. Patients were diagnosed with Alzheimer dementia, based on the criteria of the National Institute of Neurologic and Communicative Disorders and Stroke-Alzheimer Disease and Related Disorders Association standard15; patients with mild (early-stage) symptom [Clinical Dementia Rating Scale16 (CDR) or 0.5 or 1] were enrolled for the study. The dosage of medication for all the selected patients remained unchanged for 3 months. Exclusion criteria were: 1) Brain tumor or encephalitis; 2) Mental illnesses, based on the Diagnostic and Statistical Manual of Mental Disorders criteria, within 2 years before the start of the study; 3) Severe depression (Hamilton Depression Rating Scale score >18); 4) Parkinson's disease, Huntington's disease, or any other neurological disorders of normal pressure hydrocephalus; 5) Cases of medical diseases (liver disease, kidney disease, thyroid disease) that cause other cognitive function decline; 6) Patients with alcohol or drug addiction history within 2 years before the start of the study; 7) A physical disability, that may hinder the completion of a cognitive training program. All patients underwent basic demographic investigation and screening tests using the Korean version of the Mini-Mental State Examination (K-MMSE).17 The severity of Alzheimer's disease of patient was assessed based on the CDR.
Study design
All subjects underwent physical and neurological examinations. All patients conducted neuropsychological test and brain MRI at baseline. A total of 40 patients with early AD were enrolled at the Veteran Health Service Medical Center. The subjects were randomly assigned to either attend the PBCT (20 patients) or in the control group where they received the usual standard clinical care (20 patients). After 12 weeks, a set of PBCT were conducted, and the neuropsychological test was repeated within two weeks of completion. This study was approved by the Medical Research Ethics Committee of the Veteran Health Service Medical Center.
PBCT
The cognitive training program is a step-by-step customized PBCT, which covers a visuospatial, language, attention, memory and calculation. The primary aim of this program was to improve global cognitive function by combined training of subdomains. Each chapter of training entailed 10 to 20 tasks and focused on training of single domain. Skilled occupational therapist was providing the subjects with appropriate instructions of the program in each session. The intervention was carried out at the dementia center of Veteran Health Service Medical Center and performed twice a week (60 minutes per session), for 12 weeks.
Neuropsychological test
The Seoul Neuropsychological Screening Battery was conducted for the neuropsychological assessment of each cognitive function area of the patient.18 For each cognitive domain, concentration ability was investigated using the ‘forward and backward’ of the digit span, language ability was investigated using the Korean version of the Boston Naming Test (K-BNT)19 and spatio-temporal ability was investigated using the tracing drawings score of the Rey Complex Figure test (RCFT).20 Verbal memory and visual memory were assessed using immediate recall scores (total score of 3 trials), delayed recall scores, and recognition test scores of each Seoul Verbal Learning Test (SVLT)18 and RCFT.20 For executive function examination, sum of two (animal and market) semantic word fluency scores and sum of the three (ㄱ, ㅇ, ㅅ) phonemic word fluency score of Controlled Oral Word Association Test,21 and word/color reading score of the Korean-Color Word Stroop Test were used.22 Neuropsychological test was performed before the 12-week of PBCT, and follow-up test was performed 13 to 14 weeks after the baseline examination to confirm immediate effects of PBCT.
Statistical analysis method
All statistical analyses were done using SPSS 18.0 (IBM Corp., Armonk, NY, USA) with the 2-tailed test, with the level of significance 0.05. Mann-Whitney U test was used for the analysis of means for continuous variables. The percentage comparison of categorical data was performed using the chi-square test. Efficacy assessment was based on a pre/post comparison of the evaluations carried out at the baseline, and at 12 weeks. For this test, repeated measure of general linear model was used.
RESULTS
Demographic analysis
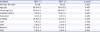
No significant difference was observed based on age, sex, education and training, and clinical dementia stage between the experimental and control groups. Also, no significant difference was observed between the groups in terms of K-MMSE, CDR, and Geriatric Depression Scale (Table 1).
Table 1
Demographic data comparing PBCT (−) patients and PBCT (+) patients (mean±standard deviation)
Overall cognitive assessment
The K-MMSE score showed a significant improvement in the paper-based cognitive program group (25.90±3.8) as compared to the control group (23.7±2.8) (p=0.042). The CDR scores of the computer-based cognitive program group significantly reduced to 0.9±3.9, compared with 0.55±0.5 of the baseline test (p=0.034). Neuropsychological tests also showed significant improvements in various areas as compared to control groups. Digit forward span was 3.60±1.2 and 4.40±1.2, for before and after PBCT, respectively. In addition, digit backward span was 2.60±0.6 and 3.90±1.6, for before and after PBCT, respectively. In the ‘go-no-go’ test, the PBCT group results were 11.80±4.5 and 16.69±4.7, for before and after PBCT, respectively. The K-BNT was 43.20±7.3 and 49.00±6.5 (p=0.043), for before and after the PBCT, and showed significant improvement in PBCT group. The results of the PBCT group for the stroop test showed significant improvement in word reading (102.60±10.7 and 108.80±8.9). No significant change was observed in both verbal and visuospatial memory between two groups (Table 2). Significant improvement in language, attention, and executive function of the PBCT group compared to the control was observed.
Table 2
Comparison of neuropsychological tests between PBCT (−) patients and PBCT (+) patients, at baseline and after 12 weeks follow up (mean±standard deviation)
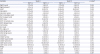
PBCT: paper-based cognitive training, K-BNT: Korean version of the Boston Naming Test, SVLT: Seoul Verbal Learning Test, RCFT: Rey-Osterrieth Complex Figure Test, COWAT: Controlled Oral Word Association Test, CWST: Color Word Stroop Test, MMSE: Mini-Mental State Examination, CDR: Clinical Dementia Rating Scale, SOB: sum of box, GDS: Geriatric Depression Scale.
*Repeated measures of General Linear Model were used.
DISCUSSION
The present study provided evidence that traditional PBCT improves cognitive functions in various areas. Specifically, this study's results showed that cognitive training had a significant impact on language, attention and executive function. Considering the limited pharmacological therapies available for AD, concurrent cognitive training may be an alternative treatment option due to simple and easy accessibility.
Previous studies reported notable improvement in global cognitive function, visuospatial abilities,23 and executive function11 after intervention by cognitive training. A positive result was often observed in global cognition, and was rarely observed in separate cognitive domains.10 Since global cognitive measures such as MMSE briefly reflects several cognitive functions, common improvement in different cognitive domains after cognitive training may be expected. Although number of previous studies reported beneficial effect of cognitive training for memory function,24 this study did not show tendency of positive effect but there was no significant difference. It is probably because this cognitive training program was not designed as combined cognitive training rather than memory strategy training. A previous study that compared combined cognitive training and pure memory training found combined cognitive training to be less efficient in memory outcome.25 Systemic review of cognitive training showed that studies with more intensive or specific cognitive training programs tend to show better efficacy.10
There are a number of limitations of this present study. First, the training duration was too short to confirm the effect of cognitive training program. Second, the follow-up period was relatively short, and longer follow-up period would be necessary for more robust and accurate results. Third, the study lacked analysis for additional confounders, such as APOE ε4 status, or medical condition of the participants which may affect the neuropsychological performance in AD patient. Finally, the sample size was small, and study with larger number of participants may be needed.
This study evaluated the effects of a PBCT, and the results indicated significant improvement in both global cognitive test and on language, attention and executive domain in the training group. The PBCT can be applied in community care facilities or home-basis, and this study result showed promising result in developing training methods to delay cognitive decline in early-stage AD patients. A further study applied in larger cohort with intensified modality is necessary in the future.
 XML Download
XML Download