

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Rahnella aquatilis exists in fresh water as an environmental organism and can cause infectious disease but the case of infection by this organism is uncommon [1]. Currently, little is known about the clinical manifestation, diagnosis and treatment for R. aquatilis. In Korea, there was only one report of bacteremia with this organism in hemodialysis patient which was published in 1997 [2]. This report describe a clinical course and treatment for a patient suffered from R. aquatilis bacteremia.
Case report
A 58-year-old woman visited our hospital for breast cancer treatment. On 23 September, 2015, she underwent modified radical mastectomy of the left breast because of invasive ductal carcinoma. Chemotherapy with doxorubicin (60 mg/m2 body surface area [BSA]) and cyclophosphamide (600 mg/m2 BSA) was administered four times between 2 November, 2015, and 1 January, 2016. Starting from 25 January, 2016, the patient was administered paclitaxel infusion (80 mg/m2 BSA) through a chemoport (B. Braun Celsite® Epoxy, France) which was inserted on that day via right subclavian vein for 12 cycles of infusion. On 12 April, 2016, the patient presented at our hospital for the tenth infusion of paclitaxel. At admission, her vital signs were stable, and the leukocyte count was 5,740/mm3 (segmented neutrophils, 61.1%). Before chemotherapy, saline was infused through the chemoport for hydration. Fourty minutes after the start of hydration, the patient complained of chills; 30 minutes later, she presented high fever (39°C) without any other symptoms except chills. The patient was administered an antipyretic, and two sets of blood samples were collected at different venous sites on the body. Blood cultures were performed using the VITEK 2 (bioMérieux, Marcy l'Etoile, France) automated system. On 13 April, 2016, the patient exhibited stable vital signs, without fever. She was then administered paclitaxel infusion as well as 1 g cefotiam every 12 hours as first empirical antibiotics. On 14 April, 2016, the fever had subsided, and the patient was discharged with a prescription for 100 mg cefixime two times daily for 7 days. On 20 April, 2016, the patient was admitted for the eleventh paclitaxel infusion, she did not exhibit any febrile events, probably because of medication with oral cefixime till admission. On 27 April, 2016, when she was admitted for the last dose of paclitaxel infusion, the leukocyte count was 2,620/mm3 (segmented neutrophils, 40.3%). After paclitaxel infusion through the chemoport, the body temperature was noted to be 38.3°C, and the patient experienced chills. Two sets of peripheral blood samples were collected from different venous sites, and the patient was started on an empirical antibiotic regimen of 4.5 g piperacillin–tazobactam every 8 hours. On 28 April, 2016, the C-reactive protein levels had increased remarkably to 7.56 mg/dl. She strongly insisted on discharge, and the previous chart and laboratory data were reviewed before arriving at a decision on discharge medication. The cultures of the two sets of peripheral blood samples collected on 12 April, 2016, exhibited R. aquatilis in 4 bottles. Although the automated system could distinguish the organism, it could not perform antibiotic susceptibility tests. Therefore, antimicrobial susceptibility was evaluated by the disc diffusion method. The organism presented susceptibility to several antibiotics (Table 1). On the basis of these results, the patient was prescribed 200 mg oral cefixime two times daily as discharge medication. She visited the outpatient clinic on 4 May, 2016, for retrieving the results of the culture test of blood samples collected on 27 April, 2016, which again exhibited R. aquatilis. This organism was found in two sets (three bottles – two anaerobic bottles and one aerobic bottle) which was drawn from two different peripheral venous sites. On that day, blood samples were collected from both the chemoport and the peripheral vein for evaluating the clearance of bacteremia. Transthoracic echocardiography were done to find out if there's any sign of infective endocarditis because two serial collections of blood culture revealed bacteremia with the same organism, R. aquatilis. No evidence of infective endocarditis was observed. The oral cefixime regimen was changed to 500 mg oral ciprofloxacin two times daily for two days. The chemoport was removed on 23 May, 2016, and swabbed for culture samples. The results of blood culture via chemoport performed on 28 April, 2016, and chemoport tip culture performed on 23 May, 2016, were negative. Throughout this event, sputum and urine samples were also subjected to culture tests; however, these samples did not exhibit any infective microorganisms. Recently, on 31 March, 2017, the patient received her eleventh dosage of herceptin, without any evidence of infection. The patient's clinical course is summarized on Figure 1.
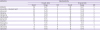
Table 1
Antibiotics sensitivity test of the Rahnella aquatilis from the blood cultures drawn on 12 April and 27 April, 2016

Discussion
R. aquatilis was first described in 1976 by Gavini and colleagues at Institut Pasteur. The name Rahnella is derived from the name of bacteriologist Otto Rahn, while “aquatilis” is derived from the Latin term for water [3]. The first clinical isolate of R. aquatilis was reported to the Center for Disease Control and Prevention in 1985 [4]. Most cases of R. aquatilis infection have been reported in compromised hosts or young children [5, 6]. A case of iatrogenic inoculation by contaminated intravenous fluid also been reported in a healthy adult [7]. The history of R. aquatilis since its discovery is relatively short; only a few pathological manifestations of the organism are understood, and it is confused with Pantoea agglomerans because of similarity in biochemical characteristics [8]. However, Rahnella does have a few characteristic traits and has now been included in commercial databases for easier detection in clinical and environmental samples. Currently, the VITEK, BBL Crystal ID, and API 20E systems include R. aquatilis in their databases, and identification of the organism is relatively easy [7]. To our knowledge, there are approximately 20 to 30 case reports of R. aquatilis infection in humans. Except for a few, most of these cases —including the present case— involve patients with diabetes mellitus, alcoholism, acquired immune deficiency syndrome, or cancer, which indicates that this organism might cause opportunistic infections. R. aquatilis has been isolated from blood, wound, urine, respiratory tract, and stool samples [5]. Although the origin of the R. aquatilis strain isolated from our patient is unclear, catheter related blood stream infection (CRBSI) was suspected clinically because fever and chill were developed in a patient with central venous catheter without any localizing sign [8]. Unfortunately, we could not get any definitive evidence of CRBSI. One possible reason is that appropriate blood culture – peripheral venous blood collection accompanied with central catheter blood collection – was not performed on febrile day. Another possible reason is that antibiotics was injected via chemoport before blood culture was drawn through a chemoport. Interestingly, the present patient performed farm work during chemotherapy, as a hobby to improve her well-being. Although we did not perform any epidemiological study at her farm, we suspect that fresh water near the farm could be the primary source of infection. Regarding the possibility that this was a nosocomial infection, the present case was the only one of R. aquatilis being isolated from clinical specimens at our hospital; therefore, we did not consider that this could be an outbreak, as seen in other case [9]. The present patient was treated with a short-term intravenous antibiotic regimen and a longer duration of oral antibiotic regimen, followed by removal of the chemoport after completion of her scheduled chemotherapy. Generally, R. aquatilis is known to possess a chromosomally encoded extended-spectrum antimicrobial resistance; for this reason, it is recommended to avoid beta-lactam-based treatment regimens, with the exception of some active agents. However, an R. aquatilis strain with sensitivity towards beta-lactam antibiotics has been isolated in specimens from a surgical wound [10]; the isolate in the present case, too, exhibited similar drug sensitivity characteristics. R. aquatils has also been reported to exhibit sensitivity towards quinolones, carbapenems, and trimethoprim–sulfamethoxazole, which, therefore, appear to be attractive treatment choices [11]. Although R. aquatilis is an environmental organism, underestimating the importance its discovery in clinical culture specimens might be dangerous because of its ability to cause diseases and even sepsis [12-14]. Since the chances of exposure to R. aquatilis are relatively high, its significance in public health should not be underestimated [15]. At the time of this publication, there were no reports of Rahnella-associated mortality.
 XML Download
XML Download