

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Urinary tract infections (UTIs) are one of the most common bacterial infections and are caused by both Gram-negative and Gram-positive bacterium [1]. Also, UTIs are one of the major healthcare-associated infections (HAIs) [2] and account for up to 32% of all HAIs [3]. HAIs are a major concern for patient safety and can result in prolonged hospital stay, increased morbidity and mortality, increased antimicrobial resistance, and excess financial burden [4]. UTIs are mostly complicated with various predisposing factors [5]. In more than 80% of the cases, they are related to the use of urologic devices including foley catheters [6], and according to risk factors and clinical settings, there are several described uropathogens [7]. E. coli is reported as the most common pathogen of UTIs, followed by the second most common, K. pneumonia [8]. In a multicenter study of bacteremic UTIs performed in Korea, the proportions of E. coli and K. pneumoniae infections were 71.8% in healthcare-associated UTIs and 89.9% in community-onset UTIs [89]. Although several studies have described the characteristics of uropathogenic E. coli and K. pneumoniae individually [1011], there are only few studies comparing clinical characteristics between these two pathogens, especially studies comparing them in UTIs. Also, increased antimicrobial resistance in Enterobacteriaceae is a global concern [121314]. The aim of this study was to compare the predisposing factors, clinical characteristics, treatment outcomes, and antimicrobial susceptibility profiles between acute pyelonephritis (APN) caused by E. coli and K. pneumoniae.
Materials and Methods
1. Study subjects
Patients with monomicrobial APN who were admitted at Keimyung University Dongsan Medical Center between January 2014 to December 2017 with E. coli or K. pneumoniae isolated from clinical specimens were enrolled in this study. They were divided into two groups, labeled as E. coli and K. pneumoniae. Asymptomatic bacteriuria was excluded.
APN was defined as one or more of the followings: 1) the presence of fever (body temperature above 38°C), pyuria and bacteriuria with urinary symptoms, flank pain, and tenderness of costovertebral angle, 2) although there were no specific symptoms or signs of UTI, APN was identified in the radiologic findings with fever or leukocytosis, and there was no other focus of infection [15]. Obstructive uropathy included benign prostate hypertrophy (BPH) and uterine prolapse. Severe APN was determined as severe sepsis or shock due to APN. Recurrent UTI was defined as defined as ≥3 microbiologically documented episodes of symptomatic UTI during the last year or 2 episodes during the last 6 months. HAI was defined as a nosocomial infection (clinical symptoms of infection occurred 48 hours after hospital admission) or community onset infections with healthcare-associated risk factors, such as hospitalization within 90 days, received dialysis, taken intravenous medication in outpatient clinics, or resided in long-term care facilities. An invasive procedure was considered a medical procedure that invades the body, usually puncturing the skin and inserting prosthesis or aspirating, such as percutaneous needle aspiration, percutaneous nephrostomy, or percutaneous pus drainage. Patients who were under 18 years old or transferred to other hospitals during treatment were excluded.
Medical records, including epidemiology, underlying diseases, predisposing factors, previous antibiotic use, clinical characteristics, antimicrobial susceptibility profile, and treatment outcomes, were retrospectively analyzed. Severity of comorbidity was classified based on McCabe and Jackson score system; nonfatal underlying disease, ultimately fatal disease, and rapidly fatal disease. Diabetes or genitourinary, and gastrointestinal diseases were included in nonfatal diseases. Ultimately fatal diseases were defined as estimated to become fatal within 4 years, such as aplastic anemia, chronic leukemia, lymphomas, metastatic carcinomas, and severe heart failure. Acute leukemia or blastic relapse of chronic leukemia were included in rapidly fatal disease [16]. Empirical antibiotic treatment and antibiotic adequacy were compared and analyzed between the two groups. The treatment outcomes were evaluated by the defervescence within 72 hours after empirical antibiotics, 30-day mortality, infection-related 30-day mortality, acute kidney injury, need for invasive procedure, and recurrence of UTI within 3 months. Infection-related 30-day mortality was defined as patients expired due to UTI or complications of UTI within 30 days. If the patients were discharged from hospital after admission within 30 days, we followed up the patients over 1 months at outpatient clinic. Acute kidney injury was defined as an increase in serum creatinine by >0.3 mg/dL within 48 hours, or an increase in serum creatinine to >1.5 times the baseline, or urine volume <0.5 mL/kg/hour for 6 hours.
Clinical specimens, such as blood, urine, and pus were obtained for identification of microorganisms. E. coli or K. pneumoniae isolation was performed using a Vitek system (BioMerieux, Lyon, France). Antimicrobial susceptibility profile was determined by the interpretation of the breakpoints recommended by the Clinical and Laboratory Standards Institute (CLSI) [17]. The study was approved by the Institutional Review Board of Dongsan Medical Center (IRB 2015-11-043).
2. Statistical methods
Statistical analysis was performed using SPSS version 21.0 (IBM Co., Armonk, NY, USA). Categorical variables were compared using the Pearson chi-square test or Fisher exact test. Continuous variables were compared using the Mann-Whitney U test or Student t test. Binary logistic regression was used to identify variables significantly associated with K. pneumoniae infection compared to E. coli. Statistical significance was defined as P values <0.05.
Results
A total of 341 patients were diagnosed with APN, with E. coli or K. pneumoniae isolation in clinical specimens during the study period; 266/341 were cases of E. coli and 75/341 of K. pneumoniae. Eight patients with E. coli and four patients with K. pneumoniae infections were excluded because they were transferred to another hospital during treatment, attaining of a total of 329 patients with APN; 258/329 were cases of E. coli and 71/329 were cases of K. pneumoniae. Among them, 219 patients were classified into community-onset APN; 194/219 cases of E. coli and 25/219 cases of K. pneumoniae infections and 110 patients were classified into healthcare-associated APN; 64/110 cases of E. coli and 46/110 cases of K. pneumoniae infections (Fig. 1).
Figure 1
Flow chart showing the number of patients enrollment in this study.
APN, acute pyelonephritis; CO, community-onset; HA, healthcare-associated.

1. Baseline epidemiology, predisposing factors, and clinical characteristics between Escherichia coli and Klebsiella pneumoniae
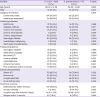
The demographics, category of infections, underlying diseases, and predisposing factors of the two groups are shown in Table 1. Mean age was higher in E. coli group than in K. pneumoniae. Males were more observed in K. pneumoniae group. In category of infection, community-onset APN was more observed in E. coli, whereas healthcare-associated APN was more observed in K. pneumoniae. Underlying diseases except neurologic diseases and solid organ transplantations showed no differences between the two groups. Urinary tract stone, recurrent UTI and bacteremia were more associated with E. coli. Urinary catheter use and complicated APN were more associated with K. pneumoniae.
Table 1
Comparison of baseline characteristics, predisposing factors, clinical characteristics, and treatment outcome of acute pyelonephritis between Esherichia coli and Klebsiella pneumoniae
2. Comparison of baseline epidemiology and clinical characteristics between Escherichia coli and Klebsiella pneumoniae healthcare-associated APN
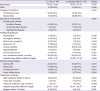
The baseline characteristics, category of infections, predisposing factors, and clinical characteristics in healthcare-associated APN were shown in Table 2. In category of infection, community-onset infections with healthcare-associated risk factors and nosocomial infections were 52 cases (81.2%), 12 cases (18.8%) in E. coli group and 16 cases (30.4%), 32 cases (69.6%) in K. pneumoniae group, respectively. Hospital stays before infection were 0.02 days in E. coli group and 27.80 days in K. pneumoniae (P = 0.005). There were no significant differences in underlying systemic diseases between the two groups. Ultimately fatal diseases were more observed in K. pneumoniae group. Prior usage of antibiotics within 3 months was not different between the two groups. There were no significant differences in the kinds of previously used antibiotic; piperacillin/tazobactam (15.8% vs. 35.0%, P = 0.111), third cephalosporin (60.5% vs. 40.0%, P = 0.136), fluoroquinolone (44.7% vs. 40.0%, P = 0.729) and carbapenem (15.8% vs. 30.0%, P = 0.307). Recurrent UTI was more frequently observed in E. coli together with neurogenic bladder, and obstructive uropathy. Urinary catheter use was more associated to K. pneumoniae infection. Presence of urinary tract stone was associated to E. coli and the same was observed for hydronephrosis without significance. Abscess formation showed no significant differences between the two groups. Renal abscesses were combined in five cases in E. coli group (7.8%) and three in K. pneumoniae group (6.5%). Prostatic abscesses were combined in two cases in E. coli group (3.1%). Finally, severe APN and bacteremic APN were more associated with E. coli infection (Table 2).
Table 2
Comparison of clinical characteristics and treatment outcomes between Escherichia coli and K. pneumoniae healthcare-associated acute pyelonephritis
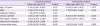
In multivariate analysis, urinary catheter use was more associated with K. pneumoniae than E. coli infection (Table 3). Age over 65 years (odds ratio [OR] 2.112, 95% confidence intervals [CI] 1.142-3.906, P = 0.017) and neurogenic bladder (OR 3.765, 95% CI 1.112-12.772, P = 0.033) were more associated with E. coli infection.
Table 3
Predisposing factors associated with Klebsiella pneumoniae compared to Escherichia coli in acute pyelonephritis
3. Comparison of antimicrobial susceptibility rates between Escherichia coli and Klebsiella pneumoniae
Comparisons of antimicrobial susceptibility rates between E. coli and K. pneumoniae were shown in Table 4.
Table 4
Comparison of antimicrobial susceptibility between Escherichia coli and Klebsiella pneumoniae
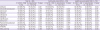
In total cases, ESBL positivity was no significant differences between E. coli and K. pneumoniae group. Piperacillin/tazobactam and tigecycline were more sensitive to E. coli than K. pneumoniae. Whereas, ciprofloxacin and gentamicin were more sensitive to K. pneumoniae than E. coli.
In community-onset APN, ESBL positivity were observed in 29.0% of E. coli and 8.0% of K. pneumoniae. Amoxicillin/clavulanate, aztreonam, cefazolin, ceftazidime, cefepime, and ciprofloxacin were more sensitive to E. coli than K. pneumoniae. Piperacillin/tazobactam showed similar antimicrobial susceptibility rate, 93.3% in E. coli and 96.0% in K. pneumoniae.
In healthcare-associated APN, K. pneumoniae group was more sensitive to ciprofloxacin and gentamicin while E. coli group was more sensitive to piperacillin/tazobactam and tigecycline. ESBL productions were observed in 48 cases of E. coli (75.0%) and 30 cases of K. pneumoniae (65.2%) infection. Among the pathogens confirmed as ESBL-producing, E. coli was more susceptible to piperacillin/tazobactam (75.0% vs. 46.7%, P = 0.011) and K. pneumoniae to ciprofloxacin (10.4% vs. 36.7%, P = 0.005). Susceptibility to trimethoprim/sulfamethoxazole showed no significant differences between the two groups (35.4% vs. 33.3%, P = 0.851) (Table 5).
Table 5
Comparison of antimicrobial susceptibility between extended spectrum-β lactamase producing Escherichia coli and Klebsiella pneumoniae in healthcare-associated acute pyelonephritis
In subgroup analysis of 104 cases of APN with ESBL producing E. coli, percentages of community-onset APN, community-onset APN with healthcare associated risk factors, and nosocomial APN were 53.8%, 37.5%, 8.7%, respectively. In 32 cases of APN with ESBL producing K. pneumoniae, the percentages were 6.2%, 21.9%, and 71.9%, respectively (P = 0.001).
4. Comparisons of empirical antibiotics, antibiotic adequacy, and treatment outcomes between the two groups
In community-onset APN, 3rd-generation cephalosporins were the most commonly used empirical antibiotics in both groups (90.2% vs. 80.0%, P = 0.164), followed by carbapenem (6.2% vs. 12.0%, P = 0.389). One hundred thirty-seven cases of E. coli and 24 cases of K. pneumoniae were treated using concordant antibiotics. The adequacy of empirical antibiotics showed 70.6% in E.coli and 96.0% in K. pneumoniae group (P = 0.007).
No significant differences between the two groups were observed in the cases with defervescence within 72 hours (75.8% vs. 84.0%, P = 0.360) and acute kidney injury (15.5% vs. 24.0%, P = 0.263). Hospital stay after infection was longer in E. coli than in K. pneumoniae group (12.46 days vs. 10.48 days, P = 0.187). Thirty-day mortality (0.5% vs. 4.0%, P = 0.216) and infection related 30-day mortality (0.0% vs. 6.2%, P = 0.076) showed no significant differences between the two groups. Relapsed UTI within 3 months was more commonly observed in K. pneumoniae when compared to E. coli group with no significance (5.2% vs. 12.0%, P = 0.376).
In healthcare-associated APN, 3rd-generation cephalosporins were the most commonly used empirical antibiotics in both groups (62.5% vs. 47.7%, P = 0.128), followed by carbapenem (28.1% vs. 27.3%, P = 0.923). Thirty-seven cases of E. coli (57.8%) were treated using concordant antibiotics and 27 cases using discordant antibiotics. Considering these 27 discordant cases, the treatment was modified to definitive antibiotics during hospitalization and 24/27 cases (88.8%) were modified within 72 hours. Thirty cases of K. pneumoniae (60%) were treated using concordant antibiotics, and 20 cases using discordant antibiotics. Among them, 18/20 (90.0%) cases were modified to definitive antibiotics and 15/20 cases (75.0%) were modified within 72 hours. Comparison of the adequacy of empirical antibiotics showed no significant differences between the two groups (P = 0.617). The duration of antimicrobial treatment was longer in the E. coli group than in the K. pneumoniae group (21.4 days vs. 15.6 days, P = 0.003).
Need for an invasive procedure was observed in 12.5% of E. coli cases and 4.0% of K. pneumoniae cases with no significance (P = 0.182). No significant differences between the two groups were observed in the cases with defervescence within 72 hours and acute kidney injury (Table 5). Hospital stay after infection was longer in K. pneumoniae than in E. coli group (20.2 days vs. 26.1 days, P = 0.124). Thirty-day mortality was significantly higher in K. pneumoniae group. However, infection-related 30-day mortality showed no significant difference between the two groups. Relapsed UTI within 3 months was more commonly observed in E. coli when compared to K. pneumoniae group with no significance (15.6% vs. 6.0%, P = 0.109).
Relapses within 3 months, infection related 30-day mortality, and defervescences within 72 hours showed no significant differences according to adequacy of empirical antibiotics.
Discussion
E. coli and K. pneumoniae are two of the most common pathogens associated with high morbidity and mortality among Gram-negative bacilli, especially in UTI [18]. The etiologies of UTI were diverse according to regions and countries, and dependent on the severity of complications; E. coli was the most common, followed by K. pneumonia [671920]. Baizet et al. reported that E. coli was the most common pathogen in cystitis, pyelonephritis in females, and upper UTI in male. K. pneumoniae was the second most common pathogen in pyelonephritis in females and upper UTI in males [19]. Comparisons of clinical characteristics between E. coli and K. pneumoniae had been presented in many reports [1921]; however, comparative studies regarding the differences in antimicrobial resistance rates and predisposing factors between the two strains were rare. In this study, we compared clinical characteristics, treatment outcomes, and determined the antimicrobial susceptibility profiles of UTI between E. coli and K. pneumoniae.
K. pneumoniae was more associated with urinary catheter use in this study. In healthcare-associated UTI, most cases were associated with urinary catheter use [567]. Oh et al. reported that patients with catheter-associated UTI had diverse pathogens according to different kinds and indwelling duration of urinary catheter (intermittent, short-term, and long-term catheterization) [7]. Indeed, urinary catheters serve as common predisposing substrates of UTIs. Maharhan et al. reported that E. coli was the most common biofilm-forming bacteria in catheter-associated UTI [22]. Biofilm-forming mechanisms can be different according to the pathogen. Uropathogens, such as K. pneumoniae and Proteus mirabilis produce urease and form crystalline biofilms on urinary catheters. Urease production can break down the urea, release ammonia, and increase urine pH and calcium magnesium phosphate crystal formation within the biofilm matrix. Crystal formation can block the catheter and lead to bladder distension, urine leakage, and bladder reflux into the kidney [23]. Uropathogenic E. coli have different mechanisms for biofilm formation; several virulence factors, such as a-hemolysin, lipopolysaccharide, protease, adhesins, aerobactin, and fimbriae, have important roles in forming the biofilm. Among several virulence factors, type I fimbriae play an important role in the attachment to the mucosal epithelium, initiation of biofilm formation, and persistence in the bladder [24]. Besides, biofilm production can increase resistance to antibiotics and virulence [25]. Unlike previous studies, we determined that K. pneumoniae was more associated with urinary catheter use than E. coli. Further research will be necessary to determine whether there are differences between these two pathogens in biofilm formation.
Along with biofilm formation, residual urine after voiding is a risk factor for UTI. E. coli was significantly associated with neurogenic bladder in this study. The probability of UTI appearance can increase in proportion to the residual volume of urine. Residual urine volume greater than 100 mL resulted in a 4.9-fold increase in UTI occurrence compared to those with residual volume less than 100 mL [26]. Furthermore, increased intravesical pressure results in bladder ischemia and delayed immune response to uropathogens. Additionally, neurogenic bladder, especially in patients with spinal cord injury, might lead to immune dysfunctions, such as decreased proinflammatory and anti-inflammatory responses to uropathogens. Therefore, uropathogens, such as E. coli and K. pneumoniae may not be easily eradicated with antibiotics when invading urothelial cells during acute UTI and proliferating within the urothelium [27].
In addition, urinary tract stone and obstructive uropathy were more frequently observed in E. coli infection in this study. Obstructive uropathy, such as BPH in men and uterine prolapse in women, can cause a physiologic blockage of the urethra and bladder outlet resulting in urinary stasis. In the same way, ureteral obstruction caused by urinary tract stones can prompt urinary stasis and renal dysfunction. As a result, urinary stasis can induce adherence of bacteria and invasion to the urogenital epithelium [28]. Chen et al. reported that the four most common uropathogens isolated from patients with urinary stones were E. coli, K. pneumoniae, P. mirabilis and Enterococcus faecalis [29].
Megged et al. compared bacteremic UTI to non-bacteremic UTI. Patients with bacteremic UTI were more associated with male, higher creatinine levels, and underlying urologic conditions other than non-bacteremic UTI [30]. Oh et al. proposed a model to estimate the probability of bacteremia in UTI. Risk factors of bacteremia were diabetes mellitus, urinary tract stone, tenderness of costovertebral angle, azotemia, neutrophilia, and thrombocytopenia [31]. In the present study, bacteremic UTI was more associated with E. coli. Furthermore, E. coli was more associated with male sex, neurogenic bladder, and presence of urinary tract stone. These factors might lead to a higher incidence of bacteremia in E. coli infection.
Recently, antimicrobial resistance in Gram-negative bacteria has been gradually increasing worldwide [12]. In Bangladesh, antimicrobial resistance rates to third-generation cephalosporins in Enterobacteriaceae were over 50% in UTI, including community-onset and healthcare-associated infections [13]. In the present study, the proportions of ESBL production were 29.0% in E. coli and 8.0% in K. pneumoniae in community-onset APN. Also, over 30% of E. coli in community-onset APN were resistant to ciprofloxacin. Ciprofloxacin or 3rd generation cephalosporin is recommended as empirical antibiotics for community-onset APN. In a report of community-onset UTI conducted in United Arab Emirates, 76% of E. coli and K. pneumoniae were ESBL producers [14]. Based on the present and previous study results, antibiotic resistance in community can be a global concern in the near future. Besides, 60-70% isolates of E. coli and K. pneumoniae in healthcare-associated UTI were resistant to third- and fourth-generation cephalosporins in the present study. In addition, in a report conducted in Turkey, ESBL production was detected in 82.8% of K. pneumoniae and 72.9% of E. coli cases in pediatric patients with nosocomial UTI [32]. Extended-spectrum cephalosporins, such as ceftazidime or cefepime, were recommended as empirical antibiotics for healthcare-associated UTI [33]. Based on present and previous study results about antimicrobial resistance of Enterobacteriaceae, we think that it is difficult to recommend third- or fourth-generation cephalosporins as an empirical antibiotic in healthcare-associated UTI because of higher resistance development. Instead, piperacillin/tazobactam, carbapenem, and amikacin were relatively effective in both bacteria.
A study by Scheurman et al. reported that acquisitions of ESBL-producing Enterobacteriaceae bloodstream infections were more observed in nosocomial and community-onset healthcare-associated infections [34]. Subgroup analysis of our study shows that ESBL-producing E. coli was relatively high in community-onset APN than K. pneumoniae. The discrepancy of these two studies might be due to difference of sources of bacteremia and composition of community and healthcare-associated infections. Also, resistance of these bacteria has been changed over the times from the mentioned study. For these reasons, high ESBL positivity of E. coli in community-onset APN might be presented in our study.
There are several limitations to this study. First, this study was retrospective and relied on microbiological culture results, which may introduce bias in the data interpretation. Second, we had to rely only on medical records. Third, we could not identify the different kinds of urinary catheters and duration of indwelling catheters. Additionally, it was difficult to evaluate urinary function or identify the subjective symptoms of discomfort during urination in all patients. Fourth, we should acknowledge that patients included in this study were in a tertiary hospital and might be in a more severe state than those in a primary medical center.
Despite these limitations, we found the characteristics of predisposing factors, clinical manifestations, and antimicrobial susceptibility of E. coli and K. pneumoniae in healthcare-associated UTI in a tertiary hospital setting in South Korea. Common causative pathogens of healthcare-associated UTI can be diverse according to region and country. Additionally, antimicrobial susceptibility can be different according to local antimicrobial resistance pattern and history of previous antibiotics use. Therefore, further multicenter studies regarding antimicrobial susceptibility and clinical characteristics of uropathogens in healthcare-associated UTI will be needed to identify the epidemiology of uropathogens and antimicrobial susceptibility in our country.
In conclusions, K. pneumoniae was more associated with urinary catheter use, and E. coli was more associated with an anatomical or functional urologic problem. E. coli was more associated with bacteremic UTI and severe UTI. Antimicrobial susceptibility test revealed that ESBL producing E. coli were more observed than K. pneumoniae in community-onset APN and antimicrobial resistant rates of third- and fourth-generation cephalosporins were high in both E. coli and K. pneumoniae in healthcare-associated APN.
 XML Download
XML Download